

Approaching Death: Improving Care at the End of Life (1997)
Chapter: 10 conclusions and recommendations, 10 conclusions and recommendations.
Our lives are time travel, moving in one direction only. We accompany one another as long as we can; as long as time grants us.
Joyce Carol Oates, A Letter to My Mother , 1996
We go toward something that is not yet.
Paul Tillich, The Eternal Now , 1959
Dying is at once a fact of life and a profound mystery. Death comes to all, yet each person experiences it in ways that are only partly accessible to the family member or physician, the researcher or philosopher. In principle, humane and skillful care for the dying is a social obligation as well as a personal offering from those directly involved. In reality, both society and individuals fall short of what is reasonably, if not simply, achievable.
Evidence and experience both indicate that much dying is far harder than it should be. Like the mythic king Tantalus, who reached for fruit and water just beyond his grasp, the dying person has too often been destined to seek but not find a pain-free and peaceful death. Such a fate need not be; better deaths are possible now.
This is not to claim that dying and death can be made easy, although certain illnesses tend to bring less-difficult deaths than others; nor is it to suggest that caring well for those approaching death can be made an exact science or flawless art. Caring well involves a frequently stressful, imperfect effort to balance science with sentiment, honesty with hope, patterns of care with room for exceptions.
This report has identified ways in which clinicians, educators, and communities do not care adequately for those approaching death. It has pointed to steps that can improve care at the end of life and sustain improvements through difficult times. It has also highlighted the reasons for believing that professionals, policymakers, and the public are ready to support such steps. These reasons range from the examples of well-known men and women facing death with grace to the focus on deficiencies in care
stimulated by the debate over assisted suicide. In sum, the timing appears right to press for a vigorous societal commitment to improve care for the dying. Such a commitment would motivate and sustain local and national efforts to strengthen and apply the existing knowledge base, reform procedures and policies that impede good care for the dying, and stress the caring functions of health delivery systems.
Today and Tomorrow
The preceding chapters have profiled important aspects of dying in America. They have noted that three-fourths of those who die are elderly and that most people who die are covered by Medicare or other federal, state, or local programs for older, disabled, or impoverished people. Compared to earlier times, death now comes more often in old age from a chronic or progressive disease. Most deaths occur in institutions, mainly hospitals and, to a lesser extent, nursing homes. The proportion of people who die at home is, however, increasing. Only a minority of all deaths involve people cared for by formal hospice programs, and the majority of these involve cancer diagnoses. All patients can potentially benefit from good palliative care, but hospice programs as organized and financed in the United States are most applicable to those with relatively predictable prognoses.
Although specifics may vary according to the nature of a person's disease and his or her personal circumstances, care for dying people and those close to them has several broad dimensions: physical, psychological, spiritual, and practical. Each of these dimensions is intertwined in the key processes of care, which include determining and communicating diagnosis and prognosis, establishing goals and plans, and fitting palliative and other care to these goals. The way care is organized, financed, monitored, and regulated affects how these processes are carried out in different settings for different kinds of patients.
The twenty-first century will bring new realities as well as continuing problems and opportunities in care at the end of life. It will undoubtedly deliver improvements in what medical science can do to prevent and relieve distress for those approaching death, but demographic, economic, and other trends will strain systems that already find it difficult to deliver what clinical knowledge currently allows—and what compassion should grant.
The committee focused primarily on trends and expectations relevant to care for dying patients during the next 10 to 20 years. One of these expectations is that policymakers and others will need to prepare during this period for the final demographic consequences of the post-World War II baby boom. The oldest members of the baby boom generation will reach age 65 in the year 2011, and the youngest members will do so nearly 20
years later. Barring dramatic unexpected developments, older adults will constitute a larger proportion of the population than today, and the absolute numbers of dying patients will be much larger. In the face of an ever-increasing population with chronic conditions, the current system, with its emphasis on acute curative care, will fail to provide needed long-term chronic care and palliative and support services. Although health care and social service providers have a long lead time compared with the educators and communities who had to scramble to provide schooling for the baby boom generation, the difficulties that policymakers are having with Social Security and Medicare do not bode well for the nation's ability to cope with an aging population.
In addition, continuing increases in longevity will mean that the proportion of those dying past age 75 will increase. The impact on the health care system and society on larger numbers of people dying in older old age will depend in part on their health status in the years before death. The "compression of morbidity hypothesis," for which the evidence is ambiguous, posits that an increase in healthier life styles means that people will experience disabling conditions for a smaller proportion of the years before death than today. Even if this does occur, the overall impact of the larger proportion of older people and their longer life span will still pose enormous challenges for social and health care systems.
Demographic politics are likely to be complex in coming years. On the one hand, the so-called senior lobby should be strengthened by the "baby boom" cohort. The "baby boomers," throughout their childhood, youth, and early middle age, have drawn public attention to their needs and concerns. On the other hand, the burden on the smaller working-age population of supporting its elders raises the specter of a generational backlash (even though younger people could also be burdened if the social support available to their aging parents is reduced). Such a backlash could take many forms, including means-testing Social Security benefits or less sympathy for supportive services for frail elderly people, those with serious disabilities, and people who are dying.
Cultural trends add further complexity to demographic politics. Immigrants, who tend to be young and have more children than native-born Americans, have been a major source of growth in the total U.S. population (NRC, 1997). Nonhispanic Caucasians—now a majority—are a decreasing proportion of the U.S. population. Thus, the large elderly population in the first decades of the next century will be dependent on a smaller and more culturally diverse population of younger people.
As described in preceding chapters, health care in the United States is undergoing major changes. The use of hospital services has dropped significantly, and further declines are likely, particularly in those areas with continued relatively high rates of use. Hospital care will likely be less available
to dying patients, potentially including some who could benefit from such care as well as many who will do better with alternatives.
Despite indications that health care spending increases have moderated from years past, the pressure to cut health care costs does not appear to be abating. In particular, given the bleak financial picture for Medicare and the significant portion of spending accounted for by beneficiaries in their last year of life, these constraints may be manifested in some degree of age-based rationing. That is, older people could be denied services simply because of their age, without regard to their life expectancies, function, or expected benefit from care. Decreased access to advanced technologies intended to prolong life could be a highly visible issue, although it is relatively unimportant for the great majority of those dying at an advanced age.
If successful, increased efforts to shift Medicare beneficiaries into various forms of managed care will test these entities, whose enrollment now is overwhelmingly concentrated in younger, healthier age groups. Potential problem areas include payment, contracting, and utilization review mechanisms that limit access to clinicians and care teams experienced in palliative care, patient scheduling norms that limit time for careful clinician-patient communication, marketing strategies intended to discourage enrollment or encourage disenrollment by seriously ill people, drug formularies that exclude or restrict important medications, and bureaucratic hurdles that discourage people from seeking care or preclude them from receiving requested services. One characteristic of many managed care organizations is an emphasis on moving more responsibility for diagnosis and patient management to primary care clinicians, including nurse practitioners, nurses, and other nonphysicians. How well this will work for seriously ill and elderly patients is not yet clear. A major role for nurses and other health care professionals is, however, already well tested in hospice, social health maintenance organizations, and other settings that care for patients dying of advanced progressive diseases, particularly cancer, and for frail elderly people.
As well as focusing attention on competing ethical and policy values, this prospect of constrained resources underscores the need for more valid and reliable tools for assessing health status, measuring outcomes, and linking them to health interventions. Considerable progress is being made in this arena. In addition, improved computer-based information and decision support systems promise several benefits. At the level of the individual, they will help patients, families, and clinicians in making more informed decisions about care at the end of life. At the system or societal level, they will strengthen structures and processes of accountability involving health care providers, purchasers, patient/consumers, and public officials.
Moreover, advanced information and communications technologies may make health care more accessible for some who face geographic or
other barriers to care. Although the potential for practical, effective, and affordable "medicine at a distance" is more promised than proved, telemedicine could help bring palliative and other expertise and services to homes, nursing homes, and other places where they are not very available today (IOM, 1996e). People who have chronic and advanced illnesses but do not qualify for hospital inpatient care could benefit.
Findings and Recommendations
Although the committee found many problems, it also found much that was good and improving in care for those approaching death. It was impressed by the principles, aspirations, and practices being advanced by the field of palliative medicine and being implemented or attempted through interdisciplinary care teams in varied settings, including hospices, hospitals, nursing homes, and private homes. More effort is now being devoted to understanding differences in people's paths toward death and developing programs that are flexible enough to accommodate these differences. In addition to dedicated professionals, many volunteers contribute their time and energy to provide emotional and practical support to dying patients and those close to them. People from a variety of backgrounds have also joined together to direct the attention of policymakers and ordinary citizens to the need to remove barriers to good care created by laws, regulations, organizational practices, and lack of supportive community resources.
Care for the dying should also benefit from ongoing efforts to improve continuity of care, strengthen information systems, prevent health problems, and create accountability for the quality of care. The developing fields of outcomes measurement can make important contributions to the care of the dying by teaching us how to conceptualize and measure quality of life and well-being for those approaching death. Quality improvement strategies are helping to identify and remedy system problems that impede good care. The committee is encouraged by the growing interest in end-of-life issues as recently evidenced by the publication of books and articles for lay and professional audiences, the commitment of foundation resources to support research and education, and the organization of conferences, working groups, and other initiatives sponsored by professional societies and others.
Deficiencies in Care at the End of Life
Notwithstanding these positive features, the committee concluded that very serious problems remain. Indeed, in this committee's view, if physician and hospital performance in infection control were as poor as it is, for
example, in pain management, the ensuing national outcry would create an immediate demand for responses from clinicians, managers, and educators.
The committee identified four broad deficiencies in the current care of people with life-threatening and incurable illnesses. First , too many people suffer needlessly at the end of life both from errors of omission—when caregivers fail to provide palliative and supportive care known to be effective—and from errors of commission—when caregivers do what is known to be ineffective and even harmful. As reported in Chapter 3 , studies have repeatedly indicated that a significant proportion of dying patients and patients with advanced disease experience serious pain, despite research identifying a range of effective pharmacological and other options for relieving most pain. Other symptoms are less well studied, and more research on symptom prevalence and management is needed, but the information available to the committee suggested similar care problems. Deficiencies in the application of existing knowledge to prevent and manage pain and other distressing symptoms stem from an unfortunate mix of ignorance about effective pharmacological and other interventions, misplaced concern about opioid addiction, and inadequate attention to people's quality of life while dying. These problems are reinforced by care systems that are not structured to provide the clinical expertise, reliability, continuity, and emotional support needed by people approaching death. Cultural biases and fears about illness, disability, and death may also contribute to avoidance of dying patients and those close to them.
In perverse counterpoint to the problem of undertreatment, the aggressive use of ineffectual and intrusive interventions may prolong and disfigure the period of dying. Some of this care is knowingly accepted; some is provided counter to patients' wishes; much is probably provided and accepted with little knowledge or consideration of its probable benefits and burdens. Medical culture still tolerates and even rewards the misapplication of life-sustaining technologies while slighting the prevention and relief of suffering.
Second , legal, organizational, and economic obstacles conspire to obstruct reliably excellent care at the end of life. Despite some reforms, outdated and scientifically flawed drug-prescribing laws, regulations, and interpretations by state medical boards still frustrate and intimidate physicians who wish to relieve their patients' pain. Addiction to appropriately prescribed opioids is virtually nonexistent whereas their underprescription for pain is well documented. Organizational structures often interfere with the coordination and continuity of care and impede the further development and application of palliative care strategies in patient care, professional education, and research.
Financial incentives also discourage health care practitioners and providers from rearranging care so that it serves dying patients well. Tradi-
tional financing mechanisms—including arrangements based on discounted fees—provide incentives for the overuse of procedural services and the under-provision of the assessment, evaluation, management, and supportive services so important for people with serious chronic or progressive medical problems. Medicare hospice benefits have helped fill gaps for a small segment of dying patients, but many more have conditions that do not readily fit the current hospice model or requirements. Alternatives to fee-for-service financing in combination with restrictive administrative practices pose different potential hazards that are largely unstudied as they affect seriously and incurably ill people.
Third , the education and training of physicians and other health care professionals fails to provide them with the knowledge, skills, and attitudes required to care well for the dying patient. Many deficiencies in practice stem from fundamental prior failures in professional education. Despite encouraging signs of change, most clinicians-in-training experience and learn too little of the caring that helps people to live well while dying. Undergraduate, graduate, and continuing medical education do not sufficiently prepare health professionals to recognize the final phases of illnesses, construct effective strategies for care, communicate with patients and those close to them, and understand and manage their own emotional reactions to death and dying.
Fourth , current knowledge and understanding are inadequate to guide and support the consistent practice of evidence-based medicine at the end of life. In addition to existing knowledge not being well used, we still know too little about how people die; how they want to die; and how different kinds of physical, emotional, and spiritual care might better serve the dying and those close to them. Biomedical and clinical research have emphasized the development of knowledge that contributes to the prevention, detection, or cure of disease and to the prolongation of life. Research on the end stages of diseases and the physiological bases of symptoms and symptom relief has been less well supported. Epidemiological and health services research has likewise not provided a strong base for understanding the degree to which people suffer symptoms (except, perhaps, cancer pain), experience death alone rather than in the company of those who care, comprehend diagnostic and prognostic information, and achieve a dying that is reasonably consistent with their preferences, community norms, and palliative care principles. Methods development is important to define and measure outcomes other than death (including patient and family perceptions) and to monitor and improve the quality of care for those approaching death.
More generally, it seems that this nation has not yet discovered how to talk realistically but comfortably about the end of life, nor has it learned how to value the period of dying as it is now experienced by most people.
For most of human history, death came fairly quickly in childhood or at adult ages that today seem relatively young. As the twentieth century ends, most people in economically advanced countries live fairly healthy lives into older age but then experience progressive disability for some time before they die. Except what can be inferred from newspaper obituary pages, this reality is largely shunned by the news, information, and entertainment media as distasteful or uninteresting. One result is an unhelpful combination of public fear, misinformation, and oversimplification that views misery as inescapable, pain as unavoidable, and public spending as misdirected for people who are approaching death.
Recommendations and Future Directions
The committee developed seven recommendations directed at different decisionmakers and different deficiencies in care at the end of life. These recommendations and a brief explanation follow. Each applies generally to people approaching death, including those for whom death is imminent and those with serious, eventually fatal illnesses who may live for some time.
RECOMMENDATION 1: People with advanced, potentially fatal illnesses and those close to them should be able to expect and receive reliable, skillful, and supportive care . Educating people about care at the end of life is a critical responsibility of physicians, hospitals, hospices, support groups, public programs, and media. Most patients and families need information not only about diagnosis and prognosis but also about what support and what outcomes they should reasonably be able to anticipate. They should, for example, not be allowed to believe that pain is inevitable or that supportive care is incompatible with continuing efforts to diagnose and treat. They should learn—before their last few days of life—that supportive services are available from hospices and elsewhere in the community and that those involved in their care will help arrange such services. Patient and family expectations and understanding will be aided by advance care planning that considers needs and goals, identifies appropriate surrogate decisionmakers, and avoids narrow preoccupation with written directives. To these ends, health care organizations and other relevant parties should adopt policies regarding information, education, and assistance related to end-of-life decisions and services. For those who seek to build public understanding of dying as a part of life and to generate public demand for reliable and effective supportive services, one model can be found in the perspectives, spirit, and strategies that have guided efforts to promote effective prenatal care and develop mother- and family-oriented arrangements for childbirth.
RECOMMENDATION 2: Physicians, nurses, social workers, and other health professionals must commit themselves to improving care for dying patients and to using existing knowledge effectively to prevent and relieve pain and other symptoms. Most patients depend on health care professionals to prevent and manage the varying physical and psychological symptoms that accompany advanced illness. To meet their obligations to their patients, practitioners must hold themselves and their colleagues responsible for using existing knowledge and available interventions to assess, prevent, and relieve physical and emotional distress. Unrelieved pain and other symptoms are the most evident problems that practitioners can readily avoid for the great majority of patients, but problems with communication, appropriate regard for patient and family wishes, and timely referral to palliative care specialists or teams are other areas in need of improvement. When good practice is hindered by organizational, financial, or legal impediments, health professionals have the responsibility as individuals and members of larger groups to advocate for system change.
RECOMMENDATION 3: Because many deficiencies in care reflect system problems, policymakers, consumer groups, and purchasers of health care should work with health care providers and researchers to
Although individuals must act to improve care at the end of life, systems of care must be changed to support such action. System change requires the involvement of public and private purchasers of care, regulators, and others whose policies and practices may create incentives for inappropriate care and barriers to excellent care.
Better information systems and tools for measuring outcomes and evaluating care are critical to the creation of effective and accountable systems of care and to the effective functioning of both internal and external systems of quality monitoring and improvement. Reliable and valid information about quality of care should be available to patients, purchasers, and ac-
crediting organizations, but organizations also need to audit their structures and processes for problem areas and commit themselves to improving care on an ongoing basis. Problem areas include insufficient numbers and types of properly trained personnel, nonexistent or inadequate protocols for symptom assessment and management, and poor procedures for evaluating the need for patient transfers or referrals and for carrying out such transfers without harm to patients. The committee supports the development of guidelines for clinical practice that assist clinicians in preventing and relieving symptoms and in managing the end stages of specific diseases.
Policymakers and purchasers need to consider both the long-recognized deficiencies of traditional fee-for-service arrangements and the less thoroughly understood strengths and limitations of alternatives, including various kinds of capitated and per case payment methods that apply in diverse ways to individual practitioners, interdisciplinary care teams, specific institutions, networks of providers, or integrated systems of care. Particularly in need of attention are the levels of payment for home and nursing home visits by physicians, the interpretation of evaluation and management codes, the lack of diagnosis- or condition-related adjustments in hospice payments for both home and inpatient care, and other financing incentives that may discourage hospices or health plans from enrolling sicker patients. In addition, reimbursement methods and related incentives should encourage continuity of care that supports patients all the way through death and reduces disconnected and episodic care. Health care professionals and organizations also need to formulate ethical guidelines to guard against possible conflicts of interest in capitated and other care systems.
The problems with laws relating to prescribing practices are twofold. One problem is outdated, scientifically flawed laws and regulations themselves. The other problem is clinician, regulator, and public misunderstanding of the appropriate use of opioids. State medical societies, licensing boards, legislative committees, and other groups should cooperate to review state laws, regulations, board practices, and physician attitudes and practices to identify problem areas and then devise revisions in those statutes and regulations that unduly burden clinical management of pain. Regulatory review and revision should be accompanied by educational efforts to increase scientifically and clinically based knowledge and correct misperceptions about the appropriate medical use of opioids and about the biological mechanisms of opioid dependence, addiction, and pain management. Legal change should help—but cannot be relied upon alone—to correct undertreatment.
RECOMMENDATION 4: Educators and other health professionals should initiate changes in undergraduate, graduate, and continuing education to ensure that practitioners have the relevant attitudes, knowledge, and
skills to care well for dying patients. Dying is too important a part of life to be left to one or two required (but poorly attended) lectures, to be considered only in ethical and not clinical terms, or to be set aside on the grounds that medical educators are already swamped with competing demands for time and resources. Every health professional who deals directly with patients and families needs a basic grounding in competent and compassionate care for seriously ill and dying patients. For clinicians and others to be held truly accountable for their care of the dying, educators must be held accountable for what they teach and what they implicitly and explicitly honor as exemplary practice. Textbooks and other materials likewise need revision to reflect the reality that people die and that dying patients are not people for whom "nothing can be done." As described in Chapter 8 , a number of promising curriculum models exist, and others are being developed and tested.
RECOMMENDATION 5: Palliative care should become, if not a medical specially, at least a defined area of expertise, education, and research. The objective is to create a cadre of palliative care experts whose numbers and talents are sufficient to (a) provide expert consultation and role models for colleagues, students, and other members of the health care team; (b) supply educational leadership and resources for scientifically based and practically useful undergraduate, graduate, and continuing medical education; and (c) organize and conduct biomedical, clinical, behavioral, and health services research. More generally, palliative care must be redefined to include prevention as well as relief of symptoms. Attention to symptoms should begin at earlier points during the trajectory of an illness because early treatment may well contribute to lessening pain at the end of life. The model for palliative care stresses interdisciplinary, comprehensive, and continuing care of patients and those close to them.
RECOMMENDATION 6: The nation's research establishment should define and implement priorities for strengthening the knowledge base for end-of-life care. The research establishment includes the National Institutes of Health, other federal agencies (e.g., the Agency for Health Care Policy and Research, the Health Care Financing Administration, the National Center for Health Statistics), academic centers, researchers in many disciplines, pharmaceutical companies, and foundations supporting health research. Their active support and involvement is necessary to advance basic and clinical research on the physiological mechanisms and treatment of symptoms common during the end of life, including neuropsychiatric problems. To extend understanding of quality-of-life issues in the treatment of advanced disease, those supporting clinical trials should encourage the collection of more information on the quality of life of those who die while
enrolled in such trials. A further step is to support more research on the physiological mechanisms and treatment of symptoms common during the end of life, including neuropsychiatric problems. Pain research appears to supply a good model for this enterprise to follow. In addition, pathways need to be developed to further the dissemination and replication of proven health care interventions and programs. Demonstration projects to test new methods of financing and organizing care should be a priority for the Health Care Financing Administration. To encourage change in the attitudes and understandings of the research establishment, the committee urges the National Institutes of Health and other public agencies to take the lead in organizing a series of workshops, consensus conferences, and agenda-setting projects that focus on what is and is not known about end stage disease and symptom prevention and treatment and that propose an agenda for further research. For the Agency for Health Care Policy and Research, the committee encourages support for the dissemination and replication of proven health care interventions and programs through clinical practice guidelines and other means.
RECOMMENDATION 7: A continuing public discussion is essential to develop a better understanding of the modern experience of dying, the options available to dying patients and families, and the obligations of communities to those approaching death. Individual conversations between practitioners and patients are important but cannot by themselves provide the supportive environment for the attitudes and actions that make it possible for most people to die free from avoidable distress and to find the peace or meaning that is significant to them. Although efforts to reduce the entertainment and news media's emphasis on violent or sensational death and unrealistic medical rescue have not been notably successful, a modicum of balance has recently been provided by thoughtful analyses; public forums; and other coverage of the clinical, emotional, and practical issues involved in end-of-life care. Regardless of how the current, highly publicized policy debate over physician-assisted suicide is resolved, the goal of improving care for those approaching death and overcoming the barriers to achieving that goal should not be allowed to fade from public consciousness. Much of the responsibility for keeping the public discussion going will rest not with the media but with public officials, professional organizations, religious leaders, and community groups.
Finally, the committee agreed that it was not prepared to take a position on the legality or morality of physician-assisted suicide. The issue should not, in any case, take precedence over those reforms to the health care system that would improve care for all dying patients. The goal of those who favor legalizing physician-assisted suicide is to promote patient autonomy, but true autonomy is not possible when significant numbers of
people have the limited choice between suicide or continued suffering. If the laws permitting physician-assisted suicide are implemented at the state level, careful monitoring of their consequences for the quality of care and the public's trust in health care will be very important.
Concluding Thoughts
Improving care at the end of life will require many changes in attitudes, policies, and actions. Such changes will involve a multitude of people and institutions that have a role in making and implementing decisions about patient care or in structuring the environments in which such decisions are reached and realized. Clearly, what patients and their families know, expect, and desire is important. Health care professionals play critical roles in diagnosis, communication, guidance and direction, treatment, negotiation, and advocacy for patients at many levels. Decisions by health plan managers, institutional administrators, and governmental officials shape and often impede the ability of patients, families, and clinicians to construct a care plan that serves the dying person well.
In general, changes in systems of care—not just individual beliefs and actions—are necessary if real gains are to be made in helping people live well despite fatal illness. Such widespread changes depend in part on a stronger social consensus on what constitutes appropriate and supportive care for those approaching death. Widely publicized—albeit not necessarily typical—instances of patient and family powerlessness to stop what they see as futile and painful treatments reflect a lack of such consensus. Paradoxically, this lack of consensus also is evident when patients or families demand treatments that practitioners see as useless, counterproductive, or even inhumane. It similarly reveals itself in a health care delivery and financing system that still rewards life-prolonging interventions (even when they will be ineffectual) and slights palliative and supportive services for those for whom life-extending treatment is neither helpful nor desired.
Freud may have been right that "our unconscious does not believe in its own death; it behaves as if immortal" (Freud, 1915, in Freud, 1959, p. 304). The committee was optimistic, nonetheless, that this society would cultivate the conscious intelligence and spirit to recognize the reality of death and the likelihood that it will bring distress. It likewise was optimistic that people would work together to create humane systems of care that assure the consistent use of existing knowledge to prevent and relieve suffering and that support efforts to provide people the right care at the right time in the right way. The analyses, conclusions, and recommendations presented here are offered with optimism that we can, individually and together, "approach" death constructively and create humane care systems that people can trust to serve them well as they die.
When the end of life makes its inevitable appearance, people should be able to expect reliable, humane, and effective caregiving. Yet too many dying people suffer unnecessarily. While an "overtreated" dying is feared, untreated pain or emotional abandonment are equally frightening.
Approaching Death reflects a wide-ranging effort to understand what we know about care at the end of life, what we have yet to learn, and what we know but do not adequately apply. It seeks to build understanding of what constitutes good care for the dying and offers recommendations to decisionmakers that address specific barriers to achieving good care.
This volume offers a profile of when, where, and how Americans die. It examines the dimensions of caring at the end of life:
- Determining diagnosis and prognosis and communicating these to patient and family.
- Establishing clinical and personal goals.
- Matching physical, psychological, spiritual, and practical care strategies to the patient's values and circumstances.
Approaching Death considers the dying experience in hospitals, nursing homes, and other settings and the role of interdisciplinary teams and managed care. It offers perspectives on quality measurement and improvement, the role of practice guidelines, cost concerns, and legal issues such as assisted suicide. The book proposes how health professionals can become better prepared to care well for those who are dying and to understand that these are not patients for whom "nothing can be done."
READ FREE ONLINE
Welcome to OpenBook!
You're looking at OpenBook, NAP.edu's online reading room since 1999. Based on feedback from you, our users, we've made some improvements that make it easier than ever to read thousands of publications on our website.
Do you want to take a quick tour of the OpenBook's features?
Show this book's table of contents , where you can jump to any chapter by name.
...or use these buttons to go back to the previous chapter or skip to the next one.
Jump up to the previous page or down to the next one. Also, you can type in a page number and press Enter to go directly to that page in the book.
Switch between the Original Pages , where you can read the report as it appeared in print, and Text Pages for the web version, where you can highlight and search the text.
To search the entire text of this book, type in your search term here and press Enter .
Share a link to this book page on your preferred social network or via email.
View our suggested citation for this chapter.
Ready to take your reading offline? Click here to buy this book in print or download it as a free PDF, if available.
Get Email Updates
Do you enjoy reading reports from the Academies online for free ? Sign up for email notifications and we'll let you know about new publications in your areas of interest when they're released.
- - Google Chrome
Intended for healthcare professionals
- Access provided by Google Indexer
- My email alerts
- BMA member login
- Username * Password * Forgot your log in details? Need to activate BMA Member Log In Log in via OpenAthens Log in via your institution
Search form
- Advanced search
- Search responses
- Search blogs
- News & Views
- Euthanasia and...
Euthanasia and assisted dying: the illusion of autonomy—an essay by Ole Hartling
Read our coverage of the assisted dying debate.
- Related content
- Peer review
- Ole Hartling , former chairman
- Danish Council of Ethics, Denmark
- hartling{at}dadlnet.dk
As a medical doctor I have, with some worry, followed the assisted dying debate that regularly hits headlines in many parts of the world. The main arguments for legalisation are respecting self-determination and alleviating suffering. Since those arguments appear self-evident, my book Euthanasia and the Ethics of a Doctor’s Decisions—An Argument Against Assisted Dying 1 aimed to contribute to the international debate on this matter.
I found it worthwhile to look into the arguments for legalisation more closely, with the hope of sowing a little doubt in the minds of those who exhibit absolute certainty in the matter. This essay focuses on one point: the concept of “autonomy.”
(While there are several definitions of voluntary, involuntary, and non-voluntary euthanasia as well as assisted dying, assisted suicide, and physician assisted suicide, for the purposes of brevity in this essay, I use “assisted dying” throughout.)
Currently, in richer countries, arguments for legalising assisted dying frequently refer to the right to self-determination—or autonomy and free will. Our ability to self-determine seems to be unlimited and our right to it inviolable. The public’s response to opinion poll questions on voluntary euthanasia show that people can scarcely imagine not being able to make up their own minds, nor can they imagine not having the choice. Moreover, a healthy person answering a poll may have difficulty imagining being in a predicament where they simply would not wish to be given the choice.
I question whether self-determination is genuinely possible when choosing your own death. In my book, I explain that the choice will always be made in the context of a non-autonomous assessment of your quality of life—that is, an assessment outside your control. 1
All essential decisions that we make are made in relation to other people. Our decisions are affected by other people, and they affect other people. Although healthy people find it difficult to imagine themselves in situations where they do not decide freely, it is also true that all of us are vulnerable and dependent on others.
Yet autonomy in relation to assisted dying is often viewed in the same way as our fundamental right to choose our own course in life. If we are able to control our lives, then surely we can also control our death. Autonomy with respect to your own death, however, is already halved: you can choose to die if you don’t want to live, but you cannot choose to live if you are about to die.
Decisions about your own death are not made in normal day-to-day contexts. The wish to die arises against a backdrop: of desperation, a feeling of hopelessness, possibly a feeling of being superfluous. Otherwise, the wish would not be there. Thus, it is under these circumstances that the right to self-determination is exercised and the decision is made. Such a situation is a fragile basis for autonomy and an even more fragile basis for decision making. The choice regarding your own death is therefore completely different from most other choices usually associated with the concept of autonomy.
Here are just some of the critical matters that would arise if assisted dying were legalised.
A duty to die
The possibility of choosing to die would inhabit everyone’s consciousness—the patient, the doctor, the relatives, and the care staff—even if not formulated as an out-and-out offer. But if a law on assisted dying gives the patient a right to die, that right may turn into a duty to die. How autonomously can the weakest people act when the world around them deems their ill, dependent, and pained quality of life as beyond recovery?
Patients can find themselves directly or indirectly under duress to choose that option if they consider themselves sufficiently pained and their quality of life sufficiently low. Patients must be at liberty to choose assisted dying freely, of course—that is how it is presented—but the point is that the patient cannot get out of having to choose. It has been called the “prison of freedom.”
Internalised external pressure
Pressure on the patient does not have to be direct or articulated. As pointed out by the US professor of biomedical ethics Daniel Sulmasy it may exist as an “internalised external pressure.” 2 Likewise, the French bioethicist Emmanuel Hirsch states that individual autonomy can be an illusion. The theologian Nigel Biggar quotes Hirsch saying that a patient “may truly want to die, but this desire is not the fruit of his freedom alone, it may be—and most often is—the translation of the attitude of those around him, if not of society as a whole which no longer believes in the value of his life and signals this to him in all sorts of ways. Here we have a supreme paradox: someone is cast out of the land of the living and then thinks that he, personally, wants to die.” 3
The end of autonomy
An inherent problem of autonomy in connection with assisted dying is that a person who uses his or her presumed right to self-determination to choose death definitively precludes himself or herself from deciding or choosing anything. Where death is concerned, your right to self- determination can be exerted only by disposing of it for good. By your autonomy, in other words, you opt to no longer have autonomy. And those around must respect the right to self-determination. The respect refers to a person who is respected, but this is precisely the person who disappears.
Danish philosopher Johannes Sløk, who supported legalisation, said, “The actual concept of death has no content, for death is the same as nothing, and one cannot choose between life and nothing. Rather, therefore, one must speak of opting out; one opts out of life, without thereby choosing anything else. Death is not ‘something other’ than life; it is the cessation or annihilation of life.”
Autonomy is a consistent principle running through the care and management of patients and is enshrined in law. However, a patient’s autonomy means that he or she has the right to decline any treatment. It does not entail a right to have any treatment the patient might wish for. Patients do not have the right to demand treatment that signifies another’s duty to fulfil that right. If that were so, autonomy would be the same as “autocracy”—rule of the self over others. Even though patients have the right to reject any intervention, they do not have the right to demand any intervention. Rejecting any claim that the person might make is not a violation of a patient’s self- determination—for example, there may be sound medical reasons for not complying with a demand. The doctor also has autonomy, allowing him or her to say no. Refusing to kill a person or assist in killing cannot be a violation of that person’s autonomy.
The killing ban
Assisted dying requires the doctor’s moral and physical help. It is a binding agreement between two people: the one who is to be killed and the one who is to kill or assist in killing. But our society does not condone killing as a relationship between two legally competent, consenting people. Exemptions from the killing ban involve war or self-defence and are not justified on the grounds that the killing is done for the “benefit” of someone else.
Valuation of a life
If the action is to be decriminalised, as some people wish, it means the doctor will have to enter into deliberations and arguments for and against a request for assisted dying each time. That is, whether he or she is willing to grant it. The alternative would be to refer the patient to another doctor who might be willing to help—that doctor would still have to assess whether the patient’s life was worth preserving.
Thus, autonomy is not the only factor or even always the key factor when deciding whether assisted dying can be granted. It is not only the patient’s own evaluation that is crucial. The value of the patient’s life must also be assessed as sufficiently low. This demonstrates the limitation of the patient’s self-determination.
Relieving suffering
If a competent and legally capable person must have the option of voluntarily choosing assisted dying in the event of unbearable suffering, why does suffering have to be a requirement? The answer is straightforward: our concepts of assisted dying imply that compassion must form a crucial aspect of the decision—mercy killing and compassionate killing are synonyms. But this leads instantly to the question of why we should not also perform assisted dying on people who are not in a position to ask for it themselves but are also suffering.
Some people find the reasoning unproblematic. It stands to reason that relieving suffering is a duty after all. But in this context it is not unproblematic, because it effectively shifts the focus from the autonomy claimed. According to prevailing ideas about autonomy, patients initially evaluate their quality of life themselves, but ultimately it is those around them who end up gauging that quality and the value of their life. That is to say, the justification for assisted dying is borne on the premise that certain lives are not worth living rather than the presence of a request. The whole point is that in the process, respect for the right to self-determination becomes relative.
Autonomy is largely an illusion in the case of assisted dying. 1 A patient overwhelmed by suffering may be more in need of compassion, care, and love than of a kind offer to help end his or her life. It is not a question of whether people have a right to say that they are unworthy. It is a question of whether they have a right to be believed when saying it.
Ole Hartling is a physician of over 30 years standing, doctor of medical sciences at the University of Copenhagen, professor of health promotion at the University of Roskilde, and an author and co-author of several books and scientific articles published mainly in Scandinavia. Between 2000 and 2007 he was a member of the Danish Council of Ethics and its chair for five years. During this time, the council extensively debated the ethics of euthanasia and assisted dying.
Competing interests: I have read and understood BMJ policy on declaration of interests and have no relevant interests to declare.
- Gastmans C ,
- MacKellar C

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Ann Med Surg (Lond)
- v.75; 2022 Mar
Euthanasia and assisted suicide: An in-depth review of relevant historical aspects
Yelson alejandro picón-jaimes.
a Medical and Surgical Research Center, Future Surgeons Chapter, Colombian Surgery Association, Bogotá, Colombia
Ivan David Lozada-Martinez
b Grupo Prometheus y Biomedicina Aplicada a las Ciencias Clínicas, School of Medicine, Universidad de Cartagena, Cartagena, Colombia
Javier Esteban Orozco-Chinome
c Department of Medicine, RedSalud, Santiago de Chile, Chile
Lina María Montaña-Gómez
d Department of Medicine, Keralty Salud, Bogotá, Colombia
María Paz Bolaño-Romero
Luis rafael moscote-salazar.
e Colombian Clinical Research Group in Neurocritical Care, Latin American Council of Neurocritical Care, Bogotá, Colombia
Tariq Janjua
f Department of Intensive Care, Regions Hospital, Minnesota, USA
Sabrina Rahman
g Independent University, Dhaka, Bangladesh
End-of-life care is an increasingly relevant topic due to advances in biomedical research and the establishment of new disciplines in evidence-based medicine and bioethics. Euthanasia and assisted suicide are two terms widely discussed in medicine, which cause displeasure on many occasions and cause relief on others. The evolution of these terms and the events associated with their study have allowed the evaluation of cases that have established useful definitions for the legal regulation of palliative care and public policies in the different health systems. However, there are still many aspects to be elucidated and defined. Based on the above, this review aimed to compile relevant historical aspects on the evolution of euthanasia and assisted suicide, which will allow understanding the use and research of these terms.
- • The history of euthanasia and assisted suicide has been traumatic.
- • The church and research have been decisive in the definition of euthanasia.
- • The legal framework on the use of euthanasia and assisted suicide has been strengthened.
1. Introduction
Euthanasia and assisted suicide are two topics discussed throughout history, mainly because they fall within the scope of life as a human right, which has been universally defended for many years [ 1 ]. However, the mean of the word euthanasia as good death generates conflicts at social, moral, and ethical levels. Mainly because death is a loss, it is difficult to understand it as something positive and; additionally, several historical events such as the Nazi experiments related the term euthanasia more to murder than to a kind and compassionate act [ 1 ]. More current texts mention that euthanasia is the process in which, through the use or abstention of clinical measures, the death of a patient in an incurable or terminal condition can be hastened to avoid excessive suffering [ 2 ].
The difference between euthanasia and assisted suicide is that in the latter, the patient takes the final action; however, both practices can be combined in the term assisted death [ 2 ]. At present, several countries authorize assisted death, including Holland, Luxembourg, and Canada [ 3 ]. Belgium and Colombia have regulations that decriminalize only euthanasia; other places where assisted suicide is legal are Switzerland and five states of the United America states, specifically Oregon, Vermont, Washington, California, and Montana [ 2 , 3 ]. Spain recently joined the list of countries that have legislated on euthanasia through the organic law March 2021 of March 24 that regulates euthanasia in that state in both public and private institutions [ 4 ]. The fact that more and more countries were joining the legislation on euthanasia and assisted suicide has brought to light the opinion of thinkers, politicians, philosophers, and physicians. Several nations have initiated discussions on the matter in their governmental systems. Latin America is trying to advance powerfully in this medical-philosophical field. Currently, in Chile, the “Muerte digna y cuidados paliativos” law, which seeks to regulate the issue of euthanasia and assisted suicide in the country, is being debated in Congress [ 5 ].
It is essential to know the point of view of physicians on euthanasia and assisted suicide, especially taking into account that these professionals who provide care and accompany patients during this moment, which, if approved, would involve the medical community in both public and private health systems. Although it seems easy to think that physicians have a position in favor of the act of euthanasia because they are in direct and continuous contact with end-of-life situations, such as palliative care, terminally ill, and critically ill patients. It is important to remember that the Hippocratic medical oaths taken at the time of graduation of professionals are mostly categorical in mentioning the rejection of euthanasia and assisted suicide [ 6 ]. Furthermore, it is also important to note that many of the oldest universities in the Western world originated through the Catholic Church; and just this creed condemns the practice of euthanasia and continues to condemn it to this day. This situation generates that many medical students in these schools have behaviors based on humanist principles under the protection of faith and religion and therefore reject the possibility of euthanasia [ 7 , 8 ].
The relevance of the topic and the extensive discussion that it has had in recent months due to the COVID-19 pandemic added to the particular interest of bioethics in this topic and the need to know the point of view of doctors and other health professionals on euthanasia and assisted suicide.
2. Origin and meaning of the term euthanasia
The word euthanasia derives from the Greek word “eu” which means good, and the word “thanatos” which means death; therefore, the etymological meaning of this word is “good death”. Over time the evolution of the meaning has varied; even as we will see below was considered a form of eradication of people categorized under the designation of leading a less dignified life. Assisted suicide is a condition in which the patient is the one who carries out the action that ends his life through the ingestion of a lethal drug but has been dispensed in the context of health care and therefore called assisted. This care is provided by a physician trained in the area. However, it requires the prior coordination of a multidisciplinary team and even the assessment by an ethics committee to determine that the patient is exercising full autonomy, free from coercion by the situation he/she is living and free from the fatalistic desires of a psychiatric illness [ 9 ]. In a more literary sense, the word euthanasia meaning of “giving death to a person who freely requests it in order to free himself from suffering that is irreversible and that the person himself considers intolerable” [ 9 ].
Some authors go deeper into the definition and consider that for the meaning of euthanasia, are necessary to consider elements that are essential in the word itself; such as the fact that it is an act that seeks to provoke death and that carried out to eliminate the suffering in the person who is dying. Other elements with a secondary character in the definition are the patient's consent (which must be granted respecting autonomy and freedom in the positive and negative sense; that means the fact must be not be coerced in any way). Another element is the terminal nature of the disease, with an irreversible outcome that generates precariousness and a loss of dignity. The third secondary element is the absence of pain of the death through the use of drugs such as high-potency analgesics, including opioids, high-potency muscle relaxants, and even anesthetic drugs. Finally, the last element is the health context in which the action is performed (essential in some legislations to be considered euthanasia) [ 10 ]. According to the World Health Organization, the union of these two components is the current definition of euthanasia, which describes as “the action performed by a person to cause the painless death of another subject, or not preventing death in case of terminal illness or irreversible coma. Furthermore, with the explicit condition that the patient must be suffering physical, emotional, or spiritual and that affliction is uncontrollable with conventional measures such as medical treatments, analgesics, among others; then the objective of euthanasia is to alleviate this suffering” [ 11 ]. Unfortunately, the term euthanasia has been misused over the years, and other practices have been named with this word. An example of this situation occurred during the Nazi tyranny when the word euthanasia concerned the murder of people with disabilities, mental disorders, low social status, or gay people. At that time, euthanasia was even a simultaneous practice to the Jewish genocide [ 11 ].
Not only has the term been misused; also exists an enormous variability of terms to refer to euthanasia. For example, the laws created to regulate euthanasia have different names around the world; in the Netherlands (Holland), the law that regulates this practice is known as the law of termination of life; in Belgium, it is called euthanasia law, in France, it is called euthanasia law too. In Oregon (USA), it is called the death with dignity act; in California, it is the end of life option act. In Canada is called the medical assistance in dying act. Victoria (Australia) is the voluntary assisted dying bill, but all these denominations refer to the already well-known term euthanasia [ 11 ].
3. Evolution of euthanasia and assisted suicide: digging into historical events
To understand the evolution and relevance of these concepts should analyze the history of euthanasia and assisted suicide; from the emergence of the term, going through its first manifestations in antiquity; mentioning the conceptions of great thinkers such as Plato and Hippocrates; going through the role of the Catholic Church; mainly in the Middle Age, where following the thought of St. Thomas Aquinas, self-induced death or death contemplated by own will, was condemned. Later, with the renaissance age and the resurgence of science, technology, and the arts, the term euthanasia made a transition to a form similar to what we know today from thinkers such as Thomas More and Francis Bacon. Finally, the first signs of eugenics were known in London, Sweden, Germany, and the United States in the twentieth century. There was a relationship with the term euthanasia that was later used interchangeably, especially in the Nazi regime, to denote a form of systemic murder that sought to eradicate those who were not worthy of living a life.
Since the sixties, with emblematic cases, the path towards the decriminalization of euthanasia began in some countries, especially concerning the cessation of extreme support measures in cases of irreversible illness or a terminal condition. The practice has progressed to the appearance of laws on euthanasia in several countries.
4. Euthanasia and assisted suicide in ancient times
In book III of Plato's “The Republic”, the author stated that those who live their lives amidst illnesses and medicines or who were not physically healthy should be left to die; implying that it was thought that people in these conditions suffered so much that their quality of life diminished, which seemed understandable to these thinkers. However, other authors such as Hippocrates and his famous Hippocratic oath sought the protection of the patient's life through medicine, especially in vulnerable health conditions prone to fatal outcomes. This Hippocratic oath is the same oath that permeates our times and constitutes an argument among those who mark their position against euthanasia and assisted suicide [ 12 , 13 ].
Other texts that collect thoughts of Socrates and his disciple Plato point out that it was possible and well understood to think of ceasing to live in the face of a severe illness; to consider death to avoid a long and torturous agony. This fact is compatible with the conception of current euthanasia since this is the end of this health care procedure [ 13 ].
In The Republic, the text by Plato, the physician Heroditus is also condemned for inventing a way to prolong death and over manage the symptoms of serious illnesses, which is currently known as distanasia or excessive treatment prolongs life. This kind of excessive treatment prolongs the sick person's suffering, even leading him to maintain biological signs present but in a state of alienation and absolute dependence on medical equipment such as ventilators and artificial feeding [ 13 ]. However, the strongest indication that Euthanasic suicide was encouraged in Greece lies in other thinkers such as the Pythagoreans, Aristotelians, and Epicureans who strongly condemned this practice, which suggests that it was carried out repeatedly as a method and was therefore condemned by these thinkers [ 12 , 13 ]. According to stoicism, the pain that exceeded the limits of what was humanly bearable was one of the causes for which the wise man separates himself from life. Referring to one of the nuances that euthanasia touches today, that is, at a point of elevated suffering, the dignity and essence of the person are lost, persisting only the biological part but in the absence of the person's well-being as a being. In this sense, Lucius Seneca said that a person should not love life too much or hate it; but that person should have a middle ground and end their life when they ceased to perceive life as a good, worthy, and longed-for event [ 1 , 12 ].
During the Roman Empire and in the territories under its rule, it was believed that the terminally ill who commit suicide had sufficient reasons to do so; so since suicide caused by impatience and lack of resolution to pain or illness was accepted, when there was no access to medicines. In addition, there was little development in medicine during that time, and many of the sick died without treatment [ 12 ]. This situation changed later with the emergence of the Catholic church; in this age, who attempted against own life, was deprived of burial in the ground. Saint Augustine said that the suicide was an abominable and detestable act; from 693 AD, anyone who attempted against his physical integrity was excommunicated. Rejecting to the individuals and their lineage, depriving them of the possibility of attending the funeral and even expelled from cities and stripped of the properties they owned [ 12 , 13 ].
4.1. Euthanasia and assisted suicide in the Middle Age
During the Middle Age, Catholicism governed the sciences, arts, and medicine; the sciences fell asleep. Due to this solid religious tendency and the persistence of Augustinian thought, suicide was not well seen. It was not allowed to administer a lethal substance to a person to end the suffering of a severe or terminal illness [ 9 , 12 ]. People who took their own lives at this time could not be buried “Christianly”; therefore, they did not have access to a funeral, nor to the accompaniment of their family in a religious rite. Physical suffering and pain were then seen as a path to glorification. Suffering was extolled as the form that god purified the sin, similar to the suffering that Jesus endured during his Calvary days. However, a contrary situation was experienced in battles; a sort of short dagger-like weapon was often used to finish off badly wounded enemies and thus reduce their suffering, thus depriving them of the possibility of healing and was called “mercy killing” [ 12 ].
5. Euthanasia in renaissance
With the awakening of science and philosophy, ancient philosophers' thoughts took up again, giving priority to man, the world, and nature, thus promoting medical and scientific development. In their discourse, Thomas More and Francis Bacon refer to euthanasia; however, they give a eugenic sense to the concept of euthanasia, similar to that professed in the book of Plato's Republic. It is precise with these phylosophers that the term euthanasia got its current focus, referring to the acceleration of the death of a seriously ill person who has no possibility of recovery [ 12 ]. In other words, it was during this period that euthanasia acquired its current meaning, and death began to be considered the last act of life. Therefore, it was necessary to help the dying person with all available resources to achieve a dignified death without suffering, closing the cycle of life that ends with death [ 13 , 14 ].
In his work titled “Utopia”, Thomas More affirmed that in the ideal nation should be given the necessary and supportive care to the dying. Furthermore, in case of extraordinary suffering, it can be recommended to end the suffering, but only if the patient agrees, through deprivation of food or with the administration of a lethal drug; this procedure must be known to the affected person and with the due permission of authorities and priests [ 12 , 13 ]. Later, in the 17th century, the theologian Johann Andreae, in his utopia “Christianopolis”, contradicts the arguments of Bacon and Moro, defending the right of the seriously ill and incurably ill to continue living, even if they are disturbed and alienated, advocating for the care based on support and indulgence [ 15 , 16 ]. Similarly, many physicians rejected the concepts of Plato, Moro, and Bacon. Instead, they focused on opposing euthanasia, most notably in the nineteenth century. For example, the physician Christoph Hufeland mentioned that the doctor's job was only to preserve life, whether it was a fate or a misfortune, or whether it was worth living [ 16 ].
5.1. Euthanasia in the 20th century
Before considering the relevant aspects of euthanasia in the 20th century, it is vital to highlight the manuscript by Licata et al. [ 17 ], which narrates two episodes of euthanasia in the 19th century. The first one happened in Sicily (Italy) in 1860, during the battle of Calatafimi, where two soldiers were in constant suffering, one because he had a serious leg fracture with gangrene, and the other with a gunshot wound. The two soldiers begged to be allowed to die, and how they were in a precarious place without medical supplies, they gave them an opium pill, which calmed them until they died [ 17 ]. The second episode reported by Licata et al. [ 17 ] was witnessed by a Swedish doctor named Alex Munthe; who evidenced the pain of many patients in a Parisian hospital. So he decided to start administering morphine to help people who had been seriously injured by wolves and had a poor prognosis; therefore, the purpose of opioid use was analgesia while death was occurring.
It is also important to highlight the manuscript entitled “Euthanasia” by S. Williams published in 1873 in “Popular Science Monthly”, a journal that published texts by Darwin, Edison, Pasteur, and Beecher. This text included the report for the active euthanasia of seriously ill patients without a cure, in which the physicians were advised to administer chloroform to these patients or another anesthetic agent to reduce the level of consciousness of the subject and speed up their death in a painless manner [ 16 ].
Understanding that euthanasia was already reported in the nineteenth century, years after, specifically in 1900, the influence of eugenics, utilitarianism, social Darwinism, and the new currents of thought in England and Germany; it began in various parts around the world, projects that considered the active termination of life, thus giving rise to euthanasia societies in which there were discussions between philosophers, theologians, lawyers, and medical doctors. Those societies discussed diverse cases, such as the tuberculous patient Roland Gerkan, who was considered unfit and therefore a candidate to be released from the world [ 16 ]. The scarcity of resources, famine, and wars were reasons to promote euthanasia as a form of elimination of subjects considered weak or unfit, as argued in texts such as Ernst Haeckel's. However, opponents to the practice, such as Binding and Hoche, defended the principle of free will in 1920 [ 16 ].
5.2. Euthanasia in the time of the Nazis
As mentioned above, the term euthanasia was misused during this period; approximately 275,000 subjects (as reported at the Nuremberg International Military Tribunal 1945–1946), who had some degree of physical or mental disability, were killed during Adolf Hitler's Euthanasia program [ 13 ]. However, the Nazis were not the first to practice a form of eugenics under the name of euthanasia, since the early 1900s in London had already begun the sterilization of the rejected, such as the blind, deaf, mentally retarded, people with epilepsy, criminals, and rapists. This practice spread to different countries like Sweden and the United States [ 13 , 16 ].
For the Nazis, euthanasia represented the systematic murder of those whose lives were unworthy of living [ 13 ]. The name given to this doctrine was “Aktion T4”. At first and by law, from 1939, the hospitals were obliged to account for all disabled newborns, which led to the execution of more than 5000 newborns utilizing food deprivation or lethal injection [ 12 , 18 ].
A year before that law, in 1938, one of the first known cases of euthanasia in children arose in Germany. That history called the story of child K, in which it was the father of the minor who asked Hitler in writing for euthanasia for his son because the child had a severe mental disability and critical morphic disorders. Hitler gave his consent to carry out the procedure on child K, and thus the program began to spread throughout the Aleman territory. Since then, physicians and nurses had been in charge of reporting the newborns with alterations, arising the “Kinderfachabteilugen” for the internment of children who would be sentenced to death after a committee's decision [ 12 , 18 , 19 ]. A list of diseases and conditions that were considered undesirable to be transmitted to Hitler's superior Aryan race was determined; thus, any child with idiocy, mongolism, blindness, deafness, hydrocephalus, paralysis, and spinal, head, and hip malformations were eligible for euthanasia [ 19 ].
Subsequently, the program was extended to adults with chronic illness, so those people were selected and transported by T4 personnel to psychiatric sanatoriums strategically located far away. There, the ill patients received the injection of barbiturate overdoses, and carbon monoxide poisoning was tested as a method of elimination, surging the widely known gas chamber of the concentration camp extermination; this situation occurred before 1940 [ 12 , 19 ]. Again, physicians and nurses were the ones who designated to the patients to receive those procedures; in this case, these health professionals supported Nazi exterminations. They took the patients to the sanatoriums, where psychiatrists evaluated them and designated with red color if they should die and with a blue color if they were allowed to live (this form of selection was similar in children) [ 12 , 13 , 19 ]. In this case, the pathologies considered as criteria for death were those generating disability such as schizophrenia, paralysis, syphilis with sequelae, epilepsy, chorea, patients with chronic diseases with many recent treatments, subjects of non-German origin and individuals of mixed blood [ 19 ]. Once in the sanatoriums, they were informed that they would undergo a physical evaluation and take a shower to disinfect themselves; instead, they were killed in gas chambers [ 12 , 13 ]. Despite the church's action in 1941 against Nazis and after achieving suspension of the Aktion T4 project; the Nazi supporters kept the practices secretly, resuming them in 1942, with the difference that the victims were killed by lethal injection, by an overdose of drugs, or left to starve to death, instead of the use of gas chambers. This new modified form of euthanasia, which did not include gas chambers, became known as “savage euthanasia” [ 12 , 13 , 19 ].
5.3. Euthanasia since the 1960s
In September 1945, trials began for crimes perpetrated by Nazi supporters; the victorious Allied forces conducted these trials at the end of the war. During these tribunals, cases of human experimentation were identified and the public exposure of the Nazi euthanasia program. After the Nuremberg trials and the abolition of Nazi experiments, a series of seven documents emerged, among which the Nuremberg code containing the ten basic principles for human research stood out [ 20 , 21 ].
After these judgments, biotechnology was accelerated, with the apparition of new techniques to intervene in the health-disease process. Additionally, the increase in life expectancy and the appearance of diseases that chronically compromise the state of health of people generated a change in the conception of the critically ill patient and the terminal state of life [ 20 , 21 ]. Cases such as Karen Ann Quinlan brought to the forefront the issue of euthanasia and precisely the control of extreme treatment measures. Karen, a young American woman, was left in a vegetative state due to severe neurological damage following alcohol and barbiturate intoxication. After six months in that state and under the guardianship of a Catholic priest, Karen's parents requested the removal of the artificial respirator, arguing that in her state of consciousness prior to the incident, she had stated that she disagreed with artificially maintaining life in comatose patients. The hospital refused to remove the ventilator, arguing the legal issues for the date, and the parents went to court, which in the first instance granted the hospital the right. Nevertheless, the New Jersey Supreme Court granted Karen Ann's right to die in peace and dignity. Despite the withdrawal of the artificial respirator, he continued to live until 1985, when he finally died [ [21] , [22] , [23] ].
Another important case was Paul Brophy, which also occurred in the United States. Paul was a firefighter in Massachusetts and went into a deep coma due to the rupture of a basilar artery aneurysm; initially, his family advocated for support measures but later requested the hospital to disconnect these means to allow death, as Paul had indicated when he was still conscious. The hospital refused to carry out this procedure, so the family went to court, where the removal of the support measures (gastrostomy) was initially denied. Hence, the family went to the state supreme court, achieving the transfer of Paul to another medical center where the gastrostomy was removed, leading to his death within a few days [ 23 ].
The case of Arthur Koestler, an influential English writer and activist diagnosed with Parkinson's disease and later with leukemia, who served as vice-president of the voluntary euthanasia society (Exit) and wrote a manual book with practical advice for euthanasia called “Guide to Self-Liberation”. He stood out because he applied one of his advice and ingested an overdose of barbiturates, causing his self-death. According to his writings, Koestler was not afraid of death but of the painful process of dying [ 23 ]. In this sense, it was a relevant case because it involved someone who held an important position in an association that advocated euthanasia, in addition to being the author of several works, which made him a recognized public figure [ 23 ].
Baby Doe was a case that also occurred in the United States; it was a small child with Down syndrome who had a tracheoesophageal fistula and esophageal atresia; in this case, surgery was necessary. On the advice of the obstetrician, the parents did not allow surgery, so the hospital managers took the case before a judge who ruled that parents could decide to perform or not the surgery. The case was appealed before a county judge who upheld the parents' power to make the decision, in the course of which the case became public and many families offered to take care of the child; however, before the case reached the supreme court, the child died at six days of age [ 23 ].
In the case of Ingrid Frank, a German woman who was in a quadriplegic state by a traffic accident, who initially sought rehabilitation but later insisted on being allowed to die; it was provided with a drink containing a cyanide solution that she drank. At the same time, she was filmed, which shows a kind of assisted suicide. For that reason, this is another case that deals with this issue and is important to know as background in the development of euthanasia and assisted suicide [ 22 , 23 ].
6. Current and future perspectives
The definition of brain death, the rational use of the concept of euthanasia and assisted suicide, and scientific literacy are the objectives of global bioethics to regulate euthanasia and assisted suicide, which can be accessible in all health systems [ [24] , [25] , [26] , [27] , [28] , [29] , [30] ]. End-of-life care will continue to be a subject of debate due to the struggle between biomedical principles, the different existing legal frameworks, and the general population's beliefs. Medical education and preparation in the perception of death, especially of a dignified death, seems to be the pillar of the understanding of the need to develop medical-legal tools that guarantee the integrity of humans until the end of their existence [ 31 , 32 ]. This is the reason why the new generations of physicians must be trained in bioethics to face these ethical conflicts during the development of their professional careers.
In addition, although the conception of bioethics belongs to the Western world, it is crucial to take into account the point of view of other cultures and creeds, for example, a study carried out in Turkey, where nursing students were questioned, found that many of them understood the reasons for performing euthanasia; however, they know that Islam prohibits it, as well as its legislation, and therefore they would not participate in this type of procedure [ 33 ]. Furthermore, Christianism and Islam prohibit euthanasia, but Judaism also prohibits it; in general, the so-called Abrahamic religions are contrary to any form of assisted death, whether it is active euthanasia, passive, or assisted suicide [ 34 ].
7. Conclusiones
The history and evolution of euthanasia and assisted suicide have been traumatic throughout human history. The church, politics, and biomedical research have been decisive in defining these concepts. Over the years, the legal framework and bioethical concepts on euthanasia have been strengthened. However, there is still much work to educate the general population and health professionals about end-of-life care and dignified death.
It is also important to remember that life is a concept that goes beyond biology. Currently, bioethics seeks to prioritize the concept of dignity, which must be linked to the very definition of life. Although the phrase is often heard that it is not necessary to move to be alive, what is important is that person feels worthy even if they have limited movement. The person's treatment must be individualized in bioethics since each individual is a unique unit. Therefore, medical paternalism must be abandoned. Instead, the subject must be more involved to understand their context and perception of life and dignity.
Ethical approval
It is not necessary.
Sources of funding for your research
Author contribution.
All authors equally contributed to the analysis and writing of the manuscript.
Provenance and peer review
Not commissioned, externally peer reviewed.
Research registration Unique Identifying number (UIN)
- 1. Name of the registry: Not applicable.
- 2. Unique Identifying number or registration ID: Not applicable.
- 3. Hyperlink to your specific registration (must be publicly accessible and will be checked): Not applicable.
Sabrina Rahman. Independent University, Dhaka, Bangladesh. [email protected] .
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.

The Ethics of Euthanasia
Malleeka Suy | SQ Blogger | SQ Online (2021-2022)
Picture t his: It is the year 3020, and the Martian soil you have been drilling into has finally worked out. Colonizing Mars is taking shape, and soon your family can permanently live on this rusty, rocky planet. However, the effects of progress don’t go unnoticed; every time you move, your skin screams in pain. Everything you once loved doing has lost its appeal. Would you take death in your own hands or live until a painful end?
This moral dilemma seems straight out of a science-fiction novel for most, but euthanasia is a legitimate deliberation for patients with terminal and mental illnesses who deem their lives too painful to live on. It is a practice that is still heavily debated in modern bioethics. Among many definitions, the American Medical Association defines euthanasia as the administration of a lethal agent by a medical professional to a patient to relieve their intolerable or incurable suffering.
Although euthanasia is not a new scientific process, as it has been practiced since the time of the ancient Greeks more than three thousand years ago, it wasn’t generally accepted by Western medicine until recently. The Netherlands was the first country to allow legal euthanasia and assisted suicide in 2002, totaling 1.7-2.8% of total deaths. Euthanasia is generally illegal in the United States, but in a nationwide 2017 American poll , 73% of the public were in favor of euthanasia, and 57% said euthanasia is morally acceptable. These numbers are nearly double the initial poll in 1947. If I had to guess why, it may be partly because of progressive exposure to mental health and its effects. This may have allowed people to understand and empathize with the circumstances and support what euthanasia stands for: a release from an unbearable life.
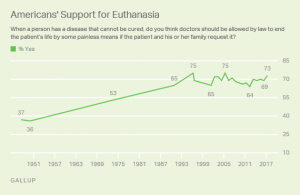
Euthanasia is especially controversial among general society and the bioethical community. One main argument for the support of euthanasia is grounded in personal autonomy–our ability to act independently– since living life is about minimizing physical pain and maximizing dignity and control . This idea is rooted in ancient times when physicians considered dying with peace and dignity a human right. An article from Stanford’s Encyclopedia of Philosophy regards autonomy as self-determination, so choices about how and when people die is them taking responsibility for their lives. Terminally ill patients in Oregon mentioned how they chose euthanasia because their condition stripped them of their independence and ability to engage in activities that gave their life meaning. After all, what is the meaning of life if we cannot live it?
Another article by the Linacre Quarterly highlights how the ethics of compassion justify the use of euthanasia. From a humanitarian standpoint, we can show compassion by suffering and sympathizing with patients and respecting their wishes of euthanasia as their “remedy.” Kenneth L. Vaux, a consultant in medical ethics, notes in his article that physicians would give a lethal dose to their loved ones out of love if they were dying and suffering, so he finds it “strange and hypocritical” that doctors cannot legally do so for their patients. He claims that “we have lost empathy, sympathy, and the covenant of care with those who have entrusted their lives to us because they believe we embody those very qualities.” Vaux also asks: “Having barred the door to Death, are we not then obliged at some point to open it?” He suggests that since doctors bring life into the world every day, consensually ending a patient’s life for their benefit should be no different.
Despite popular social support, there are many arguments against euthanasia as well–the most popular being religion. Several faiths, such as Christianity, see euthanasia as a form of murder and find it to be morally unacceptable because it may weaken society’s respect for the sanctity of life. Religious groups actively argue against euthanasia, and for this reason, euthanasia became a debate of preservation and purity of life.
Even though medicine is rooted in science, some physicians also use religion as justification against practicing euthanasia. Contrary to public British opinion, studies show that most UK doctors do not support legislation permitting euthanasia due to their religiosity or faith, and less than a quarter of doctors would be willing to practice euthanasia if it became legal.
Physicians also have a professional obligation to fulfill that becomes morally blurred with euthanasia. For more than 2,500 years, doctors have taken the Hippocratic Oath to do no harm and treat those under their care. Does bringing death by euthanasia violate the Hippocratic Oath, or is it in line with a doctor’s mission? Would acting under Hippocrates then make a doctor a hypocrite?
Because of this subjectivity, doctors sometimes feel uncertain about administering euthanasia. Even if a patient is under a lot of pain and medication, how can doctors be sure that their decision was made rationally? In a Dutch article , an experienced psychiatrist dealing with a patient’s invisible suffering made him uncertain about assessing how deeply rooted their suffering really was, and therefore how moral it would be to allow euthanasia to happen. The fickle nature of the human mind makes many physicians and ethicists question whether or not euthanasia should be a normal practice.
Physicians often have their own reservations about euthanasia and how they cope with patients who wish for it. They frequently feel pressured by the patient or the patient’s relatives to perform euthanasia. A 2011 survey among Dutch physicians also found that 86% of physicians dread the emotional burden of performing euthanasia. One physician recounts how a patient told them, “If you won’t perform euthanasia, I might go to a railway line or climb a high building.” This form of blackmail can lead to dangerous expectations, where future normativity of the practice is anticipated or even praised.
Instead of placing the burden on doctors, what if the government or even robots could control euthanasia? Although this faceless jurisdiction seems like a good solution, critics argue that euthanasia would be normalized and twisted for eugenic purposes, adding to the nightmare of AI domination and impeding the sanctity and preciousness of life. These speculations seem inconceivable, but history has unfortunately seen it happen, such as in Hitler’s Germany, where Aktion T4, a Euthanasia Program systematically murdered patients with disabilities to restore the “integrity” of the German nation, thrived. Perhaps then a grimmer alternative to the use of euthanasia is the elimination of incurable, disabled, or elderly patients. Mechanization of euthanasia would also impact the patient and the medical profession, both in what it means to be human and obeying the Hippocratic Oath. Routinization of the practice could also increase the desires of people’s wishes to end their lives, whether individually justified or not.
References:
https://jamanetwork.com/journals/jama/article-abstract/2532018
https://plato.stanford.edu/entries/euthanasia-voluntary/#MoraCaseForVoluEuth
http://www.cirugiaycirujanos.com/frame_esp.php?id=308
https://www.sciencedirect.com/science/article/pii/S0885392414003066?via%3Dihub
https://www.healthline.com/health/what-is-euthanasia#making-a-decision
https://livinganddyingwell.org.uk/wp-content/uploads/2020/02/Redefining-Physicians-Role-in-Assisted-Dying.pdf
https://shibbolethsp.jstor.org/start?entityID=urn%3Amace%3Aincommon%3Aucsd.edu&dest=
https://www.jstor.org/stable/3561966&site=jstor
https://doi.org/10.1177%2F0269216310397688
https://www.medicalnewstoday.com/articles/182951#some-statistics
https://journals.sagepub.com/doi/10.1177/0269216310397688
https://www.nejm.org/doi/10.1056/NEJMclde1310667
https://medicine.missouri.edu/centers-institutes-labs/health-ethics/faq/euthanasia
https://news.gallup.com/poll/211928/majority-americans-remain-supportive-euthanasia.aspx
https://www.ama-assn.org/delivering-care/ethics/euthanasia
https://pubmed.ncbi.nlm.nih.gov/21145197/
https://doi.org/10.1016/j.jpainsymman.2014.04.016
https://www.ccsenet.org/journal/index.php/gjhs/article/view/19405/13366
https://encyclopedia.ushmm.org/content/en/article/euthanasia-program
Tips on How to Write a Euthanasia Argumentative Essay

Abortion, birth control, death sentencing, legalization of medical marijuana, and gender reassignment surgery remain the most controversial medical issues in contemporary society. Euthanasia is also among the controversial topics in the medical field. It draws arguments from philosophy, ethics, and religious points of view.
By definition derives from a Greek term that means good death, and it is the practice where an experienced medical practitioner or a physician intentionally ends an individual's life to end pain and suffering. The names mercy killing or physician-assisted suicide also knows it.
Different countries have different laws as regards euthanasia. In the UK, physician-assisted suicide is illegal and can earn a medical practitioner 14 years imprisonment. All over the world, there is a fierce debate as regards mercy killing.
Like any other controversial topic, there are arguments for and against euthanasia. Thus, there are two sides to the debate. The proponents or those for euthanasia believe it is a personal choice issue, even when death is involved.
On the other hand, those against euthanasia or the opponents believe that physicians must only assist patients when the patients are sound to make such a decision. That is where the debate centers.
This article explores some of the important basics to follow when writing an exposition, argumentative, persuasive, or informative essay on euthanasia.
Steps in Writing a Paper on Euthanasia
When assigned homework on writing a research paper or essay on euthanasia, follow these steps to make it perfect.
1. Read the Prompt
The essay or research paper prompt always have instructions to follow when writing any academic work. Students, therefore, should read it to pick up the mind of the professor or teaching assistant on the assigned academic task. When reading the prompt, be keen to understand what approach the professor prefers. Besides, it should also tell you the type of essay you are required to write and the scope.
2. Choose a Captivating Topic
After reading the prompt, you are required to frame your euthanasia essay title. Make sure that the title you choose is captivating enough as it invites the audience to read your essay. The title of your essay must not divert from the topic, but make it catchy enough to lure and keep readers. An original and well-structured essay title on euthanasia should give an idea of what to expect in the body paragraphs. It simply gives them a reason to read your essay.
3. Decide on the Best Thesis Statement for your Euthanasia Essay
Creating a thesis statement for a euthanasia essay does not deviate from the conventions of essay writing. The same is consistent when writing a thesis statement for a euthanasia research paper. The thesis statement can be a sentence or two at the end of the introduction that sums up your stance on the topic of euthanasia. It should be brief, well crafted, straight to the point, and outstanding. Right from the start, it should flow with the rest of the essay and each preceding paragraph should support the thesis statement.
4. Write an Outline
An outline gives you a roadmap of what to write in each part of the essay, including the essay hook, introduction, thesis statement, body paragraphs, and the conclusion. We have provided a sample euthanasia essay outline in this article, be sure to look at it.
5. Write the First Draft
With all ingredients in place, it is now time to write your euthanasia essay by piecing up all the different parts. Begin with an essay hook, then the background information on the topic, then the thesis statement in the introduction. The body paragraphs should each contain an idea that is well supported with facts from books, journals, articles, and other scholarly sources. Be sure to follow the MLA, APA, Harvard, or Chicago formatting conventions when writing the paper as advised in the essay prompt.
6. Proofread and Edit the Essay
You have succeeded in skinning the elephant, and it is now time to cut the pieces and consume. Failure to proofread and edit an essay can be dangerous for your grade. There is always an illusion that you wrote it well after all. However, if you take some time off and come to it later, you will notice some mistakes. If you want somebody to proofread your euthanasia essay, you can use our essay editing service . All the same, proofreading an essay is necessary before turning the essay in.
Creating a Euthanasia Essay or Research Paper Outline
Like any other academic paper, having a blueprint of the entire essay on euthanasia makes it easy to write. Writing an outline is preceded by choosing a great topic. In your outline or structure of argumentative essay on euthanasia, you should highlight the main ideas such as the thesis statement, essay hook, introduction, topic sentences for the body paragraphs and supporting facts, and the concluding remarks. Here is a sample outline for a euthanasia argumentative essay.
This is a skeleton for your euthanasia essay:
Introduction
- Hook sentence/ attention grabber
- Thesis statement
- Background statement (history of euthanasia and definition)
- Transition to Main Body
- The legal landscape of euthanasia globally
- How euthanasia affects physician-patient relationships
- Biblical stance on euthanasia
- Consequences of illegal euthanasia
- Ethical and moral issues of euthanasia
- Philosophical stance on euthanasia
- Transition to Conclusion
- Restated thesis statement
- Unexpected twist or a final argument
- Food for thought
Sample Euthanasia Essay Outline
Title: Euthanasia is not justified
Essay hook - It is there on TV, but did you know that a situation could prompt a doctor to bring to an end suffering and pain to a terminally ill patient? There is more than meets the eye on euthanasia.
Thesis statement : despite the arguments for and against euthanasia, it is legally and morally wrong to kill any person, as it is disregard of the right to life of an individual and the value of human life.
Paragraph 1: Euthanasia should be condemned as it ends the sacred lives of human beings.
- Only God gives life and has the authority to take it and not humans.
- The bible says, Thou shalt not kill.
- The Quran states, "Whoever killed a Mujahid (a person who is granted the pledge of protection by the Muslims) shall not smell the fragrance of Paradise though its fragrance can be smelt at a distance of forty years (of traveling).
Paragraph 2: Euthanasia gives physicians the power to determine who lives and who dies.
- Doctors end up playing the role of God.
- It could be worse when doctors make mistakes or advance their self-interests to make money. They can liaise with family members to kill for the execution of a will.
Paragraph 3: it destroys the patient-physician relationship
- Patients trust the doctors for healing
- When performed on other patients, the remaining patients lose trust in the same doctor of the facility.
- Under the Hippocratic Oath, doctors are supposed to alleviate pain, end suffering, and protect life, not eliminate it.
Paragraph 4: euthanasia is a form of murder
- Life is lost in the end.
- There are chances that when tried with other therapeutic and non-therapeutic approaches, terminally ill patients can always get better.
- It is selfish to kill a patient based on a medical report, which in itself could be erratic.
- Patients respond well to advanced care approaches.
Paragraph 5: ( Counterargument) euthanasia proponents argue based on relieving suffering and pain as well as reducing the escalating cost of healthcare.
- Euthanasia helps families avoid spending much on treating a patient who might not get well.
- It is the wish of the patients who have made peace with the fact that they might not recover.
Conclusion
In sum, advancement in technology in the medical field and the existence of palliative care are evidence enough that there is no need for mercy killing. Even though there are claims that it ends pain and suffering, it involves killing a patient who maybe could respond to novel approaches to treatment.
Abohaimed, S., Matar, B., Al-Shimali, H., Al-Thalji, K., Al-Othman, O., Zurba, Y., & Shah, N. (2019). Attitudes of Physicians towards Different Types of Euthanasia in Kuwait. Medical Principles and Practice , 28 (3), 199-207.
Attell, B. K. (2017). Changing attitudes toward euthanasia and suicide for terminally ill persons, 1977 to 2016: an age-period-cohort analysis. OMEGA-Journal of Death and Dying , 0030222817729612.
Barone, S., & Unguru, Y. (2017). Should Euthanasia Be Considered Iatrogenic? AMA journal of ethics, 19(8), 802-814.
Emanuel, E. (2017). Euthanasia and physician-assisted suicide: focus on the data. The Medical Journal of Australia , 206 (8), 1-2e1.
Inbadas, H., Zaman, S., Whitelaw, S., & Clark, D. (2017). Declarations on euthanasia and assisted dying. Death Studies, 41 (9), 574-584.
Jacobs, R. K., & Hendricks, M. (2018). Medical students' perspectives on euthanasia and physician-assisted suicide and their views on legalising these practices in South Africa. South African Medical Journal , 108 (6), 484-489.
Math, S. B., & Chaturvedi, S. K. (2012). Euthanasia: the right to life vs right to die. The Indian journal of medical research, 136 (6), 899.
Reichlin, M. (2001). Euthanasia in the Netherlands. KOS , (193), 22-29.
Saul, H. (2014, November 5). The Vatican Condemns Brittany Maynard's Decision to end her Life as �Absurd'.
Sulmasy, D. P., Travaline, J. M., & Louise, M. A. (2016). Non-faith-based arguments against physician-assisted suicide and euthanasia. The Linacre Quarterly, 83 (3), 246-257.
Euthanasia Essay Introduction Ideas
An introduction is a gate into the compound of your well-reasoned thoughts, ideas, and opinions in an essay. As such, the introduction should be well structured in a manner that catches the attention of the readers from the onset.
While it seems the hardest thing to do, writing an introduction should never give you the fear of stress, blank page, or induce a writer's block. Instead, it should flow right from the essay hook to the thesis statement.
Given that you can access statistics, legal variations, and individual stories based on personal experiences with euthanasia online, writing a euthanasia essay introduction should be a walk in the park.
Ensure that the introduction to the essay is catchy, appealing, and informative. Here are some ideas to use:
- Rights of humans to life
- How euthanasia is carried out
- When euthanasia is legally allowed
- Stories from those with experience in euthanasia
- The stance of doctors on euthanasia
- Definition of euthanasia
- Countries that allow euthanasia
- Statistics of physicians assisted suicide in a given state, locality, or continent.
- Perception of the public given the diversity of culture
There are tons of ideas on how to start an essay on euthanasia. You need to research, immerse yourself in the topic, and scoop the best evidence. Presenting facts in an argumentative essay on euthanasia will help convince the readers to argue for or against euthanasia. Based on your stance, make statements in favor of euthanasia or statements against euthanasia known from the onset through the strong thesis statement.
Essay Topics and Ideas on Euthanasia
- Should Euthanasia be legal?
- What are the different types of euthanasia?
- Is euthanasia morally justified?
- Cross-cultural comparison of attitudes and beliefs on euthanasia
- The history of euthanasia
- Euthanasia from a Patient's Point of View
- Should euthanasia be considered Iatrogenic?
- Does euthanasia epitomize failed medical approaches?
- How does euthanasia work?
- Should Physician-Assisted Suicide be legal?
- Sociology of Death and Dying
- Arguments for and against euthanasia and assisted suicide
- Euthanasia is a moral dilemma
- The euthanasia debate
- It Is Much Better to Die with Dignity Than to Live with Pain Essay
- Euthanasia Is a Moral, Ethical, and Proper
- Euthanasia Law of Euthanasia in California and New York
- Effect of Euthanasia on Special Population
- Euthanasia is inhuman
- Role of nurses in Euthanasia
- Are family and relative decisions considered during the euthanasia
- The biblical stance on euthanasia
Related Articles:
- Argumentative essay topics and Ideas
- Topics and ideas for informative essays
Get Help with Writing Euthanasia Argumentative Essay for School
We have covered the tips of writing an argumentative essay on euthanasia. Besides, we have also presented a sample euthanasia essay outline, which can help you write your essay. However, sometimes you might lack the motivation to write an essay on euthanasia, even when you have access to argumentative essay examples on euthanasia.
It is the right time to pay someone to write your argumentative essay . We have the best essay writers who have expertise in creating the best argumentative essays on any topic. They understand the entire process of argumentative writing and can create a top-grade euthanasia essay within the shortest turnaround time.
Do not wait until it is too late; let our nerds help you ace your homework. Order an essay today and forget your academic writing woes.
Order Essay on Euthanasia!
Gradecrest is a professional writing service that provides original model papers. We offer personalized services along with research materials for assistance purposes only. All the materials from our website should be used with proper references. See our Terms of Use Page for proper details.
The Ethical and Legal Implications of Euthanasia

Generally, the topic of euthanasia has resulted in hot debates among all stakeholders, including healthcare professionals and legal experts, due to the ethical and legal issues associated with the topic. It affects both patients and their healthcare providers. Over the years, the debate on euthanasia has focused on suffering patients with terminal illnesses. However, the topic has extended to include even patients with mental illnesses like depression. Therefore, it is appropriate to look at the controversy surrounding euthanasia in a recent case study. Euthanasia is a controversial topic that requires further inquiry to fully understand different opinions offered by the opposing sides and the ethical implications associated with it.
Recent Case Study
The case published in the Catholic Herald involves a 29-year-old woman who underwent euthanasia following a series of mental illnesses. According to the author, despite being physically fit, the woman was given a lethal injection, having been granted her wish to die by the court after eight years of legal battles. In her argument, the woman claimed she had experienced extreme bouts of depression that had made her life intolerable. The case raised concerns among various stakeholders, including politicians who lamented how dangerous euthanasia could be.
Ethical Issues Involved in the Case Study
Generally, the case study raises various ethical dilemmas related to euthanasia, including when it is justifiable to end one’s life. In addition, the topic also opens up a whole discussion on the limitations of patients’ autonomy and the ethical responsibilities of healthcare professionals, as highlighted in the bioethical principles of beneficence and maleficence. Concerning autonomy, questions are raised regarding the patient’s capability to understand the decision that she was making. With superior knowledge and training, the physician is best positioned to help make an ethical decision that is in the patient’s best interest to protect patients from irresponsible choices. For patients to make an autonomous decision, they should be mentally capable of comprehending the information of the decision. In the case study, the patient has a mental health condition. Hence, her ability to make rational decisions is in question.
The Context of Euthanasia
The case study highlights euthanasia, particularly among patients with mental conditions such as depression. Historically, numerous attempts have been made to legalize euthanasia, but minimal success has occurred. The euthanasia discussion in psychiatry was awakened after the Nazi Holocaust when thousands of psychiatric patients were gassed or poisoned to death under the ‘euthanasia program’. According to Felder, the Nazi euthanasia program was used by scientists, mainly physicians, to conduct medical experiments. It is out of the scientific experiments of the Nazi physicians that ‘The Nuremberg Code’ was established to guide future experiments on human subjects.
Additionally, politicians have had their hand in the matter by sponsoring bills to legalize the act, with some opposing such attempts and publicly making their views known. From a social perspective, euthanasia has continued to be controversial, with many societies coming up to air their opinion. In the traditional Christian context and culture, euthanasia is viewed as morally unacceptable due to human life’s sacred nature. However, other social groups support euthanasia with the thought of extending dignity to death, such as the Voluntary Euthanasia Society. As such, there is no single available societal perspective regarding the issue of euthanasia. Hence, it is important to society as it touches on the critical matters of life and death.
The Differing Perspectives on Euthanasia
The individuals and societies in support of euthanasia have always centered their opinion on patient suffering. They argue that patients in the terminal stages of illness experience excruciating pain and have poor wound healing, poor social interactions, and many other aspects of physical suffering. According to the proponents, euthanasia is a more merciful response to relieve this suffering, especially where the quality of life is jeopardized. Among the patients with mental illnesses, the proponents argue that some mental conditions, including severe depression, induce intense suffering and are unresponsive to treatment. Additionally, the proponents note that since the patients request most cases of euthanasia, it is a way for physicians to show respect for personal autonomy. Thus, to the proponents, euthanasia relieves undue suffering and is in harmony with respect for autonomy and the individual’s right to a dignified death.
Contrary to the proponents’ arguments, the opponents base their argument on the intrinsic wrongness of killing, professional integrity, and the possibility of potential abuse. According to Naga and Mrayyan, willingly ending one’s life is inconsistent with human rights, and alternatives should be sought to relieve the patient’s suffering and improve their quality of life. Furthermore, Naga and Mrayyan note that administering lethal substances by physicians to end life is unethical according to guiding medical ethical practices, especially the Hippocratic Oath that restricts physicians from administering such substances to their patients or aiding their patients to die. They also note that legalizing euthanasia could lead to its potential abuse and a slippery slope where individuals will use it to escape chronic but manageable medical conditions.
Evaluation of the Arguments and Their Ethical Implications
The arguments presented by both the proponents and the opponents seem to be entirely influenced by one’s culture, moral philosophy, and personal experiences. Those opposed to euthanasia seem to be influenced by their religious cultures. Specifically, Christian teachings view life as sacred and state it should not be terminated prematurely at any cost. On the other hand, the proponents seem to subscribe to the Stoic philosophy that has always defended suicide as a reasonable departure from life, especially when intense suffering is involved. Anecdotal evidence also suggests that personal life experiences with suffering may make one choose to end one’s life. For example, seeing a cancer patient suffer may make individuals consider euthanasia if diagnosed with a similar terminal disease, as they will not want to experience the same ordeal.
While both the proponents and those opposed to euthanasia have valid arguments, myriads of ethical issues surround each side’s perspective. It is indeed true that certain illnesses, including mental conditions, lead to severe suffering and reduced quality of life. However, ethical issues arise regarding the ability of the patients requesting euthanasia to make autonomous decisions. For example, Appelbaum notes that it is common for depressed patients to reject treatment and even request death, yet change their decision once the depression is resolved. Accordingly, this raises the ethical question concerning the impact of the mental illness itself on the patient’s decision-making. It has also been observed that most patients are only resistant to one form of treatment and that other options should be tried to relieve their suffering.
Furthermore, it is noted that the right to autonomy is not always absolute and that physicians have the legal and ethical responsibility to override the patient’s decisions and continue pursuing alternative treatment in response to the patient’s symptoms and request a dignified death. Thus, the argument regarding patients’ autonomy to end their lives is weak. On the other hand, the opponents’ unethical medical practice mainly touches on physicians’ ethical responsibilities to act in good faith and protect their patients from harm. In line with non-maleficence and beneficence principles, physicians cannot administer lethal dosages to their patients as it causes more harm than good. Additionally, the claim of potential abuse if euthanasia is legalized, holds grounds owing to several reported cases, including ones with mental illnesses, where euthanasia has been performed without following due process in countries where it is legalized. Thus, the ethical questions raised by those opposed to euthanasia regarding non-maleficence, benevolence, and potential abuse are strongly supported by evidence.
Personal Perspective on Euthanasia
The issue of euthanasia among depressed patients will continue to dominate medical discussions. Subjectively, the opponents of euthanasia seem to offer a strong argument. Notably, depression can be treated just like other mental conditions, and symptoms can be controlled where treatment is impossible. Patient autonomy among psychiatric patients is in question. Mental illnesses tend to affect one’s way of thinking, and suicidal ideations are common phenomena among depressed patients. I have dealt with patients who have changed their stance on ‘mercy killing’ after a series of professional counseling sessions and continued treatment. Thinking about these experiences concerning my patients and the ethical dilemmas related to euthanasia makes me view it as an undesirable event in medical practice that I will not want to engage in.
The topic of euthanasia is controversial based on the numerous arguments aired by those in its support and those who are against it. The case study published in the Catholic Herald offers a good scenario through which the effects of euthanasia can be accessed and its ethical implications reviewed. While the Pro-euthanasia argument is based on the need to relieve undue suffering, respect autonomy, and grant the right to a dignified death, the opponents have emphasized the intrinsic wrongness of killing, professional integrity, and the possibility of a “slippery slope”. Overall, the ethical issues addressed autonomy, beneficence, and non-maleficence. Subjectively, the ethical questions touching upon professional integrity, especially the need to observe non-maleficence and doing good, are strong enough to make me offer my support against euthanasia.
📎 References:
1. Appelbaum, P. S. (2017). Should mental disorders be a basis for physician-assisted death? Law & Psychiatry, 68(4), 315-317. https://doi.org/10.1176/appi.ps.201700013 2. Beauchamp, T. L. (2016) Principlism in bioethics. In P. Serna & J. A. Seoane (Eds.), Bioethical decision making and argumentation (pp. 1-16). New York, NY: Springer. 3. Caldwell, S. (2018, February 1). Dutch doctors euthanize a 29-year old woman with depression. Catholic Herald. 4. Felder, B. M. (2013). “Euthanasia,” human experiments, and psychiatry in Nazi-occupied Lithuania, 1941-1944. Holocaust and Genocide Studies, 27(2), 242-275. https://doi.org/10.1093/hgs/dct025 5. Kim, S. Y., De Vries, R. G., & Peteet, J. R. (2016). Euthanasia and assisted suicide of patients with psychiatric disorders in the Netherlands 2011 to 2014. JAMA Psychiatry, 73(4), 362-368. https://doi.org/10.1001/jamapsychiatry.2015.2887 6. Naga, B. S. B., & Mrayyan, M. T. (2013). Legal and ethical issues of euthanasia: Argumentative essay. Middle East Journal of Nursing, 7(5), 31-39. https://doi.org/10.5742/MEJN.2013.75330 7. Nunes R., & Rego, G. (2016.) Euthanasia: A challenge to medical ethics. Journal of Clinical Research & Bioethics, 7(4), 1-5. https://doi.org/10.4172/2155-9627.1000282 8. Tomasini, F. (2014). Stoic defence of physician-assisted suicide. Acta Bioethica, 20(1), 99-108. Retrieved from https://scielo.conicyt.cl/pdf/abioeth/v20n1/art11.pdf
Table of content
Crafted with Care:
Nursing Essays!
Precision, Passion, & Professionalism in Every Page.
Euthanasia - Essay Samples And Topic Ideas For Free
Euthanasia, also known as assisted dying or mercy killing, remains a deeply contested ethical and legal issue. Essays could delve into the various forms of euthanasia, such as voluntary, non-voluntary, and involuntary euthanasia, discussing the moral and legal implications of each. The discourse might extend to the examination of the cultural, religious, and societal attitudes towards euthanasia, exploring how different societies and religious groups perceive the right to die. Discussions could also focus on the experiences of countries and regions that have legalized euthanasia, examining the impact on healthcare practices, legal frameworks, and societal attitudes. Moreover, the broader implications of euthanasia on medical ethics, patient autonomy, and the sanctity of life could be explored to provide a comprehensive understanding of the complexities surrounding euthanasia and the ongoing debates on its legalization and practice. A substantial compilation of free essay instances related to Euthanasia you can find at Papersowl. You can use our samples for inspiration to write your own essay, research paper, or just to explore a new topic for yourself.
Euthanasia: is it Ethical
While doing research on the topic of Euthanasia and Physician Assisted Suicide, I have come to see that people have a hard time believing that this should be an option for people who have terminal illnesses. Euthanasia is the painless killing of a patient suffering from an incurable and painful disease or in an irreversible coma and Physician Assisted Suicide (PAS) is The voluntary termination of one's own life by administration of a lethal substance with the direct or indirect […]
Arguments for and against Euthanasia
Euthanasia is also known as physician-assisted suicide or good death. It refers to the method where animals that are suffering or in discomfort are helped to rest in death. Many pet owners consider Euthanasia a more compassionate manner of bidding their beloved animals goodbye. In the case of people, many states have not legalized euthanasia for people with dementia or those suffering from incurable diseases. Euthanasia creates an ethical dilemma on three main lines: legal, medical, and philosophical. There are […]
Ethics Behind Physician-Assisted Suicide
Assisted suicide is the act of intentionally killing yourself with the assistance of someone else. In the United States, physician-assisted suicide is when a physician provides a patient, who meets the criteria of having a terminal illness, with medication in order to terminate their life to relieve pain and/or suffering. Physician-assisted suicide is often confused with euthanasia. Euthanasia is illegal in the US. It requires a doctor, or another individual, to administer the medication to the patient. Other terms for […]
We will write an essay sample crafted to your needs.
Why Euthanasia should be Legalised
Did you know that the word euthanasia comes from Greek which means good death? However, Only 9 out of the 196 countries in the world have legalised euthanasia or assisted death, including the Netherlands, Belgium, Switzerland and Japan. - posted on Deccan Chronicle. These are all first world countries that value freedom and I strongly believe that Euthanasia should be extended to all other countries. There are 4 different types of euthanasia voluntary, involuntary, active and passive euthanasia. First, I […]
The Ban on Euthanasia
Imagine your girl best friend gets into a car crash. After the incident, you find out she suffered major spinal cord damage and her legs will be paralyzed for the rest of her life. You go to visit her in the hospital the same week but arrive to shocking news. She tells you she has lost the will to live and wants to be euthanized, or painlessly killed. She tells you she is worried about how this accident will affect […]
Assisted Suicide the Rights we have
The right to assisted suicide is one of the most controversial topics ever discussed because of the fact that other people control your life when you are unable to. But some people think that they can stop you from dying even though death is inevitable when one is terminally ill. They think that because of religious and moral reasons they could stop someone from ending their own life. Assisted suicide also known as ""Euthanasia"" is used to make a painless […]
Economic Benefits of Euthanasia
Euthanasia is assisted suicide, it is an action taken by a doctor with consent of the patient in order to relieve immense pain and suffering. However, is the overall process of Euthanasia beneficial for the economy? Based on research, euthanasia is beneficial to the economy, and saves a vast amount of money for families for hospital stays, private insurance companies, taxpayers, and medicare each year. For a hospital stay, the average cost per inpatient day is $2,534.00 for a local […]
Euthanasia Debate
The intention to deliberately help someone accelerate the death of an incurable patient, even to stop his or her suffering has never been an easy task. The ethics of euthanasia is one that has been debated over since the fourth century B.C. Euthanasia is translated from Greek as "good death" or "easy death. At first, the term referred to painless and peaceful natural deaths in old age that occurred in comfortable and familiar surroundings. Today the word is currently understood […]
Physician-assisted Suicide: Right to Die
You may have heard of Physician-assisted suicide before, but what exactly is it? Physician-Assisted suicide is when someone who is terminally ill and completely competent of making choices the right to take their own life, legally with the help of a doctor. Though it seems as if they should be able to do that, in most states the law does get in the way of that. There are ethical and moral issues surrounding this issue. Regardless of those issues, those […]
Religious Perspectives on Euthanasia
Death is one of the most important things that religions deal with. All faiths offer meaning and explanations for death and dying; all faiths try to find a place for death and dying within human experience. Most religions disapprove of euthanasia. Some of them absolutely forbid it. Virtually all religions state that those who become vulnerable through illness or disability deserve special care and protection and that proper end of life care is a much better thing than euthanasia. Religions […]
Active and Passive Euthanasia
Euthanasia is the termination of a terminally ill person's life in order to relieve patients of their severe and untreatable pain. It is further broken down into two types: active and passive. In this paper, I will be focusing on active euthanasia and will argue that it is morally justifiable for a physician to alleviate agony for a patient and their family via direct action. Active euthanasia is morally permissible when a patient explicitly states their consent due to the […]
Physician Assisted Suicide: Medical Practice
Physician assisted suicide is when a physician provides a patient with the necessary means and information to help the patient perform a life ending act. Physician assisted suicide is when is when a person gets prescribed a lethal dose of medication from their physician that they can take when they get ready too. Physician assisted suicide has become an option for those around the world and even legal in certain States in the US. This option is legal in 6 […]
The Controversy over Euthanasia
Euthanasia, as defined by the Merriam-Webster Dictionary, is the act or practice of killing or permitting the death of hopelessly sick or injured individuals (such as persons or domestic animals) in a relatively painless way for reasons of mercy. The growing euthanasia epidemic has raised a profusion of controversy in recent years due to the legal and moral implications. Although described as relatively painless,euthanasia is something that should be methodically and thoroughly thought through because of the permanent effect it […]
Euthanasia and Death Penalty
Euthanasia and death penalty are two controversy topics, that get a lot of attention in today's life. The subject itself has the roots deep in the beginning of the humankind. It is interesting and maybe useful to learn the answer and if there is right or wrong in those actions. The decision if a person should live or die depends on the state laws. There are both opponents and supporters of the subject. However different the opinions are, the state […]
Physician Assisted Suicide: the Growing Issue of Dying with Dignity and Euthanasia
Is someone wanting to die with dignity more important than the conscience of a doctor who provides care for others? The issue of physician-assisted death can be summed up by simply saying it has a snowball effect. What starts as physician-assisted death turns into euthanizing and from there it could end up in the killing of patients without their full comprehension as to what they agreed to. The solution to this issue is accepting there is a problem and figuring […]
Definition of Euthanasia
Euthanasia defined as an intentionally ending of the life of the terminally ill person in order to relieve pain or suffering, done by a physician, legally. This is not to be confused with the similar physician assisted suicide, the suicide of patient suffering from an incurable disease, effected by the taking of lethal drug by a doctor for this purpose. It is legal in only a few places of the world, and the laws vary by the places. That means […]
Physician Assisted Suicide
Healthcare isn't as perfect as we think it should be considering there are so many medications and treatments that can help restore or cure one's illness. When needing the assistance of a healthcare facility, there are many different challenges that can impact patients and their families. Challenges that include life or death decision making, insurance coverage, the need for medications, cost of services, and so on. As these challenges may seem as if they are minor to some, they truly […]
Euthanasia and Physician-Assisted Suicide
In a documentary, Charles Scott was a man who loved to read, sing, and enjoy being outdoors. He was diagnosed with lymphoma. Struggling every day just to breathe after walking 10 steps to the bathroom and dealing with his eyesight deteriorating, He found life to be full of pain instead of joy. He found no want in having to wait through multiple medications, operations, pain, hospice, and finally him dying suffocating trying to catch his breath” he wished to die […]
Physician-Assisted Euthanasia/Suicide
Part 1: Ethical Question Should doctors have a choice to opt out of assisting terminally ill patients with euthanasia/suicide? Part 2: Introduction Some people think being a physician is an exciting job for the most part. However, physicians have the task of making tough decisions that could hurt many people emotionally. The morality of assisted euthanasia and suicide has been questioned by many people. Some may consider euthanasia and suicide immoral any wrong. Unfortunately, euthanasia and suicide may be the […]
Arguments for Legalizing Euthanasia
I once heard euthanasia is a heart-wrenching kindness and i believe that to be true.Although we as vet techs know it is the right thing to do, being apart of ending there pain and suffering,it is hard being the one to end it knowing the bond an animal has with its owner.Everyone has their own thoughts about this topic and how we prefer to handle it.There are different tolerances everyone has on how it should be done and what the […]
Why Active Euthanasia and Physician Assisted Suicide should be Legalized
This reference source gives us an overview of why euthanasia should be legalized. It goes into depth about how patients and doctors are affected by the decision to end a person's life, and moral issues, and whether it is right or wrong to purposely end someone's life. This source highlights that euthanasia should be in the best interest of the patient who is suffering from an illness, such as an incurable disease or a serious health issue. Doctors should be […]
Physician-assisted Suicide is not Federally Mandated
Physician-assisted suicide is not federally mandated due to the lack of bipartisanship in Congress, the principles of federalism, and contributions from conservative organizations and interest groups. The attitudes and moral acceptability about certain behaviors and actions differ significantly among Republicans and Democrats. According to a 2007 survey, 62% of Democrats support doctors assisting a terminally ill patient to commit suicide, while only 49% of Republicans support this notion (Gallup, Inc 2007). 59% of Democrats also find physician-assisted suicide to be […]
Physician-assisted Suicide and Euthanasia
Physician-assisted suicide and euthanasia have become some of the most highly controversial topics discussed in medicine, making those who have medicine as an occupation question the morality behind the act. A common misconception people often times make is confusing the fact that physician-assisted suicide and voluntary active euthanasia as the same thing. The NCI dictionary of cancer terms states euthanasia is accessibility to ""[a]n easy or painless death or the intentional ending of the life of a person suffering from […]
Euthanasia and Physician Assisted Suicide
Sometimes people criticize euthanasia and physician-assisted suicide from what is called "pro-life" perspectives and other times from "pro-death" perspectives; each perspective has a different argument about their position and the side they are on in this debate. This paper will review some of these arguments that have been made to date, as well as some of the more recent developments in this issue (Dieterle 129). To begin with, many people argue that euthanasia and physician-assisted suicide are morally acceptable because […]
Hinduism and Buddhist Perspective of Suicide and Euthanasia
The principle of ahimsa, or no violence, is fervently held in Hinduism and is reflective in followers' everyday lives. This concept extends to oneself as well as others. For one, suicide is condemned in this religion because all life is considered sacred. Humans life is perceived as precious because only through one of the three human realms can liberation be achieved. Other living things, such as insects and animals, do not receive the same opportunity, so it is crucial followers […]
Euthanasia – One of the most Debated Topics Today
The topic of euthanasia is one of the most debated topics today. Elderly patients can be pressured into a decision they don't want to make. Citizens can also be unfairly euthanized as well. Euthanasia should stay illegal due to the obligation to elderly patients, non permitted euthanization, of an individual, and which can open hopefully widen perspective on this issue, as well as many others. Euthanasia is a complex topic that can't be described simply and without depth. Euthanasia can […]
Physician-assisted Suicide Debate
Let's say a patient is in incredible pain or has an incurable illness and the patient can only be kept alive by machines or by enduring their pain. Should any patient who is in these circumstances be allowed to choose death over this life? Many people go against assisted suicide because of religion and or whatever they believe in. Another reason why people may disagree is that the patients who are not in the right mind and or are too […]
Ethics and Challenges of Euthanasia
As there are other patients who have a higher chance of living, euthanizing the patient was the more practical option. Euthanasia advocates argue that futile care may harm others. For instance, a young child with an acute respiratory disease, who has a potentially higher chance of getting cured, could not get a bed and ventilator in the ICU because others were using it even though they are not getting any personal benefit from the treatment (Niederman & Berger, 2010). This […]
Euthanasia: Merciful Death or Playing God
A death by suicide. Just hearing the word suicide can send chills down one's spine. How could someone get to the point of self-termination? Why would anybody ever consider such a terrible way to die? The thing is, suicide does not have to be a terrible or scary way to die if one is faced with insurmountable troubles accompanying an untreatable disease. With assistance from licensed professionals, it can give those suffering a painless option if they so choose to […]
What is Euthanasia?
Euthanasia is a easy death, some may say euthanasia is a undeviating act for taking a life through prescription drugs. A patient that has a short expand of life can address such an issue with their healthcare provider. Counseling can be provided before the final decision is made by doctor and the patient. At anytime the patient reserves the right to with draw from the process. The patient however must have good reason for the process before a doctor will […]
Additional Example Essays
- End Of Life Ethical Issues
- Socioautobiography Choices and Experiences Growing up
- A Class Divided
- Gender Inequality in Education
- Does Arrest Reduce Domestic Violence
- Homelessness in America
- New Imperialism
- Solutions to Gun Violence
- Catherine Roerva: A Complex Figure in the Narrative of Child Abuse
- The Mental Health Stigma
- Psychiatric Nurse Practitioner
- Substance Abuse and Mental Illnesses
How To Write An Essay On Euthanasia
Introduction to the concept of euthanasia.
When embarking on an essay about euthanasia, it’s crucial to begin with a clear definition of what euthanasia entails. Euthanasia, often referred to as "mercy killing," is the act of intentionally ending a person's life to relieve them of suffering, typically from a terminal illness or an incurable condition. In your introduction, outline the various types of euthanasia, such as voluntary, non-voluntary, and involuntary, and the ethical, legal, and moral questions they raise. This introductory segment sets the stage for an in-depth exploration of the arguments for and against euthanasia and its implications in the realms of medicine, ethics, and law.
Exploring the Arguments For and Against Euthanasia
The body of your essay should delve into the complex arguments surrounding euthanasia. On one hand, proponents argue that euthanasia is a compassionate response to unbearable suffering, respecting an individual's right to choose death over prolonged pain. They may also cite the importance of dignity in death and the reduction of medical costs for terminally ill patients. On the other hand, opponents raise concerns about the sanctity of life, the potential for abuse, and the slippery slope towards non-voluntary or involuntary euthanasia. They may also discuss the moral obligations of medical professionals to preserve life. This section should present a balanced view of the debate, providing a comprehensive understanding of the various perspectives on euthanasia.
Ethical and Legal Considerations
A crucial aspect of your essay should be an examination of the ethical and legal considerations surrounding euthanasia. Discuss the ethical principles involved, such as autonomy, beneficence, non-maleficence, and justice. Explore how different countries and cultures view and legislate euthanasia, noting the variations in legal frameworks and the criteria required for it to be carried out. This analysis should provide insight into the complexities of legalizing and regulating euthanasia, and the ethical dilemmas faced by healthcare providers, patients, and their families.
Concluding with Personal Reflections and Broader Implications
Conclude your essay by summarizing the key points and offering personal reflections on the topic. Reflect on the implications of euthanasia for society and the field of healthcare. Consider how advances in medical technology and changes in societal attitudes might influence the future of euthanasia. Your conclusion should not only provide closure to your essay but also encourage further thought and dialogue on this sensitive and contentious issue, highlighting the ongoing importance of ethical deliberation in decisions about life and death.
1. Tell Us Your Requirements
2. Pick your perfect writer
3. Get Your Paper and Pay
Hi! I'm Amy, your personal assistant!
Don't know where to start? Give me your paper requirements and I connect you to an academic expert.
short deadlines
100% Plagiarism-Free
Certified writers

25,000+ students realised their study abroad dream with us. Take the first step today
Meet top uk universities from the comfort of your home, here’s your new year gift, one app for all your, study abroad needs, start your journey, track your progress, grow with the community and so much more.

Verification Code
An OTP has been sent to your registered mobile no. Please verify

Thanks for your comment !
Our team will review it before it's shown to our readers.
- School Education /
Essay on Euthanasia: 100, 200 and 300 Words Samples
- Updated on
- Feb 22, 2024

Essay on Euthanasia: Euthanasia refers to the act of killing a person without any emotions or mercy. Euthanasia is an ethnically complex and controversial topic, with different perspectives and legal regulations on different topics. School students and individuals preparing for competitive exams are given assigned topics like essays on euthanasia. The objective of such topics is to check the candidate’s perspectives and what punishment should be morally and legally right according to them.

If you are assigned an essay on euthanasia, it means your examiner or teacher wants to know your level of understanding of the topic. In this article, we will provide you with some samples of essays on euthanasia. Feel free to take ideas from the essays discussed below.
Master the art of essay writing with our blog on How to Write an Essay in English .
Table of Contents
- 1 Essay on Euthanasia in 150 Words
- 2.1 Euthanasia Vs Physician-Assisted Suicide
- 2.2 Euthanasia Classification
- 3 Is Euthanasia Bad?
Essay on Euthanasia in 150 Words
Euthanasia or mercy killing is the act of deliberately ending a person’s life. This term was coined by Sir Francis Bacon. Different countries have their perspectives and laws against such harmful acts. The Government of India, 2016, drafted a bill on passive euthanasia and called it ‘The Medical Treatment of Terminally Ill Patient’s Bill (Protection of Patients and Medical Practitioners).
Euthanasia is divided into different classifications: Voluntary, Involuntary and Non-Voluntary. Voluntary euthanasia is legal in countries like Belgium and the Netherlands, with the patient’s consent. On one side, some supporters argue for an individual’s right to autonomy and a dignified death. On the other hand, the opponents raise concerns about the sanctity of life, the potential for abuse, and the slippery slope towards devaluing human existence. The ethical debate extends to questions of consent, quality of life, and societal implications.
Also Read: Essay on National Science Day for Students in English
Essay on Euthanasia in 350 Words
The term ‘Euthanasia’ was first coined by Sir Francis Bacon, who referred to an easy and painless death, without necessarily implying intentional or assisted actions. In recent years, different countries have come up with different approaches, and legal regulations against euthanasia have been put forward.
In 2016, the government of India drafted a bill, where euthanasia was categorised as a punishable offence. According to Sections 309 and 306 of the Indian Penal Code, any attempt to commit suicide and abetment of suicide is a punishable offence. However, if a person is brain dead, only then he or she can be taken off life support only with the help of family members.
Euthanasia Vs Physician-Assisted Suicide
Euthanasia is the act of intentionally causing the death of a person to relieve their suffering, typically due to a terminal illness or unbearable pain.
Physician-assisted suicide involves a medical professional providing the means or information necessary for a person to end their own life, typically by prescribing a lethal dose of medication.
In euthanasia, a third party, often a healthcare professional, administers a lethal substance or performs an action directly causing the person’s death.
It is the final decision of the patient that brings out the decision of their death.
Euthanasia Classification
Voluntary Euthanasia
It refers to the situation when the person who is suffering explicitly requests or consents to euthanasia. A patient with a terminal illness may express his or her clear and informed desire to end their life to a medical professional.
Involuntary
It refers to the situation when euthanasia is performed without the explicit consent of the person, often due to the individual being unable to communicate their wishes.
Non-Voluntary
In this situation, euthanasia is performed without the explicit consent of the person, and the person’s wishes are unknown.
Active euthanasia refers to the deliberate action of causing a person’s death, such as administering a lethal dose of medication.
It means allowing a person to die by withholding or withdrawing treatment or life-sustaining measures.
Euthanasia and assisted suicide are a defeat for all. We are called never to abandon those who are suffering, never giving up but caring and loving to restore hope. — Pope Francis (@Pontifex) June 5, 2019
Also Read: Essay on Cleanliness
Is Euthanasia Bad?
Euthanasia is a subjective term and its perspectives vary from person to person. Different cultures, countries and religions have their own set of values and beliefs. Life is sacred and gifted to us by god or nature. Therefore, intentionally causing death goes against moral and religious beliefs.
However, some people have raised concerns about the potential for a slippery slope, where the acceptance of euthanasia could lead to the devaluation of human life, involuntary euthanasia, or abuse of the practice. Some even argue that euthanasia conflicts with their traditional medical ethics of preserving life and prioritizing the well-being of the patient.
Today, countries like the Netherlands and Belgium have legalised euthanasia. In India, the USA and the UK, it is a punishable offence with varying sentences and fines. Euthanasia is a complex and controversial topic and creating a law against or for it requires a comprehensive study by experts and the opinions of all sections of society.
Ans: Euthanasia refers to the act of killing a person without any emotions or mercy. Euthanasia is an ethnically complex and controversial topic, with different perspectives and legal regulations on different topics.
Ans: The term ‘Euthanasia’ was first coined by Sir Francis Bacon, who referred to an easy and painless death, without necessarily implying intentional or assisted actions. In recent years, different countries have come up with different approaches, and legal regulations against euthanasia have been put forward. In 2016, the government of India drafted a bill, where euthanasia was categorised as a punishable offence. According to Sections 309 and 306 of the Indian Penal Code, any attempt to commit suicide and abetment of suicide is a punishable offence. However, if a person is brain dead, only then he or she can be taken off life support only with the help of family members.
Ans: Belgium and the Netherlands have legalised euthanasia. However, it is banned in India.
Related Articles
For more information on such interesting topics, visit our essay writing page and follow Leverage Edu.

Shiva Tyagi
With an experience of over a year, I've developed a passion for writing blogs on wide range of topics. I am mostly inspired from topics related to social and environmental fields, where you come up with a positive outcome.
Leave a Reply Cancel reply
Save my name, email, and website in this browser for the next time I comment.
Contact no. *

Connect With Us

25,000+ students realised their study abroad dream with us. Take the first step today.

Resend OTP in
Need help with?
Study abroad.
UK, Canada, US & More
IELTS, GRE, GMAT & More
Scholarship, Loans & Forex
Country Preference
New Zealand
Which English test are you planning to take?
Which academic test are you planning to take.
Not Sure yet
When are you planning to take the exam?
Already booked my exam slot
Within 2 Months
Want to learn about the test
Which Degree do you wish to pursue?
When do you want to start studying abroad.
January 2024
September 2024
What is your budget to study abroad?

How would you describe this article ?
Please rate this article
We would like to hear more.
Have something on your mind?

Make your study abroad dream a reality in January 2022 with
India's Biggest Virtual University Fair

Essex Direct Admission Day
Why attend .

Don't Miss Out
- Dissertation
- PowerPoint Presentation
- Book Report/Review
- Research Proposal
- Math Problems
- Proofreading
- Movie Review
- Cover Letter Writing
- Personal Statement
- Nursing Paper
- Argumentative Essay
- Research Paper
- Discussion Board Post
How To Write A Vivid Euthanasia Argumentative Essay?

Table of Contents

Euthanasia (good death from Greek) is the practice of intentional life ending aiming to relieve patients’ pain and suffering. The topic of its use is fiercely debated all over the world.
People have divided into two camps: some say Euthanasia is the matter of choice, even when it comes to choosing death. Another group claims that doctors mustn’t be empowered to offer death to people who may not even realize the decision they make.
Every country where Euthanasia is legal has its own specific legislative base of its use. Nevertheless, there is one aspect of this topic that unites all the people together: the issue is considered from the moral and ethical perspective.
Euthanasia argumentative essay: the basics
The topics for an argumentative essay writing are usually two-sided: voting for or against the topic, agree or disagree with the statement, choose one option or another.
Writing any argumentative assay requires highlighting both possible points of view, no matter what is your own. Remember, you should explain both sides equally correct and impartial.
So let’s take a closer look into the details…
How to write a Euthanasia thesis statement?
Before writing an essay on Euthanasia you have to think about your own attitude towards the topic. It will help you write a good thesis statement.
…Why you need it?
The thesis is the representation of the essay’s main idea. You’ll have to clarify both sides of the topic, sure. Still, you also need to express your own point of view. And that is made with the thesis statement in the first place.
You may clearly state your opinion in the thesis, like:
“Injecting a medication to a hopeless patient is a murder.”
“Taking life from a person who wants to end up sufferings is mercy.”
Also, you can try to intrigue your readers and present your thesis as a question with no answer provided right away. Like:
“Helping people die: is it murder or mercy?”
“Would you personally use your right for euthanasia if there was no chance to get better?”
Variations are welcomed.
Euthanasia essay introduction: general recommendations
Most professional essay writing services agree that writing an introduction is always the hardest thing. You get the fear of the blank paper, writer’s block, and the stress from remembering all the requirements you should ideally follow.
… Sounds familiar?
There are no reasons to be that stressed, actually. The web is full of info, interesting statistics, law variations, and personal stories.
A combination of those would be both, catchy and informative, that’s all you need for a perfect intro.
Start with some background information to help your reader understand the subject better.
What kind of info would be relevant?
- A brief definition of Euthanasia.
- When it might be allowed.
- Laws of the countries where it is permitted.
- Personal stories of friends/relatives.
- Stories of doctors and nurses.
All of that can be easily found online. Your goal here would rewrite it in your style, make it appealing to read and combined logically. End your introduction with the thesis statement. You already know how it’s done.
Specifics of Euthanasia essay main body
The main body for an argumentative essay should consist of two parts, one for each point of view. Once you express your point of view in the introduction, then it would be logical to start the main body from it.
Still, it is far from being obligatory. You may start with whatever you find more comfortable.
Like, f.e., you decide to start by talking about the positive aspects of Euthanasia. List the statements using words “firstly,” “secondly,” “moreover,” etc. Begin with the weakest argument and move up to the most solid one you have.
Provide the reader with some positive examples, including personal stories, if they fit in, try to find shreds of evidence of euthanasia practice in your country.
Here are some ideas for statements in favor of Euthanasia:
- A patient’s life can be worse than death.
- It is better to die from Euthanasia than from suicide.
- Euthanasia can help in saving budget funds. Saved money may help somebody else.
- Some people don’t want to see how their relatives suffer hopelessly.
- Death from Euthanasia can be more humane than natural.
Once you finish with the arguments for the first part, go on representing the opposite point of view. A good idea to begin the second paragraph with phrases like “on the other hand,” “the other side of the coin is,” “however,” etc.
List a couple of statements against Euthanasia. You may also search for some scandals including the illegal activity of doctors who made such decision without consulting the patient’s relatives.
Here are several ideas that might be helpful.
- Life is the primary integral right and can’t be taken away.
- If there are many organizations and measures to prevent suicides, why should we offer death to someone?
- Each aspect of Euthanasia can’t be foreseen in the law.
- It’s impossible to define who may/may not be offered the Euthanasia.
- What if the person who chose Euthanasia could recover and live the life to its fullest?
What to write in Euthanasia essay conclusion?
In conclusion, you sum up all the ideas highlighted in your essay, without adding new ones. Start with phrases like “to sum up,” “to conclude,” “in conclusion,” “on balance,” “in a nutshell,” etc.
Here you should also express your point of view and paraphrase the thesis you used in the introduction. For uttering your point, use inputs like “my point of view is,” “I strongly believe,” “I am convinced,” “to tell you the truth,” and so on.
How to create a Euthanasia essay outline?
An outline is a brief sketch of your essay. If you need to write it, select the main ideas of your work and write them down in a couple of sentences.
The sketch outline for an essay on Euthanasia may be like:
“Th work is about the problem of Euthanasia. I highlight some statements for and against the use of Euthanasia and support them with top examples. In conclusion, I explain my personal position on this question.”
The full version of an outline would look something like this…
Introduction
- Hook sentence
- Thesis statement
- Transition to Main Body
- History of Euthanasia
- Euthanasia statistics in countries where it is legal
- Impact of legal Euthanasia on people’s life
- Negative consequences of illegal Euthanasia
- Transition to Conclusion
- Unexpected twist or a final argument
- Food for thought
The use of Euthanasia argumentative essay example
This topic is pretty vast. It can be both good and bad for you. Due to the variety of topics within the issue of Euthanasia, it might be easy to find something you are genuinely interested in.
On the other hand, there are dozens of various materials, thousands of articles, and billions of opinions you should consider before writing. Sometimes it might be difficult for you to get a full picture.
Therefore, a sample of the essay on this topic is presented here. It follows all the standards of an argumentative essay and shows you how this type of work may be completed.
On balance…
I’d say that it’s great to work with such an ambiguous topic. You’ll definitely benefit from training your persuasive and analytical skills while working on this essay.
Hope you’ve found some inspiration here, good luck!
Not excited to write an essay on euthanasia? Buy argumentative essay instead! Luckily, we’ve got dozens of writers, who are 100% fit for the job. Order an essay and save time for yourself!

Preparing to Write a Depression Research Paper

What Is Spatial Order And How To Use It In Essay?

Custom drinking and driving
Advertisement
Supported by
A Culture Warrior Takes a Late Swing
The editor and essayist Joseph Epstein looks back on his life and career in two new books.
- Share full article

By Dwight Garner
NEVER SAY YOU’VE HAD A LUCKY LIFE: Especially If You’ve Had a Lucky Life , by Joseph Epstein
FAMILIARITY BREEDS CONTENT: New and Selected Essays , by Joseph Epstein
When Tammy Wynette was asked to write a memoir in her mid-30s, she initially declined, she said in an interview, because “I didn’t think my life was over yet.” The publisher responded: Has it occurred to you that in 15 years no one might care? She wrote the book. “Stand by Your Man: An Autobiography” (1979) was a hit.
The essayist and editor Joseph Epstein — whose memoir “Never Say You’ve Had a Lucky Life,” is out now, alongside a greatest-hits collection titled “Familiarity Breeds Content” — has probably never heard Wynette sing except by accident. (In a 1993 essay, he wrote that he wished he didn’t know who Willie Nelson was, because it was a sign of a compromised intellect.) But his memoir illustrates another reason not to wait too long to commit your life to print.
There is no indication that Epstein, who is in his late 80s, has lost a step. His prose is as genial and bland, if comparison to his earlier work is any indication, as it ever was. But there’s a softness to his memories of people, perhaps because it was all so long ago. This is the sort of memoir that insists someone was funny, or erudite, or charismatic, while rarely providing the crucial details.
Epstein aw-shucks his way into “Never Say You’ve Had a Lucky Life” — pretending to be self-effacing while not being so in the least is one of his salient qualities as a writer — by warning readers, “I may not have had a sufficiently interesting life to merit an autobiography.” This is because he “did little, saw nothing notably historic, and endured not much out of the ordinary of anguish or trouble or exaltation.” Quickly, however, he concludes that his life is indeed worth relating, in part because “over the years I have acquired the literary skill to recount that life well.”
Here he is wrong in both directions. His story is interesting enough to warrant this memoir. His personal life has taken complicated turns. And as the longtime editor of the quarterly magazine The American Scholar, and a notably literate conservative culture warrior, he’s been in the thick of things.
He does lack the skill to tell his own story, though, if by “skill” we mean not well-scrubbed Strunk and White sentences but close and penetrating observation. Epstein favors tasseled loafers and bow ties, and most of his sentences read as if they were written by a sentient tasseled loafer and edited by a sentient bow tie.
He grew up in Chicago, where his father manufactured costume jewelry. The young Epstein was popular and, in high school, lettered in tennis. His title refers to being lucky, and a big part of that luck, in his estimation, was to grow up back when kids could be kids, before “the therapeutic culture” took over.
This complaint sets the tone of the book. His own story is set next to a rolling series of cultural grievances. He’s against casual dress, the prohibition of the word “Negro,” grade inflation, the Beat Generation, most of what occurred during the 1960s, standards slipping everywhere, de-Westernizing college curriculums, D.E.I. programs, you name it. His politics aren’t the problem. We can argue about those. American culture needs more well-read conservatives. The problem is that in his search for teachable moments, his memoir acquires the cardboard tone of a middling opinion column.
His youth was not all tennis lessons and root beer floats. He and his friends regularly visited brothels because, he writes, sex was not as easy to come by in the 1950s. He was kicked out of the University of Illinois Urbana-Champaign for his role in the selling of a stolen accounting exam to other students.
He was lucky to find a place at the University of Chicago, a place of high seriousness. The school changed him. He began to reassess his values. He began to read writers like Irving Howe, Sidney Hook, Midge Decter and Norman Podhoretz, and felt his politics pull to the right.
After college, he was drafted into the Army and ended up in Little Rock, Ark., where he met his first wife. At the time, she was a waitress at a bar and restaurant called the Gar Hole. Here Epstein’s memoir briefly threatens to acquire genuine weight.
She had lost custody of her two sons after a divorce. Together they got them back, and she and Epstein had two sons of their own. After their divorce, Epstein took all four of the boys. This is grist for an entire memoir, but Epstein passes over it quickly. One never gets much of a sense of what his boys were like, or what it was like to raise them. He later tells us that he has all but lost touch with his stepsons and has not seen them for decades.
He worked for the magazine The New Leader and the Encyclopaedia Britannica before becoming the editor of The American Scholar in 1975. It was a position he would hold for 22 years. He also taught at Northwestern University for nearly three decades.
At The American Scholar he began to write a long personal essay in each issue, under the pseudonym Aristides. He wrote 92 of these, on topics such as smoking and envy and reading and height. Most ran to 6,500 words, or about 4,000 words longer than they should have been.
Many magazine editors like to write every so often, to keep a hand in. But there is something unseemly about an editor chewing up acres of space in his own publication on a regular basis. Editorially, it’s a droit du seigneur imposition.
A selection of these essays, as well as some new ones, can now be found in “Familiarity Breeds Content.” In his introduction to this book, Christopher Buckley overpraises Epstein, leaving the reader no choice but to start mentally pushing back.
Buckley calls Epstein “the most entertaining living essayist in the English language.” (Not while Michael Kinsley, Lorrie Moore, Calvin Trillin, Sloane Crosley and Geoff Dyer, among many others, walk the earth.) He repurposes Martin Amis’s comment about Saul Bellow: “One doesn’t read Saul Bellow. One can only reread him.” To this he adds, “Ditto Epstein.” (Epstein is no Saul Bellow.) Buckley says, “Joe Epstein is incapable of writing a boring sentence.”
Well. How about this one, from an essay about cats?
A cat, I realize, cannot be everyone’s cup of fur.
Or this one, from an essay about sports and other obsessions:
I have been told there are people who wig out on pasta.
Or this one, about … guess:
When I was a boy, it occurs to me now, I always had one or another kind of hat.
Juggling today appears to be undergoing a small renaissance.
If one is looking to save on fuel bills, politics is likely to heat up a room quicker than just about anything else.
In tennis I was most notable for flipping and catching my racket in various snappy routines.
The essays are, by and large, as tweedy and self-satisfied as these lines make them sound. There are no wild hairs in them, no sudden deepenings of tone. Nothing is at stake. We are stranded with him on the putt-putt course.
Epstein fills his essays with quotation after quotation, as ballast. I am a fan of well-deployed, free-range quotations. So many of Epstein’s are musty and reek of Bartlett’s. They are from figures like Lord Chesterfield and Lady Mary Montagu and Sir Herbert Grierson and Tocqueville and Walpole and Carlyle. You can feel the moths escaping from the display case in real time.
To be fair, I circled a few sentences in “Familiarity Breeds Content” happily. I’m with him on his distrust of “fun couples.” He writes, “A cowboy without a hat is suitable only for bartending.” I liked his observation, which he borrowed from someone else, that a career has five stages:
(1) Who is Joseph Epstein? (2) Get me Joseph Epstein. (3) We need someone like Joseph Epstein. (4) What we need is a young Joseph Epstein. (5) Who is Joseph Epstein?
It’s no fun to trip up a writer on what might have been a late-career victory lap. Epstein doesn’t need me to like his work. He’s published more than 30 books, and you can’t do that unless you’ve made a lot of readers happy.
NEVER SAY YOU’VE HAD A LUCKY LIFE : Especially If You’ve Had a Lucky Life | By Joseph Epstein | Free Press | 287 pp. | $29.99
FAMILIARITY BREEDS CONTENT : New and Selected Essays | By Joseph Epstein | Simon & Schuster | 441 pp. | Paperback, $20.99
Dwight Garner has been a book critic for The Times since 2008, and before that was an editor at the Book Review for a decade. More about Dwight Garner
Explore More in Books
Want to know about the best books to read and the latest news start here..
Salman Rushdie’s new memoir, “Knife,” addresses the attack that maimed him in 2022, and pays tribute to his wife who saw him through .
Recent books by Allen Bratton, Daniel Lefferts and Garrard Conley depict gay Christian characters not usually seen in queer literature.
What can fiction tell us about the apocalypse? The writer Ayana Mathis finds unexpected hope in novels of crisis by Ling Ma, Jenny Offill and Jesmyn Ward .
At 28, the poet Tayi Tibble has been hailed as the funny, fresh and immensely skilled voice of a generation in Māori writing .
Amid a surge in book bans, the most challenged books in the United States in 2023 continued to focus on the experiences of L.G.B.T.Q. people or explore themes of race.
Each week, top authors and critics join the Book Review’s podcast to talk about the latest news in the literary world. Listen here .
Link between plastic and heart attacks shows it's time to reduce packaging and its chemicals

Cranes lift waste, mostly plastic and paper at a recycling plant. Credit: AP/Oded Balilty
This guest essay reflects the views of former EPA regional administrator Judith Enck, president of Beyond Plastics and a professor at Bennington College.
Plastic has now been linked to increased risk of heart attack, stroke, and premature death in humans. At what point will policymakers realize this material — which lingers for centuries and is made with chemicals known to be toxic to humans — is as much a threat to human health as it is to the planet?
Plastic pollution entered our daily lives in the 1950s as single-use plastic like grocery bags, bottles, utensils, and food packaging began sullying our streets, parks, streams, beaches, and eventually the ocean. Recently, it’s become much more than just an environmental issue. Plastic has infiltrated our food, water, air, soil, and yes, even our bodies. It’s been found in human blood, lungs, breast milk, placentas, and more.
A March study in the New England Journal of Medicine found tiny plastic particles in human arteries — specifically the carotid arteries, which supply blood to the brain. That’s not the worst of it: Patients with plastic-tainted arteries were nearly five times more likely to suffer from a cardiovascular event like heart attack or stroke.
Still, the chemical additives in plastic are arguably more concerning. They have been associated with cancer, nervous system damage, hormone disruption, and fertility issues, just to name a few.
Over 16,000 chemicals are used in plastic to give it color, pliability, durability, fire resistance, and more. Of those, at least 4,200 are considered “highly hazardous” to human health and the environment. Thousands more haven’t even been tested for toxicity. Because these additives aren’t tightly bound to plastic, they can leach into our food and beverages from their plastic packages, especially when heated.
From our Editorial Board, get inside the local, city and state political scenes.
By clicking Sign up, you agree to our privacy policy .
We don’t need another 50 years of research to confirm that ingesting a nonbiodegradable, inorganic material made with toxic chemicals is a risk to human health. Our plastic exposure will only expand in the future — plastic production is expected to triple by 2060.
Inaction is no longer an option. Fortunately, New York state lawmakers are considering a transformational piece of public policy. If adopted, the Packaging Reduction and Recycling Infrastructure Act would be the most sweeping packaging reduction law in the world, cutting plastic packaging in half over the next 12 years. After reduction, the remaining packaging must be reusable or recyclable.
This part alone is monumental, but the bill also requires some of the most toxic chemicals used in packaging to be eliminated. It would prohibit the use of PFAS (known as “forever chemicals”), lead, mercury, bisphenols, formaldehyde, vinyl chloride, and other chemicals in packaging — chemicals you probably didn’t know were in the plastic covering your food and drinks.
The legislation also would make a sizable dent in the nation’s plastic production and use, given New York’s ranking as the fourth-largest state in the country. If enacted, this bill would set a blueprint for other states to adopt.
New York legislators should remember this is an election year, and voters want to see effective policies to reduce plastic pollution. A 2022 poll found that 88% of people registered to vote in New York are concerned about single-use plastic products and support local and state policies to reduce single-use plastic.
We need Assembly Speaker Carl Heastie and State Senate Majority Leader Andrea Stewart-Cousins to bring the Packaging Reduction and Recycling Infrastructure Act to the floor for a vote. Our health, and the planet’s health, are at stake. We have no more time to waste on waste.
THIS GUEST ESSAY reflects the views of former EPA regional administrator Judith Enck, president of Beyond Plastics and a professor at Bennington College.
Euthanasia: Advantages and Disadvantages Essay
Introduction, euthanasia- pros and cons, works cited.
Euthanasia, or as it’s known in English as ‘mercy killing’, is a Greek term for ‘good death’ and has been one of the most controversial and heatedly debated topics in healthcare and politics. It’s an intentionally administered death to a patient of a fatal injury or disease and is administered with the consent of the patient/victim and their relatives, although there have been cases where it has been done without consent. It’s a controversial policy topic for policymakers, politicians, lawyers, and the medical community and has been legalized in several states of the USA, whereas in many states, it remains violently protested against the notion and has been tagged as physician-assisted suicide. (Burke J. Balch, 2006). There are many aspects of euthanasia, with voluntary euthanasia being on the request of the patient and involuntary where no such request is made and no consent is asked for (or given). For patients undergoing severe medical treatments, the withdrawal of medical facilities and thus leaving them vulnerable to death is euthanasia by omission (i.e. omission of medical aids or life-saving facilities). For other patients suffering from incurable diseases, the administering of fatal, venomous injections to give them a slow (albeit painless) death is called euthanasia by action.
There have been numerous and many intense debates for and against euthanasia, with equal merit on both sides and pro – euthanasia thinkers being called merciless and those lacking faith and other Godly considerations. The most popular arguments against euthanasia include the derogation of human life and disregard for an individual’s right to live. The most heavily criticized of all such similar actions is involuntary euthanasia which bears the brunt of all severe protests against the issue, with involuntary euthanasia being dubbed as the deprivation of an individual of their basic right to live and die fully. This is the notion most historians and policymakers of all states banning it holds. They regard the whole necessity of choosing one’s death by the state laws as a request to let the government sell contaminated food to its citizens knowing it’s harmful to their health. The slippery slope phenomenon is also a famous theory against the question of legalizing euthanasia, ascertaining that the practice might be extended to people who are terminally ill to people who could be saved otherwise but eat up a lot of resources which makes it open to economic considerations as opposed to ethical/human ones. Another stand very popular among the medical community is that the crucial healthcare rule is the will to health and quality life and the abstinence of willing anything which may prove detrimental to an individual (Robinson, 2007).
The pros on the other hand provide quite interesting perspectives on the issue. Proponents can give almost every counter-statement to everything the opponents have to say to vilify the practice of euthanasia. The basic of all healthcare intentions is to relieve the sufferer’s suffering. This is should entail putting an end to the pain and torture of perpetual illness by administering peaceful death. This also follows a basic question of freedom of choice, everyone should have the right to choose for themselves, their life and death, and the government should not interfere in such crucial and personal decisions (ProCon.org, 2009).
Looking at both sides introduces some personal concerns in the mind regarding whether one should be given the right to live and die or not. Both above such abstract and seemingly complex considerations is one more objective and more critical factor that needs to be taken into account while deciding the fate of euthanasia and policies regarding its legality.
Looking at the issue from a governmental and economical perspective, facilities administered to terminally ill patients are usually very expensive and exhaust the already scarce resources at hand. So even if deliberately putting an end to a patient who’s already proceeding slowly toward a painful, hopeless end might seem selfish and hurried, it’s wise to sometimes give up such considerations in regard for the ‘greater good that can come out of such decisions. It’s rather important to free up r4esouces for people who have hope of recovery and need them to lead better lives as opposed to people who’re immune to all cures and expensive treatments and end up becoming a burden to society.
- Burke J. Balch, J. (2006). Why We Shouldn’t Legalize Assisting Suicide.
- ProCon.org. (2009). Founding Fathers on Religion in Government.
- Robinson, B. (2007). euthanasia and physician assisted suicide.
- Chicago (A-D)
- Chicago (N-B)
IvyPanda. (2023, October 30). Euthanasia: Advantages and Disadvantages. https://ivypanda.com/essays/euthanasia-advantages-and-disadvantages/
"Euthanasia: Advantages and Disadvantages." IvyPanda , 30 Oct. 2023, ivypanda.com/essays/euthanasia-advantages-and-disadvantages/.
IvyPanda . (2023) 'Euthanasia: Advantages and Disadvantages'. 30 October.
IvyPanda . 2023. "Euthanasia: Advantages and Disadvantages." October 30, 2023. https://ivypanda.com/essays/euthanasia-advantages-and-disadvantages/.
1. IvyPanda . "Euthanasia: Advantages and Disadvantages." October 30, 2023. https://ivypanda.com/essays/euthanasia-advantages-and-disadvantages/.
Bibliography
IvyPanda . "Euthanasia: Advantages and Disadvantages." October 30, 2023. https://ivypanda.com/essays/euthanasia-advantages-and-disadvantages/.
- Singer’s Views on Voluntary Euthanasia, Non-voluntary Euthanasia, and Involuntary Euthanasia
- Why Active Euthanasia is Morally Wrong
- When Ethics and Euthanasia Conflict?
- Euthanasia: Right to Live or Right to Die
- Euthanasia in Today’s Society
- Euthanasia: A Legalized Right to Die
- Euthanasia: Is It the Best Solution?
- Euthanasia: Is It Worth the Fuss?
- Euthanasia Legalization: Public Policy Debates
- Euthanasia for Terminally Ill People: Pros & Cons
- Euthanasia: Every For and Against
- Ethical Theories: Utilitarian Theory of Ethics
- Ethical Issues in Terri Schiavo Case
- Medical Malpractice: What are the Grounds?
- Ethical Issues in Health Care
Opinion: Earth Day essays praised for being inspirational and insightful

A high school sophomore and a veteran local activist offered powerful messages of what we can achieve if we work together
- Show more sharing options
- Copy Link URL Copied!
Re “We can all do more to preserve the environment” ( April 19 ): Thank you to Faith Barton for a thoughtful and thought-provoking opinion piece. It is encouraging to read the words of a high school sophomore that ring so true today.
Back in the early 1970s, there was a public service announcement that featured a Native American shedding a tear at the amount of litter in his environment. Now, more than 50 years later, we are still dealing with the same problem, and in some places it is considerably worse. Until all of us take personal responsibility in caring for the planet upon which we all live, I fear that we will still be talking about this problem 50 years from now.
Faith has given us a path to travel in making this planet, our planet, a cleaner place to live. Let’s all get behind her.
— John Silcox, Serra Mesa
Re “Does local energy and local control translate into lower rates?” ( April 19 ): Carolyn Chase’s op-ed is wonderful! We must return to Earth Day’s roots if we are to survive and flourish in the climate change crisis.
Let’s listen to a longtime, deeply experienced leader who has the wisdom to recognize we have all the energy we need right here in San Diego and the technology to make it work. If they were used locally, rooftop solar and parking lot solar would cut down on expensive transmission lines. Local employees and administrators would care about their own community as opposed to Sempra’s stockholders, who do not live here.
The current system doesn’t work for San Diego. Let’s put in something that will work!
— Joan L. Raphael, Mira Mesa
Get Essential San Diego, weekday mornings
Get top headlines from the Union-Tribune in your inbox weekday mornings, including top news, local, sports, business, entertainment and opinion.
You may occasionally receive promotional content from the San Diego Union-Tribune.

More from this Author

Readers React
Opinion: Guns are the leading cause of death among children in the U.S. Where’s the outrage?
April 24, 2024

Opinion: Cutting library funding will haunt the city of San Diego by hurting children
April 23, 2024

Opinion: Abuse victim’s powerful message must resonate with San Diego community

Opinion: Fixed electricity fee is not ‘progressive’ — it’s a gift to the state’s utilities
April 22, 2024

Opinion: ‘Empty warehouse’ eyed for huge homeless shelter actually a classic Modernist building

Opinion: SANDAG dupes public, then asks taxpayers to pay more even more? Unbelievable.
April 19, 2024
More in this section

Google should follow precedent set by cable TV and pay for content
Local TV stations carried on cable systems drew more viewers than ESPN or CNN. Congress allowed them to seek payment from cable companies.
April 25, 2024

Opinion: Does mayor’s math add up on costly homeless initiative?
Re “San Diego’s dubious real estate track record slows down mayor’s proposed new 1,000-bed shelter” (April 14): Mayor Todd Gloria’s latest initiative to provide 1,000 beds in a potential homeless shelter Downtown is cause for great concern.

Opinion: ‘Triage’ approach and common sense needed to make progress on homelessness
Addressing symptoms of a problem won’t make the problem go away

Opinion: CEO of museum challenges claims about its legal obligations
Officials are honoring their 2004 agreement with the city of San Diego on the use of the site
April 18, 2024

Opinion: Senior pleads for help after home insurance bill nearly triples
Are homeowners paying more to bail out insurers struggling with wildfire costs?
April 17, 2024

Opinion: Will city’s Styrofoam ban only be heeded in certain neighborhoods? Maybe
Relying on public complaints to enforce the law could lead to disparities
Faculty of Arts
Active learning through video essays: challenges, opportunities and ways forward.
25 April 2024, 5.00 PM
Dr. Estrella Sendra (KCL)
Richmond Building, 5.65 Lecture Room (5th Floor, Students' Union, Queens Road)

- Election 2024
- Entertainment
- Newsletters
- Photography
- Personal Finance
- AP Investigations
- AP Buyline Personal Finance
- AP Buyline Shopping
- Press Releases
- Israel-Hamas War
- Russia-Ukraine War
- Global elections
- Asia Pacific
- Latin America
- Middle East
- Election Results
- Delegate Tracker
- AP & Elections
- Auto Racing
- 2024 Paris Olympic Games
- Movie reviews
- Book reviews
- Personal finance
- Financial Markets
- Business Highlights
- Financial wellness
- Artificial Intelligence
- Social Media
Panama Papers trial’s public portion comes to an unexpectedly speedy end
The Supreme Court stands in Panama City, Monday, April 8, 2024 as the trial starts for those charged in connection with the worldwide “Panama Papers” money laundering case. (AP Photo/Agustin Herrera)
Juergen Mossack, partner of the law firm Mossack-Fonseca, leaves the Supreme Court during the trial of the “Panama Papers” money laundering case in Panama City, Monday, April 8, 2024. (AP Photo/Agustin Herrera)
Lawyers and court workers leave the Supreme Court during a recess for the trial of the “Panama Papers” money laundering case in Panama City, Monday, April 8, 2024. (AP Photo/Agustin Herrera)
- Copy Link copied
PANAMA CITY (AP) — The public portion of a trial of more than two-dozen associates accused of helping some of the world’s richest people hide their wealth came to an unexpectedly speedy conclusion Friday when a Panamanian judge said she would take the two weeks of trial arguments and testimony under advisement.
The trial came eight years after 11 million leaked secret financial documents that became known as the “Panama Papers” prompted the resignation of the prime minister of Iceland and brought scrutiny to the then-leaders of Argentina and Ukraine, Chinese politicians, and Russian President Vladimir Putin, among others.
Judge Baloisa Marquínez noted Friday that the case included more than 530 volumes of information. The public trial had been expected to run to the end of the month. The judge has 30 working days to issue a verdict.
Those on trial include the owners of the Mossack Fonseca law firm that was at the heart of the 2016 massive document leak. Jürgen Mossack attended the trial, while his partner Ramón Fonseca did not for health reasons, according to his counsel.
Panamanian prosecutors allege that Mossack, Fonseca and their associates created a web of shell companies that used complex transactions to hide money linked to illicit activities in the “car wash” corruption scandal of Brazilian construction giant Odebrecht .
“This whole process from eight years ago until now … has had a lot of consequences for my family, on my personal situation and truly has been a great injustice not just for me but for all of the people who have worked with me,” Mossack testified Friday. “I trust your honor will know how to evaluate all that has been said here.”
Mossack had said at the start of the trial, as he has for years, that he was not guilty of the money laundering charges.
According to Panamanian prosecutors, the Mossack Fonseca firm created 44 shell companies, 31 of which opened accounts in Panama to hide money linked to the Brazilian scandal.
Fonseca has said the firm, which closed in 2018, had no control over how its clients might use offshore vehicles created for them.
Mossack Fonseca helped create and sell around 240,000 shell companies across four decades in business. It announced its closure in March 2018, two years after the scandal erupted.
The firm’s documents were first leaked to the German daily Suddeutsche Zeitung, and were shared with the International Consortium of Investigative Journalists, which began publishing collaborative reports with news organizations in 2016.
“The reputational deterioration, the media campaign, the financial siege and the irregular actions of some Panamanian authorities have caused irreparable damage, whose consequence is the complete cease of operations to the public,” the firm said in a statement at the time.
The Mossack and Fonseca were acquitted on other charges in 2022.
COMMENTS
The analyses, conclusions, and recommendations presented here are offered with optimism that we can, individually and together, "approach" death constructively and create humane care systems that people can trust to serve them well as they die. Page 259 Share Cite.
Conclusion Writing an essay on euthanasia is a complex and intricate process that requires a thorough understanding of the topic and careful consideration of its ethical and moral implications. However, with the help of GradesFixer essay examples, this process can be made much easier. The GradesFixer provides well-written and thoroughly ...
Conclusion. In the end, after examining both sides of the problem, Euthanasia should be seen as an option for dying patients because they should have the right to choose, end their suffering of living, and it will save them money on medical costs.
Conclusion . In conclusion, euthanasia is a complex issue with both advantages and disadvantages. While euthanasia can relieve pain and suffering, promote personal autonomy and individual freedom, and reduce healthcare costs, it also carries several risks and ethical implications, including the potential devaluation of human life and the risk ...
As a medical doctor I have, with some worry, followed the assisted dying debate that regularly hits headlines in many parts of the world. The main arguments for legalisation are respecting self-determination and alleviating suffering. Since those arguments appear self-evident, my book Euthanasia and the Ethics of a Doctor's Decisions—An Argument Against Assisted Dying 1 aimed to contribute ...
3. Evolution of euthanasia and assisted suicide: digging into historical events. To understand the evolution and relevance of these concepts should analyze the history of euthanasia and assisted suicide; from the emergence of the term, going through its first manifestations in antiquity; mentioning the conceptions of great thinkers such as Plato and Hippocrates; going through the role of the ...
The Netherlands was the first country to allow legal euthanasia and assisted suicide in 2002, totaling 1.7-2.8% of total deaths. Euthanasia is generally illegal in the United States, but in a nationwide 2017 American poll, 73% of the public were in favor of euthanasia, and 57% said euthanasia is morally acceptable. These numbers are nearly ...
Besides, it should also tell you the type of essay you are required to write and the scope. 2. Choose a Captivating Topic. After reading the prompt, you are required to frame your euthanasia essay title. Make sure that the title you choose is captivating enough as it invites the audience to read your essay.
It has been a pertinent issue in human rights discourse as it also affects ethical and legal issues pertaining to patients and health care providers. This paper discusses the legal and ethical ...
Crafting an essay on the conclusion of euthanasia is indeed a challenging task. The intricacy. associated with the topic. The conclusion demands a balance between providing closure to. the reader and leaving room for contemplation on the complex nature of euthanasia. the ethical principles involved, and the potential implications of the arguments.
This is referred to as euthanasia. It is the act of deliberately terminating life when it is deemed to be the only way that a person can get out of their suffering (Johnstone 247). Euthanasia is commonly performed on patients who are experiencing severe pain due to terminal illness. For one suffering from terminal illness, assisted death seems ...
📑 Aspects to Cover in an Euthanasia Essay. Euthanasia is the process of intentional life ending. Its goal is to stop patients' suffering and pain. In today's world, euthanasia is a debatable topic, and there are many questions about it. Euthanasia essays can help students to raise awareness of the process and its aspects.
Euthanasia is Greek word that when directly translated refers to the "good death"; more specifically euthanasia is a term that is used to describe death conditions that has been undertaken deliberately for purposes of alleviating suffering of an individual usually from a terminal illness for which no recovery is expected. Hence, for ...
This essay explores the ethical and legal implications surrounding the controversial topic of euthanasia, specifically focusing on a recent case study of a woman who underwent euthanasia due to mental illness. ... Conclusion. The topic of euthanasia is controversial based on the numerous arguments aired by those in its support and those who are ...
Euthanasia comes from the Greek words "Eu", meaning well or easy, and "Thanatos", meaning death. In modern terms it is the intentional premature termination of another's life by direct intervention or by withholding care. [1] Within that it can be either voluntary (expressed or implied consent), or involuntary.
Euthanasia: Dying with Dignity Essay. Euthanasia: Dying with Dignity Someday, a loved one may be faced with tough times or a terrible tragedy that leaves them in pain and agony for the rest of their life. It may not happen today, tomorrow, or even next month, but it is always a good idea to have a well thought out plan.
48 essay samples found. Euthanasia, also known as assisted dying or mercy killing, remains a deeply contested ethical and legal issue. Essays could delve into the various forms of euthanasia, such as voluntary, non-voluntary, and involuntary euthanasia, discussing the moral and legal implications of each.
Essay on Euthanasia: Euthanasia refers to the act of killing a person without any emotions or mercy. Euthanasia is an ethnically complex and controversial topic, with different perspectives and legal regulations on different topics. School students and individuals preparing for competitive exams are given assigned topics like essays on euthanasia.
Conclusion. Euthanasia remains a complex and contentious issue, with arguments both for and against it deeply rooted in ethical principles and deeply held beliefs. Advocates for euthanasia stress the importance of autonomy and self-determination, the relief of suffering, and the protection of personal choice as compelling reasons to support the ...
What to write in Euthanasia essay conclusion? In conclusion, you sum up all the ideas highlighted in your essay, without adding new ones. Start with phrases like "to sum up," "to conclude," "in conclusion," "on balance," "in a nutshell," etc. Here you should also express your point of view and paraphrase the thesis you used ...
General Arguments Against Euthanasia: 1-One should not interfere in the doings of God: As God has a purpose to everything. Counter point: A person in favor of it usually says how one can be sure of what god wants or what god has in His mind. God has given us intellect to make one's life as better as possible.
She was allowed to refer only to a single 3-by-5 index card, which she had packed with information based on a "summary sheet" of takeaways that she and her teammates worked up together, with ...
FAMILIARITY BREEDS CONTENT: New and Selected Essays, by Joseph Epstein. When Tammy Wynette was asked to write a memoir in her mid-30s, she initially declined, she said in an interview, because ...
Since my essay last year, MacArthur and a coalition of funders launched Press Forward, a national movement to strengthen communities by reinvigorating local news.Press Forward will invest more than $500 million over five years to re-center local news as a force for community cohesion; support new models and solutions that are ready to scale; and close longstanding inequities in journalism ...
Opinion Commentary Guest Essays Link between plastic and heart attacks shows it's time to reduce packaging and its chemicals. ... By Judith EnckGuest essay Updated April 24, 2024 5:20 pm.
In conclusion, the moral and ethical arguments in favor of euthanasia revolve around the principles of relieving suffering, respecting individual autonomy, and promoting compassion and empathy. Euthanasia provides a means for individuals to end their lives with dignity when suffering becomes unbearable, preserving their autonomy and their right ...
Euthanasia- Pros and Cons. There have been numerous and many intense debates for and against euthanasia, with equal merit on both sides and pro-euthanasia thinkers being called merciless and those lacking faith and other Godly considerations.The most popular arguments against euthanasia include the derogation of human life and disregard for an individual's right to live.
Re "We can all do more to preserve the environment" (April 19): Thank you to Faith Barton for a thoughtful and thought-provoking opinion piece. It is encouraging to read the words of a high ...
Active Learning Through Video Essays: Challenges, Opportunities and Ways Forward. 25 April 2024, 5.00 PM - 23 April 2024, 6.00 PM. Dr. Estrella Sendra (KCL) Richmond Building, 5.65 Lecture Room (5th Floor, Students' Union, Queens Road)
PANAMA CITY (AP) — The public portion of a trial of more than two-dozen associates accused of helping some of the world's richest people hide their wealth came to an unexpectedly speedy conclusion Friday when a Panamanian judge said she would take the two weeks of trial arguments and testimony under advisement.. The trial came eight years after 11 million leaked secret financial documents ...