Research Design Review
A discussion of qualitative & quantitative research design, the use of quotes & bringing transparency to qualitative analysis.
“An overemphasis on the researcher’s interpretations at the cost of participant quotes will leave the reader in doubt as to just where the interpretations came from [however] an excess of quotes will cause the reader to become lost in the morass of stories.” (Morrow, 2005, p. 256)
By embedding carefully chosen extracts from participants’ words in the final document, the researcher uniquely gives participants a voice in the outcomes while contributing to the credibility – and transparency – of the research. In essence, the use of verbatims gives the users of the research a peek into the analyst’s codebook by illustrating how codes associated with particular categories or themes in the data were defined during the analysis process.
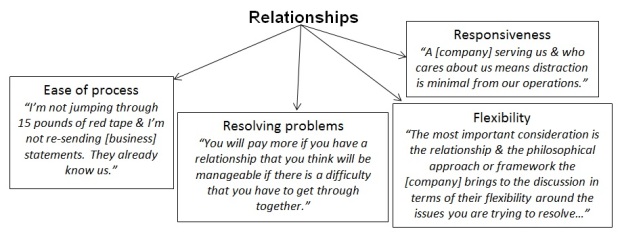
As an example, the analysis of data from a recent in-depth interview study among business decision makers determined that the broad concept of “relationships” was a critical factor to driving certain types of decisions. That alone is not a useful finding; however, the analysis of data within this category uncovered themes that effectively gave definition to the “relationships” concept. As shown below, the definitional themes, in conjunction with illustrative quotes from participants, give the reader a concise and useful understanding of “relationships.”
In this way, quotes contribute much-needed transparency to the analytical process. As discussed elsewhere in Research Design Review (e.g., see this April 2017 article ), transparency in the final document is built around “thick description,” defined as “a complete account…of the phenomena under investigation as well as the rich details of the data collection and analysis processes and interpretations of the findings” (Roller & Lavrakas, 2015, p. 363). One of the ingredients in a thick description of the analytical process is the details of code development and the coding procedures. The utilization of verbatims from participants in the final report adds to the researcher’s thick description (and transparency) by helping to convey the researcher’s thinking during data analysis and how that thinking steered the creation and application of codes.
Morrow, S. L. (2005). Quality and trustworthiness in qualitative research in counseling psychology. Journal of Counseling Psychology , 52 (2), 250–260. http://doi.org/10.1037/0022-0167.52.2.250
Roller, M. R., & Lavrakas, P. J. (2015). Applied qualitative research design: A total quality framework approach . New York: Guilford Press.
Image captured from: https://cdmginc.com/testing-corner-quotation-marks-add-power/

Share this:
- Click to share on Reddit (Opens in new window)
- Click to share on Twitter (Opens in new window)
- Click to share on LinkedIn (Opens in new window)
- Click to share on Facebook (Opens in new window)
- Click to share on Tumblr (Opens in new window)
- Click to email a link to a friend (Opens in new window)
- Click to print (Opens in new window)
- Pingback: Qualitative Data Analysis: 16 Articles on Process & Method | Research Design Review
A good reference, as well as making a good point about the integration and grounding of the participant’s voice with the researcher’s/ evaluator’s interpretations and recommendations. This exemplfies the strentgh of a qualitative approach!
Leave a comment Cancel reply
This site uses Akismet to reduce spam. Learn how your comment data is processed .

- Already have a WordPress.com account? Log in now.
- Subscribe Subscribed
- Copy shortlink
- Report this content
- View post in Reader
- Manage subscriptions
- Collapse this bar

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Can J Hosp Pharm
- v.67(6); Nov-Dec 2014
Qualitative Research: Getting Started
Introduction.
As scientifically trained clinicians, pharmacists may be more familiar and comfortable with the concept of quantitative rather than qualitative research. Quantitative research can be defined as “the means for testing objective theories by examining the relationship among variables which in turn can be measured so that numbered data can be analyzed using statistical procedures”. 1 Pharmacists may have used such methods to carry out audits or surveys within their own practice settings; if so, they may have had a sense of “something missing” from their data. What is missing from quantitative research methods is the voice of the participant. In a quantitative study, large amounts of data can be collected about the number of people who hold certain attitudes toward their health and health care, but what qualitative study tells us is why people have thoughts and feelings that might affect the way they respond to that care and how it is given (in this way, qualitative and quantitative data are frequently complementary). Possibly the most important point about qualitative research is that its practitioners do not seek to generalize their findings to a wider population. Rather, they attempt to find examples of behaviour, to clarify the thoughts and feelings of study participants, and to interpret participants’ experiences of the phenomena of interest, in order to find explanations for human behaviour in a given context.
WHAT IS QUALITATIVE RESEARCH?
Much of the work of clinicians (including pharmacists) takes place within a social, clinical, or interpersonal context where statistical procedures and numeric data may be insufficient to capture how patients and health care professionals feel about patients’ care. Qualitative research involves asking participants about their experiences of things that happen in their lives. It enables researchers to obtain insights into what it feels like to be another person and to understand the world as another experiences it.
Qualitative research was historically employed in fields such as sociology, history, and anthropology. 2 Miles and Huberman 2 said that qualitative data “are a source of well-grounded, rich descriptions and explanations of processes in identifiable local contexts. With qualitative data one can preserve chronological flow, see precisely which events lead to which consequences, and derive fruitful explanations.” Qualitative methods are concerned with how human behaviour can be explained, within the framework of the social structures in which that behaviour takes place. 3 So, in the context of health care, and hospital pharmacy in particular, researchers can, for example, explore how patients feel about their care, about their medicines, or indeed about “being a patient”.
THE IMPORTANCE OF METHODOLOGY
Smith 4 has described methodology as the “explanation of the approach, methods and procedures with some justification for their selection.” It is essential that researchers have robust theories that underpin the way they conduct their research—this is called “methodology”. It is also important for researchers to have a thorough understanding of various methodologies, to ensure alignment between their own positionality (i.e., bias or stance), research questions, and objectives. Clinicians may express reservations about the value or impact of qualitative research, given their perceptions that it is inherently subjective or biased, that it does not seek to be reproducible across different contexts, and that it does not produce generalizable findings. Other clinicians may express nervousness or hesitation about using qualitative methods, claiming that their previous “scientific” training and experience have not prepared them for the ambiguity and interpretative nature of qualitative data analysis. In both cases, these clinicians are depriving themselves of opportunities to understand complex or ambiguous situations, phenomena, or processes in a different way.
Qualitative researchers generally begin their work by recognizing that the position (or world view) of the researcher exerts an enormous influence on the entire research enterprise. Whether explicitly understood and acknowledged or not, this world view shapes the way in which research questions are raised and framed, methods selected, data collected and analyzed, and results reported. 5 A broad range of different methods and methodologies are available within the qualitative tradition, and no single review paper can adequately capture the depth and nuance of these diverse options. Here, given space constraints, we highlight certain options for illustrative purposes only, emphasizing that they are only a sample of what may be available to you as a prospective qualitative researcher. We encourage you to continue your own study of this area to identify methods and methodologies suitable to your questions and needs, beyond those highlighted here.
The following are some of the methodologies commonly used in qualitative research:
- Ethnography generally involves researchers directly observing participants in their natural environments over time. A key feature of ethnography is the fact that natural settings, unadapted for the researchers’ interests, are used. In ethnography, the natural setting or environment is as important as the participants, and such methods have the advantage of explicitly acknowledging that, in the real world, environmental constraints and context influence behaviours and outcomes. 6 An example of ethnographic research in pharmacy might involve observations to determine how pharmacists integrate into family health teams. Such a study would also include collection of documents about participants’ lives from the participants themselves and field notes from the researcher. 7
- Grounded theory, first described by Glaser and Strauss in 1967, 8 is a framework for qualitative research that suggests that theory must derive from data, unlike other forms of research, which suggest that data should be used to test theory. Grounded theory may be particularly valuable when little or nothing is known or understood about a problem, situation, or context, and any attempt to start with a hypothesis or theory would be conjecture at best. 9 An example of the use of grounded theory in hospital pharmacy might be to determine potential roles for pharmacists in a new or underserviced clinical area. As with other qualitative methodologies, grounded theory provides researchers with a process that can be followed to facilitate the conduct of such research. As an example, Thurston and others 10 used constructivist grounded theory to explore the availability of arthritis care among indigenous people of Canada and were able to identify a number of influences on health care for this population.
- Phenomenology attempts to understand problems, ideas, and situations from the perspective of common understanding and experience rather than differences. 10 Phenomenology is about understanding how human beings experience their world. It gives researchers a powerful tool with which to understand subjective experience. In other words, 2 people may have the same diagnosis, with the same treatment prescribed, but the ways in which they experience that diagnosis and treatment will be different, even though they may have some experiences in common. Phenomenology helps researchers to explore those experiences, thoughts, and feelings and helps to elicit the meaning underlying how people behave. As an example, Hancock and others 11 used a phenomenological approach to explore health care professionals’ views of the diagnosis and management of heart failure since publication of an earlier study in 2003. Their findings revealed that barriers to effective treatment for heart failure had not changed in 10 years and provided a new understanding of why this was the case.
ROLE OF THE RESEARCHER
For any researcher, the starting point for research must be articulation of his or her research world view. This core feature of qualitative work is increasingly seen in quantitative research too: the explicit acknowledgement of one’s position, biases, and assumptions, so that readers can better understand the particular researcher. Reflexivity describes the processes whereby the act of engaging in research actually affects the process being studied, calling into question the notion of “detached objectivity”. Here, the researcher’s own subjectivity is as critical to the research process and output as any other variable. Applications of reflexivity may include participant-observer research, where the researcher is actually one of the participants in the process or situation being researched and must then examine it from these divergent perspectives. 12 Some researchers believe that objectivity is a myth and that attempts at impartiality will fail because human beings who happen to be researchers cannot isolate their own backgrounds and interests from the conduct of a study. 5 Rather than aspire to an unachievable goal of “objectivity”, it is better to simply be honest and transparent about one’s own subjectivities, allowing readers to draw their own conclusions about the interpretations that are presented through the research itself. For new (and experienced) qualitative researchers, an important first step is to step back and articulate your own underlying biases and assumptions. The following questions can help to begin this reflection process:
- Why am I interested in this topic? To answer this question, try to identify what is driving your enthusiasm, energy, and interest in researching this subject.
- What do I really think the answer is? Asking this question helps to identify any biases you may have through honest reflection on what you expect to find. You can then “bracket” those assumptions to enable the participants’ voices to be heard.
- What am I getting out of this? In many cases, pressures to publish or “do” research make research nothing more than an employment requirement. How does this affect your interest in the question or its outcomes, or the depth to which you are willing to go to find information?
- What do others in my professional community think of this work—and of me? As a researcher, you will not be operating in a vacuum; you will be part of a complex social and interpersonal world. These external influences will shape your views and expectations of yourself and your work. Acknowledging this influence and its potential effects on personal behaviour will facilitate greater self-scrutiny throughout the research process.
FROM FRAMEWORKS TO METHODS
Qualitative research methodology is not a single method, but instead offers a variety of different choices to researchers, according to specific parameters of topic, research question, participants, and settings. The method is the way you carry out your research within the paradigm of quantitative or qualitative research.
Qualitative research is concerned with participants’ own experiences of a life event, and the aim is to interpret what participants have said in order to explain why they have said it. Thus, methods should be chosen that enable participants to express themselves openly and without constraint. The framework selected by the researcher to conduct the research may direct the project toward specific methods. From among the numerous methods used by qualitative researchers, we outline below the three most frequently encountered.
DATA COLLECTION
Patton 12 has described an interview as “open-ended questions and probes yielding in-depth responses about people’s experiences, perceptions, opinions, feelings, and knowledge. Data consists of verbatim quotations and sufficient content/context to be interpretable”. Researchers may use a structured or unstructured interview approach. Structured interviews rely upon a predetermined list of questions framed algorithmically to guide the interviewer. This approach resists improvisation and following up on hunches, but has the advantage of facilitating consistency between participants. In contrast, unstructured or semistructured interviews may begin with some defined questions, but the interviewer has considerable latitude to adapt questions to the specific direction of responses, in an effort to allow for more intuitive and natural conversations between researchers and participants. Generally, you should continue to interview additional participants until you have saturated your field of interest, i.e., until you are not hearing anything new. The number of participants is therefore dependent on the richness of the data, though Miles and Huberman 2 suggested that more than 15 cases can make analysis complicated and “unwieldy”.
Focus Groups
Patton 12 has described the focus group as a primary means of collecting qualitative data. In essence, focus groups are unstructured interviews with multiple participants, which allow participants and a facilitator to interact freely with one another and to build on ideas and conversation. This method allows for the collection of group-generated data, which can be a challenging experience.
Observations
Patton 12 described observation as a useful tool in both quantitative and qualitative research: “[it involves] descriptions of activities, behaviours, actions, conversations, interpersonal interactions, organization or community processes or any other aspect of observable human experience”. Observation is critical in both interviews and focus groups, as nonalignment between verbal and nonverbal data frequently can be the result of sarcasm, irony, or other conversational techniques that may be confusing or open to interpretation. Observation can also be used as a stand-alone tool for exploring participants’ experiences, whether or not the researcher is a participant in the process.
Selecting the most appropriate and practical method is an important decision and must be taken carefully. Those unfamiliar with qualitative research may assume that “anyone” can interview, observe, or facilitate a focus group; however, it is important to recognize that the quality of data collected through qualitative methods is a direct reflection of the skills and competencies of the researcher. 13 The hardest thing to do during an interview is to sit back and listen to participants. They should be doing most of the talking—it is their perception of their own life-world that the researcher is trying to understand. Sophisticated interpersonal skills are required, in particular the ability to accurately interpret and respond to the nuanced behaviour of participants in various settings. More information about the collection of qualitative data may be found in the “Further Reading” section of this paper.
It is essential that data gathered during interviews, focus groups, and observation sessions are stored in a retrievable format. The most accurate way to do this is by audio-recording (with the participants’ permission). Video-recording may be a useful tool for focus groups, because the body language of group members and how they interact can be missed with audio-recording alone. Recordings should be transcribed verbatim and checked for accuracy against the audio- or video-recording, and all personally identifiable information should be removed from the transcript. You are then ready to start your analysis.
DATA ANALYSIS
Regardless of the research method used, the researcher must try to analyze or make sense of the participants’ narratives. This analysis can be done by coding sections of text, by writing down your thoughts in the margins of transcripts, or by making separate notes about the data collection. Coding is the process by which raw data (e.g., transcripts from interviews and focus groups or field notes from observations) are gradually converted into usable data through the identification of themes, concepts, or ideas that have some connection with each other. It may be that certain words or phrases are used by different participants, and these can be drawn together to allow the researcher an opportunity to focus findings in a more meaningful manner. The researcher will then give the words, phrases, or pieces of text meaningful names that exemplify what the participants are saying. This process is referred to as “theming”. Generating themes in an orderly fashion out of the chaos of transcripts or field notes can be a daunting task, particularly since it may involve many pages of raw data. Fortunately, sophisticated software programs such as NVivo (QSR International Pty Ltd) now exist to support researchers in converting data into themes; familiarization with such software supports is of considerable benefit to researchers and is strongly recommended. Manual coding is possible with small and straightforward data sets, but the management of qualitative data is a complexity unto itself, one that is best addressed through technological and software support.
There is both an art and a science to coding, and the second checking of themes from data is well advised (where feasible) to enhance the face validity of the work and to demonstrate reliability. Further reliability-enhancing mechanisms include “member checking”, where participants are given an opportunity to actually learn about and respond to the researchers’ preliminary analysis and coding of data. Careful documentation of various iterations of “coding trees” is important. These structures allow readers to understand how and why raw data were converted into a theme and what rules the researcher is using to govern inclusion or exclusion of specific data within or from a theme. Coding trees may be produced iteratively: after each interview, the researcher may immediately code and categorize data into themes to facilitate subsequent interviews and allow for probing with subsequent participants as necessary. At the end of the theming process, you will be in a position to tell the participants’ stories illustrated by quotations from your transcripts. For more information on different ways to manage qualitative data, see the “Further Reading” section at the end of this paper.
ETHICAL ISSUES
In most circumstances, qualitative research involves human beings or the things that human beings produce (documents, notes, etc.). As a result, it is essential that such research be undertaken in a manner that places the safety, security, and needs of participants at the forefront. Although interviews, focus groups, and questionnaires may seem innocuous and “less dangerous” than taking blood samples, it is important to recognize that the way participants are represented in research can be significantly damaging. Try to put yourself in the shoes of the potential participants when designing your research and ask yourself these questions:
- Are the requests you are making of potential participants reasonable?
- Are you putting them at unnecessary risk or inconvenience?
- Have you identified and addressed the specific needs of particular groups?
Where possible, attempting anonymization of data is strongly recommended, bearing in mind that true anonymization may be difficult, as participants can sometimes be recognized from their stories. Balancing the responsibility to report findings accurately and honestly with the potential harm to the participants involved can be challenging. Advice on the ethical considerations of research is generally available from research ethics boards and should be actively sought in these challenging situations.
GETTING STARTED
Pharmacists may be hesitant to embark on research involving qualitative methods because of a perceived lack of skills or confidence. Overcoming this barrier is the most important first step, as pharmacists can benefit from inclusion of qualitative methods in their research repertoire. Partnering with others who are more experienced and who can provide mentorship can be a valuable strategy. Reading reports of research studies that have utilized qualitative methods can provide insights and ideas for personal use; such papers are routinely included in traditional databases accessed by pharmacists. Engaging in dialogue with members of a research ethics board who have qualitative expertise can also provide useful assistance, as well as saving time during the ethics review process itself. The references at the end of this paper may provide some additional support to allow you to begin incorporating qualitative methods into your research.
CONCLUSIONS
Qualitative research offers unique opportunities for understanding complex, nuanced situations where interpersonal ambiguity and multiple interpretations exist. Qualitative research may not provide definitive answers to such complex questions, but it can yield a better understanding and a springboard for further focused work. There are multiple frameworks, methods, and considerations involved in shaping effective qualitative research. In most cases, these begin with self-reflection and articulation of positionality by the researcher. For some, qualitative research may appear commonsensical and easy; for others, it may appear daunting, given its high reliance on direct participant– researcher interactions. For yet others, qualitative research may appear subjective, unscientific, and consequently unreliable. All these perspectives reflect a lack of understanding of how effective qualitative research actually occurs. When undertaken in a rigorous manner, qualitative research provides unique opportunities for expanding our understanding of the social and clinical world that we inhabit.
Further Reading
- Breakwell GM, Hammond S, Fife-Schaw C, editors. Research methods in psychology. Thousand Oaks (CA): Sage Publications Ltd; 1995. [ Google Scholar ]
- Strauss A, Corbin J. Basics of qualitative research. Thousand Oaks (CA): Sage Publications Ltd; 1998. [ Google Scholar ]
- Willig C. Introducing qualitative research in psychology. Buckingham (UK): Open University Press; 2001. [ Google Scholar ]
- Guest G, Namey EE, Mitchel ML. Collecting qualitative data: a field manual for applied research. Thousand Oaks (CA): Sage Publications Ltd; 2013. [ Google Scholar ]
- Ogden R. Bias. In: Given LM, editor. The Sage encyclopedia of qualitative research methods. Thousand Oaks (CA): Sage Publications Inc; 2008. pp. 61–2. [ Google Scholar ]
This article is the seventh in the CJHP Research Primer Series, an initiative of the CJHP Editorial Board and the CSHP Research Committee. The planned 2-year series is intended to appeal to relatively inexperienced researchers, with the goal of building research capacity among practising pharmacists. The articles, presenting simple but rigorous guidance to encourage and support novice researchers, are being solicited from authors with appropriate expertise.
Previous article in this series:
Bond CM. The research jigsaw: how to get started. Can J Hosp Pharm . 2014;67(1):28–30.
Tully MP. Research: articulating questions, generating hypotheses, and choosing study designs. Can J Hosp Pharm . 2014;67(1):31–4.
Loewen P. Ethical issues in pharmacy practice research: an introductory guide. Can J Hosp Pharm. 2014;67(2):133–7.
Tsuyuki RT. Designing pharmacy practice research trials. Can J Hosp Pharm . 2014;67(3):226–9.
Bresee LC. An introduction to developing surveys for pharmacy practice research. Can J Hosp Pharm . 2014;67(4):286–91.
Gamble JM. An introduction to the fundamentals of cohort and case–control studies. Can J Hosp Pharm . 2014;67(5):366–72.
Competing interests: None declared.
Higher Ed Professor
Demystifying higher education.
- Productivity
- Issue Discussion
- Current Events
Tips for novice qualitative researchers when using quotes
O ne of the biggest struggles that new qualitative researchers experience is how to make use of their data, specifically the use of quotes. The balance is a delicate one where you want to maintain fidelity to the voices of your participants and other data sources, yet you cannot simply dump pages and pages of transcriptions into the findings section. You have to identify the most central elements, pick out representative quotes, and at the most basic level tell a story about what you found. In this post, I want to provide tips for novice qualitative researchers when using quotes to help navigate this difficult balancing act.

It can be helpful to think about how a good journalist would convey information in a newspaper or magazine article. The best reporters are able to blend in the voices of their sources (using quotes) along with context setting prose.
There is a balancing act that conveys the information of the article using an effective mix of direct quotations and other text to understand and evaluate the facts being presented.
As the reader, you hopefully have enough information by the end of the story to understand what is happening but also to consider the various viewpoints presented in the story.
In many ways, this is exactly what you want to do with the presentation of your findings. You want to present the main ideas (i.e. your themes) along with supporting quotations.
The way you talk about the data, as in the case of the reporter, will provide additional context and a narrative to help guide the reader through the information presented.
Along these same lines, as the author, you will have to determine your voice in the writing of your findings.
Are you an impartial observer? Are you a participant in the conversation?
The type of study you are conducting will also provide some hints as to the approach you may take.
For instance, an ethnography would suggest the author as a more active participant as compared to a traditional case study approach.
Of course, as you discussed in your positionality section of your research, there are no truly impartial observers.
Rather, novice researchers often write their findings in a more neutral tone rather than overtly inserting themselves into the narrative. In many cases, this is because students so used to the rhetoric around bias as a negative try to remove themselves to make their research less biased.
In other cases, it is simply easier to “report the news” than be a part of the story.
Moreover, the author must decide how much of a quote to use in a particular section.
The options can range from a small phrase through a sentence to a longer block quotation. Often, new qualitative researchers will too liberally use block quotations.
In other words, a key phrase or sentence may be all they really want to convey but they include a paragraph to “provide context.”
Avoid this trap.
If you need to provide context for a quote, then put this in your own words rather than in the participants.
Along the same lines, nearly every qualitative research falls into the trap of falling in love with a one or two participants.
It is amazing to sit down with an interviewee who provides great insight, is exceptionally quotable, and hits on everything you want to address in your findings.
However, no matter how great a participant might be, you have to be careful that you are relying too much on a single or even a few participants.
Likewise, there will always be those dud interviews that do not provide much information.
As the author, try to vary up the participants you use in your findings. There may be a good reason to focus on one or two people in a section. For example, they may have been the only people with a given perspective.
Ultimately, to the extent possible, you want to vary how often you are quoting your participants.
If you see that you are using one or two for more than a paragraph or two, ask yourself if there are others who may not be quite as quotable, but still provide a shared perspective or view on the topic you are discussing.
There are two ways to approach which quotes you will use that will provide the best information while also demonstrating the range of your data (which is the primary reason to vary your sources).
First, your goal should be to begin by identify the best and most exemplary quotes for each point that you want to make, a process that begins with data analysis but is not completed until writing.
Second, you want to make sure to spread these quotes around across participants.
You will likely have a participant or two that have the most amazing quotes for every section of your findings. That is great and this is a good problem to have, but you obviously need to use more people or sources of data.
So after you identify the best quotes, look to see if you are relying too much on a few sources through the findings chapter or inside of individual sections.
If you are, then look at who has the second-best quote.
It might not be quite as pithy as your exemplary quote, but it still makes the point you are trying to convey. Replace some of your exemplary quotes with some second or even third best quotes to provide better balance throughout your discussion of the data.
Of course, there is far more that could be said when discussion how to write up qualitative data. My goal here as been to provide some tips for novice qualitative researchers when using quotes and discussing findings.
One of the great challenges of qualitative research is constantly working to improve your writing and how you convey the voices of your data.
Whether you are a novice or an experienced qualitative researcher, this is an ongoing challenge and I hope you continue working to improve the craft of qualitative research.
Beyond the default colon: Effective use of quotes in qualitative research
- The Writer's Craft
- Open access
- Published: 22 November 2019
- Volume 8 , pages 360–364, ( 2019 )
Cite this article
You have full access to this open access article

- Lorelei Lingard 1
11k Accesses
65 Citations
38 Altmetric
Explore all metrics
Avoid common mistakes on your manuscript.
In the Writer’s Craft section we offer simple tips to improve your writing in one of three areas: Energy, Clarity and Persuasiveness. Each entry focuses on a key writing feature or strategy, illustrates how it commonly goes wrong, teaches the grammatical underpinnings necessary to understand it and offers suggestions to wield it effectively. We encourage readers to share comments on or suggestions for this section on Twitter, using the hashtag: #how’syourwriting?
Last week the ‘e’ key died on my laptop. It’s a first-world problem, I’ll admit, but it really threw my writing for a loop—a lot of words require an ‘e’ key. Reflecting on what other keys I could not do without, I made a quick shortlist: comma, ‘ly’ and colon. The comma because its absence would consign me to the sort of breathy, adolescent writing that fills social media. The ‘ly’ because without that duo I can’t make most of the adverbs that prop up my first drafts. And the colon because I’m a qualitative researcher. How would I introduce quotes if the colon key were out of order?
I’m only partly joking. Every qualitative researcher confronts the challenge of selecting the right quotes and integrating them effectively into their manuscripts. As writers, we are all guilty of resorting to the default colon as an easy way to tuck quotes into our sentences; as readers, we have all suffered through papers that read like a laundry list of quotes rather than a story about what the writer learned. This Writer’s Craft instalment offers suggestions to help you choose the right quotes and integrate them with coherence and style, following the principles of authenticity and argument.
Authenticity
At the point of manuscript writing, a qualitative researcher is swimming in a sea of data. Innumerable transcript excerpts have been copied and pasted into data analysis software or (for the more tactile among us) onto multi-coloured sticky notes. Some of these excerpts we like very much. However, very few of them will make it into the final manuscript, particularly if we are writing for publication in a health research or medical education journal, with their 3000–4000 word limits.
Selecting the best quotes from among these cherished excerpts is harder than it looks. We should be guided by the principle of authenticity: does the quote offer readers first hand access to dominant patterns in the data? There are three parts to selecting a good, authentic quote: the quote is illustrative of the point the writer is making about the data, it is reasonably succinct, and it is representative of the patterns in data. Consider this quote, introduced with a short phrase to orient the reader:
Rather than feeling they were changing identities as they went through their training, medical students described the experience of accumulating and reconciling multiple identities: ‘the “life me”, who I was when I started this, is still here, but now there’s also, like, a “scientific me” as well as a sort of “doctor me”. And I’m trying to be all of that’ (S15) .
This quote is illustrative, providing an explicit example of the point that student identity is multiplying as training unfolds. It is succinct, expressing efficiently what other participants took pages to describe. And it is representative, remaining faithful to the overall sentiments of the many participants reporting this idea.
We have all read—and written!—drafts in which the quoted material does not reflect these characteristics. The remainder of this section addresses these recurring problems.
Is the quote illustrative?
A common challenge is the quote that illustrates the writer’s point implicitly, but not explicitly. Consider this example:
Medical students are undergoing a process of identity-negotiation: we’re ‘learning so much all the time, and some of it is the science stuff and some of it is professional or, like, practical ethical things, and we have to figure all that out’ (S2).
For this quote to serve as evidence for the point of identity-negotiation, the reader must infer that ‘figure all that out’ is a reference to this process. But readers may read their own meaning into decontextualized transcript extracts. Explicit is better, even if it sacrifices succinctness. In fact, this is the right quote, but we had trimmed away the first three sentences where ‘figuring out identity’ got explicit mention. The quote could be lengthened to include these sentences, or, to preserve succinctness, just that quoted phrase can be inserted into the introduction to the quote:
Medical students are ‘figuring out identity’, a process of negotiation in which they are ‘learning so much all the time, and some of it is the science stuff and some of it is professional or, like, practical ethical things, and we have to figure all that out’ (S2).
Is the quote succinct?
Interview transcripts are characterized by meandering and elliptical or incomplete speech. Therefore, you can search diligently and still come up with a 200-word quote to illustrate your 10-word point. Sometimes the long quote is perfect and you should include it. Often, however, you need to tighten it up. By including succinctness as part of the authenticity principle, my aim is to remind writers to explicitly consider whether their tightening up retains the gist of the quote.
The previous example illustrates one tightening technique: extract key phrases and integrate them into your own, introductory sentence to the quote. Another solution is to use the ellipsis to signal that you have cut part of the quote out:
Identity formation in the clinical environment is also influenced by materials and tools, ‘all this stuff you’ve never used before … you don’t know where it is or how to use it, and don’t even get me started on the computerized record. … So many hours and I’m still confused, am I ever going to know where to enter things?’ (S7) .
The first ellipsis signals that something mid-sentence has been removed. In this case, this missing material was an elaboration of ‘all this stuff’ that mentioned other details not relevant to the point being made. The second ellipsis follows a period, and therefore signals that at least one sentence has been removed and perhaps more. When using an ellipsis, only remove material that is irrelevant to the meaning of the quote, not relevant material that importantly nuances the meaning of the quote. The goal is not a bricolage which cuts and pastes tiny bits so that participants say what you want them to; it is a succinct-enough representation that remains faithful to the participant’s intended meaning.
Changing the wording of a quotation always risks violating the authenticity principle, so writers must do it thoughtfully. Two other situations, however, may call for this approach: to maintain the grammatical integrity of your sentence and to tidy up oral speech Footnote 1 . The first is usually not problematic, particularly if you are altering for consistent tense or for agreement of verb and subject or pronoun and antecedent, or replacing a pronoun with its referent. Square brackets signal such changes:
Participants from the community hospital setting, however, ‘[challenged] the assumption of anonymity when evaluating teachers’. (verb tense changed from present to past)
The second situation can be trickier: when should you tidy up the messiness of conversational discourse? Interview transcripts are replete with what linguists refer to as ‘fillers’ or ‘hesitation markers’, sounds and words such as ‘ah/uh/um/like/you know/right’ [ 1 ]. There is general agreement among qualitative scholars that quotes should be presented verbatim as much as possible, and those engaged in discourse and narrative analysis will necessarily analyze such hesitations as part of the meaning. In other applied social research methodologies, however, writers might do some ‘light tidying up’ both for readability and for ethical reasons, as long as they do not undermine authenticity in doing so [ 2 ]. Ethical issues include the desire not to do a disservice to participants by representing the um’s and ah’s of their natural speech, and the concern to protect participant anonymity by removing identifiable linguistic features such as regional or accented speech.
Finally, an emerging strategy for succinctness is to put the quotes into a table. Many qualitative researchers resent the constraints of the table format as an incursion from the quantitative realm. However, used thoughtfully, it can offer a means of presenting complex results efficiently. In this example, Goldszmidt et al. name, define and illustrate five main types of supervisor interruptions that they observed during their study of case review on internal medicine teaching teams (Tab. 1 ; [ 3 ]).
This is a nice example of how ‘Tab. 1 ’, conventionally used in quantitative research papers for demographic details of the research sample, can be re-conceptualized to feature the key findings from a qualitative analysis. Tables should be supplemented, however, with narrative explanation in which the writer contextualizes and interprets the quoted material. More on this in the section on Argument.
Is the quote representative?
We have all been tempted to include the highly provocative quote (that thing we cannot believe someone said on tape), only to realize by the third draft that it misrepresents the data and must be relinquished. Quote selection should reflect strong patterns in the data; while discrepant examples serve an important purpose, their use should be purposeful and explicit. Your quote selection should also be distributed across participants, in order that you represent the data set. This may mean using the second- or third-best example rather than continuing to quote the same one or two highly articulate individuals.
You must provide sufficient context that readers can accurately infer the meaning of the quote. Sometimes this means including the interviewer’s question as well as the participant’s answer. In focus group research, where the emphasis is on the group discussion, it might be necessary to quote an exchange among participants rather than extracting individual comments. This example illustrates this technique:
Interviewer: And, in your experience, how do the students respond to your feedback about how well they communicated? SP1: Oh, really well, it’s really important to the students, they listen to what we say about their performance— Interruption with overlapping talk SP4: Well, yeah, on a good day maybe, sure. But not every time. Lots of sessions I feel like we’re probably more like props to them, so how well we think they did, I’m not sure that matters. SP3: Don’t you find it depends on the student? (FG2)
Of course, such a long excerpt threatens the goal of succinctness. Alternatively, you could use multiple quotes from this excerpt in a single sentence of your own:
Some standardized patients in the group believed that their assessor role was ‘really important to the students, they listen to what we say about their performance’, while others argued that ‘we’re probably more like props to them, so how well we think they did, I’m not sure that matters’. (FG2)
Sometimes a quote is representative but also, therefore, identifiable, jeopardizing confidentiality:
One participant explained that, ‘as chair of the competency committee, I prioritize how we spend our time. So that we can pay sufficient attention to this 2nd year resident. She’s supposed to be back from maternity leave but she had complications so her rotations need some altering for her to manage.’ (CCC4, P2)
In this case, the convention of using a legend (Clinical Competency Committee 4, participant 2) to attribute the quote may be insufficient to protect anonymity. If the study involves few programs and the methods identify them (e.g., Paediatrics and Medicine) and name the institution (e.g., Western University), the speaker may be identifiable to some readers, as may the resident.
Quoted material does not stand on its own: we must incorporate it into our texts, both grammatically and rhetorically. Grammatical incorporation is relatively straightforward, with one main rule to keep in mind: quoted material is subject to the same sentence-level conventions for grammar and punctuation as non-quoted material. Read this example aloud:
Arts and humanities teaching offers an opportunity for faculty to connect with medical students on a different level, ‘we can share how we feel about the work of caring, what it costs us, how it rewards us, as human beings’ (F9).
Your ear likely hears that this should be two sentences. But quotation marks seem to distract us from this, and we create a run-on sentence by putting a comma between the sentences. An easy correction is to replace the comma with a colon.
Arts and humanities teaching offers an opportunity for faculty to connect with medical students on a different level: ‘we can share how we feel about the work of caring, what it costs us, how it rewards us, as human beings’ (F9).
Many writers rely on the colon as their default mechanism for integrating quoted material. However, while it is often grammatically accurate, it is not always rhetorically sufficient. That is, the colon doesn’t contextualize, it doesn’t interpret. Instead, it ‘drops’ the quote in and leaves the reader to infer how the quoted material illustrates or advances the argument. This is problematic because it does not fulfil the requirement for adequacy of interpretation in presenting qualitative results. As Morrow argues, writers should aim for a balance of their interpretations and supporting quotations: ‘an overemphasis on the researcher’s interpretations at the cost of participant quotes will leave the reader in doubt as to just where the interpretations came from; an excess of quotes will cause the reader to become lost in the morass of stories’ [ 4 ]. (p. 256).
There are many techniques for achieving this balance between researcher interpretations and supporting quotations. Some techniques retain the default colon but attend carefully to the material that precedes it. Consider the following examples:
One clinician said: ‘Entrustment isn’t a decision, it’s a relationship’. (F21) One clinician argued: ‘Entrustment isn’t a decision, it’s a relationship’. (F21) One clinician in the focus group disagreed with the idea that entrustment was about deciding trainee progress: ‘Entrustment isn’t a decision, it’s a relationship’. (F21) Focus group participants debated the meaning of entrustment. Many described it matter-of-factly as ‘the process we use to decide whether the trainee should progress’, while a few argued that ‘entrustment isn’t a decision, it’s a relationship’. (F21)
These examples offer progressively more contextualization for the quote. The first example simply drops the quote in following the nondescript verb, ‘said’, offering no interpretive gloss and therefore exerting minimal rhetorical control over the reader. The second offers some context via the verb ‘argued’, which interprets the participant’s positioning or tone. The third interprets the meaning of the quote even more by situating it in the context of a focus group debate. And the fourth eschews the default colon entirely, integrating two quotes into the narrative structure of the author’s sentence to illustrate the dominant and the discrepant positions on entrustment in this focus group debate.
Integrating quotes into the narrative structure of your sentence, like the last example, offers two advantages to the writer. First, it interprets the quote for the reader and therefore exerts strong rhetorical control over the quote’s meaning. Second, it offers variety and style. If your goal is compelling prose, variety and style should not be underestimated. We have all had the experience of reading Results sections that proceed robotically: point-colon-quote, point-colon-quote, point-colon-quote …. If only to make the reader’s experience more enjoyable, your revision process should involve converting some of these to integrated narration.
Notwithstanding the goal of succinctness, sometimes you will include a longer quote because it beautifully illustrates the point. However, a long quote may offer opportunities for readers to focus on images or phrases other than those you intended, therefore creating incoherence in the argument you are making about your results. To guard against this, you might try the ‘quotation sandwich’ technique [ 5 ] of both an introductory phrase that sets up the context of the quote and a summary statement following it emphasizing why you consider it important and what you are using it to illustrate.
Finally, how many quotes do you need to support your point? More is not necessarily better. One quote should be sufficient to illustrate your point. Some points in your argument may not require a quoted excerpt at all. Consider this example, in which the first sentence presents a finding that is not illustrated with a quotation:
Residents described themselves as being always tired. However, their perceptions of the impact of their fatigue varied, from ‘not a factor in the care I provide’ (R8) to ‘absolutely killing me … I’m falling asleep at the bedside’ (R15).
The finding that residents are always tired does not require illustration. It is readily understandable and will not surprise anyone; therefore, following it with the quote ‘I’m tired all the time’ (R2) will feel redundant. The second part of the finding, however, benefits from illustration to show the variety of perception regarding impact.
If you do use multiple quotes to illustrate a point in your argument, then you must establish the relations between them for the reader. You can do this between the quoted excerpts or after them, as modelled above with the four examples used to illustrate progressively stronger quote contextualization.
In conclusion, quotes can be the life’s blood of your qualitative research paper. However, they are the evidence, not the argument. They do not speak for themselves and readers cannot infer what you intend them to illustrate. The authenticity principle can help you select a quote that is illustrative, succinct and representative, while the argument principle can remind you to attend to the grammatical and the rhetorical aspects of integrating the quote into the story you are telling about your research.
A third situation is beyond the scope of this piece: translating quoted material from another language into English. For careful consideration of this issue, please see Helmich et al. [ 6 ].
Gunnel T. Planning what to say: Uh and um among the pragmatic markers. In Kaltenbock G, Keizer E, Lohmann A. (eds). Outside the Clause: Form and Function of Extra-Clausal Constituents. Amsterdam/Philadelphia: John Benjamins; 2016: pp. 97–122.
Corden A, Sainsbury R. Using Verbatim Quotations in Reporting Qualitative Social Research: Researchers’ views. University of. York: York: Social Policy Research Unit; 2006.
Google Scholar
Goldszmidt M, Aziz N, Lingard L. Taking A Detour: Positive And Negative Impacts Of Supervisor Interruptions During Admission Case Review, Acad Med. 2012;87:1382–8.
Morrow SL. Quality and Trustworthiness in Qualitative Research in Counseling Psychology. J Couns Psychol. 2005;52:250–60.
Article Google Scholar
Graff G, Birkenstein C. ‘They Say/I Say’: The Moves that Matter in Academic Writing. 4th edition. London: Norton & Co; 2018.
Helmich E, Cristancho S, Diachun L, et al. ‘How would you call this in English?’ Being reflective about translations in international, cross-cultural qualitative research. Perspect Med Educ. 2017;6:127.
Download references
Author information
Authors and affiliations.
Centre for Education Research & Innovation and Department of Medicine, Health Sciences Addition, Schulich School of Medicine & Dentistry, Western University, London, Canada
Lorelei Lingard
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Lorelei Lingard .
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License ( http://creativecommons.org/licenses/by/4.0/ ), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Reprints and permissions
About this article
Lingard, L. Beyond the default colon: Effective use of quotes in qualitative research. Perspect Med Educ 8 , 360–364 (2019). https://doi.org/10.1007/s40037-019-00550-7
Download citation
Published : 22 November 2019
Issue Date : December 2019
DOI : https://doi.org/10.1007/s40037-019-00550-7
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Find a journal
- Publish with us
- Track your research
Market Research
17 research quotes to inspire and amuse you
Being a researcher requires dedication, hard work and more than a little inspiration. Here’s something to boost the last item on that list.
We’ve sourced some of the most interesting and thought-provoking research quotes we can find. We hope they’ll leave you feeling inspired and motivated to start – or complete – your best ever research project.
As these quotes show, research is a common thread running through all kinds of professions and pursuits, from Ancient Rome right up to the present day. If you practice research, you’re part of a long list of people throughout history, all dedicated to finding new knowledge and ideas that ultimately make the world a better place.
Looking for the most recent trends to enhance your results?
Free eBook: The new era of market research is about intelligence
1. “No research without action, no action without research”
- Kurt Lewin
Lewin (1890-1947) was a German-American social psychologist. He’s known for his theory that human behavior is a function of our psychological environment.
2. “Research is seeing what everybody else has seen and thinking what nobody else has thought.”
- Albert Szent-Györgyi
Szent-Györgyi (1893-1986) was a Hungarian pharmacologist known for his work on vitamins and oxidation. He was awarded the Nobel Prize in Physiology or Medicine in 1937.
3. "Bad news sells papers. It also sells market research."
- Byron Sharp
Sharp is Professor of Marketing Science and Director of the Ehrenberg-Bass Institute, the world’s largest centre for research into marketing.
4. "In fact, the world needs more nerds."
- Ben Bernanke
Bernanke is an American economist and former chair of the board of governors at the United Stares Federal Reserve.
5. "Research is what I'm doing when I don't know what I'm doing."
- Wernher von Braun
Von Braun (1912-1977) was a German-American physicist and rocket engineer whose team launched the first US satellite into space.
6. "Research is formalized curiosity. It is poking and prying with a purpose."
- Zora Neale Hurston
Hurston (1891-1960) was an American anthropologist and writer known for her research and writing on slavery, race, folklore and the African-American experience.
7. "Research is creating new knowledge."
- Neil Armstrong
Armstrong (1930-2012) was an American astronaut famed for being the first man to walk on the Moon.
8. "I believe in innovation and that the way you get innovation is you fund research and you learn the basic facts."
- Bill Gates
Gates needs little introduction – he’s an entrepreneur, philanthropist and the founder of Microsoft.
9. “The best research you can do is talk to people”
- Terry Pratchett
Pratchett is an award-winning British science fiction and fantasy author. He was knighted in 2009. He is known for The Hitch Hiker’s Guide to the Galaxy and the Discworld series.
10. “Research means that you don’t know, but are willing to find out”
- Charles F. Kettering
Kettering (1876-1958) was an American engineer, known for inventing the electric starter used in combustion engines, as well as other automobile technologies.
11. “Nothing has such power to broaden the mind as the ability to investigate systematically and truly all that comes under thy observation in life.”
- Marcus Aurelius
Marcus Aurelius (121-180) was a Roman Emperor and Stoic philosopher.
12. “It is a good thing for a research scientist to discard a pet hypothesis every day before breakfast.“
- Konrad Lorenz
Lorenz (1903-1989) was an Austrian biologist known for his game-changing research on animal behavior. He was jointly awarded the Nobel Prize in Physiology or Medicine in 1973.
13. “Research is something that everyone can do, and everyone ought to do. It is simply collecting information and thinking systematically about it.”
- Raewyn Connell
Connell is an Australian sociologist. She is a former professor of at the University of Sydney and is known for her work on gender and transgender studies.
14. “As for the future, your task is not to foresee it, but to enable it.”
- Antoine de Saint Exupery
De Saint Exupery (1900-1944) was a French aviator, author and poet, best known for his story The Little Prince, one of the best-selling books of all time.
15. “It is a capital mistake to theorize before one has data.”
- Arthur Conan Doyle (writing as Sherlock Holmes)
Conan Doyle (1859-1930) was a British crime writer and creator of the legendary Sherlock Holmes, master of deduction.
16. “If we knew what we were doing, it would not be called research, would it?”
- Albert Einstein
Maybe the most famous scientist of all time, Albert Einstein (1879-1955) was a German physicist who came up with the theory of relativity. However, it was his description of the photoelectric effect, the interplay between light and electrically charged atoms, that won him the Nobel Prize for Physics in 1921.
17. “The power of statistics and the clean lines of quantitative research appealed to me, but I fell in love with the richness and depth of qualitative research.”
- Brené Brown
Brown is a researcher and storyteller studying courage, shame, empathy and vulnerability. She is a best-selling author and inspirational speaker. She is a research professor at the University of Houston.
Sarah Fisher
Related Articles
June 27, 2023
The fresh insights people: Scaling research at Woolworths Group
June 20, 2023
Bank less, delight more: How Bankwest built an engine room for customer obsession
June 16, 2023
How Qualtrics Helps Three Local Governments Drive Better Outcomes Through Data Insights
April 1, 2023
Academic Experience
Great survey questions: How to write them & avoid common mistakes
March 21, 2023
Sample size calculator
March 9, 2023
Experience Management
X4 2023: See the XM innovations unveiled for customer research, marketing, and insights teams
February 22, 2023
Achieving better insights and better product delivery through in-house research
December 6, 2022
Improved Topic Sentiment Analysis using Discourse Segmentation
Stay up to date with the latest xm thought leadership, tips and news., request demo.
Ready to learn more about Qualtrics?
- Open access
- Published: 25 April 2024
A qualitative evaluation of factors influencing Tumor Treating fields (TTFields) therapy decision making among brain tumor patients and physicians
- Priya Kumthekar 1 , 2 ,
- Madison Lyleroehr 3 ,
- Leilani Lacson 7 ,
- Rimas V. Lukas 1 , 2 ,
- Karan Dixit 1 , 2 ,
- Roger Stupp 1 , 2 ,
- Timothy Kruser 7 ,
- Jeff Raizer 1 , 2 ,
- Alexander Hou 6 ,
- Sean Sachdev 5 , 2 ,
- Margaret Schwartz 1 , 2 ,
- Jessica Bajas PA 1 ,
- Ray Lezon 1 , 2 ,
- Karyn Schmidt 1 ,
- Christina Amidei 4 , 2 &
- Karen Kaiser 3
BMC Cancer volume 24 , Article number: 527 ( 2024 ) Cite this article
Metrics details
Tumor Treating Fields (TTFields) Therapy is an FDA-approved therapy in the first line and recurrent setting for glioblastoma. Despite Phase 3 evidence showing improved survival with TTFields, it is not uniformly utilized. We aimed to examine patient and clinician views of TTFields and factors shaping utilization of TTFields through a unique research partnership with medical neuro oncology and medical social sciences.
Adult glioblastoma patients who were offered TTFields at a tertiary care academic hospital were invited to participate in a semi-structured interview about their decision to use or not use TTFields. Clinicians who prescribe TTFields were invited to participate in a semi-structured interview about TTFields.
Interviews were completed with 40 patients with a mean age of 53 years; 92.5% were white and 60% were male. Participants who decided against TTFields stated that head shaving, appearing sick, and inconvenience of wearing/carrying the device most influenced their decision. The most influential factors for use of TTFields were the efficacy of the device and their clinician’s opinion. Clinicians ( N = 9) stated that TTFields was a good option for glioblastoma patients, but some noted that their patients should consider the burdens and benefits of TTFields as it may not be the desired choice for all patients.
Conclusions
This is the first study to examine patient decision making for TTFields. Findings suggest that clinician support and efficacy data are among the key decision-making factors. Properly understanding the path to patients’ decision making is crucial in optimizing the use of TTFields and other therapeutic decisions for glioblastoma patients.
Peer Review reports
Introduction
Glioblastoma is the most common malignant primary brain tumor in adults, accounting for over 50% of all gliomas, with an annual incidence rate of 3 to 4 cases per 100,000 people, resulting in 240,000 newly diagnosed cases worldwide each year [ 1 , 2 ]. Since 2005, the standard treatment for glioblastoma has been surgical resection followed by radiotherapy with concurrent and adjuvant temozolomide (TMZ). For newly diagnosed glioblastomas, the addition of TMZ to surgery and radiation therapy prolongs median survival from 12.1 to 14.6 months and increases the five-year survival rate from 2 to 10% [ 3 ].
In addition to the current standard of care, patients with glioblastomas can receive a more recently approved therapy called Tumor Treating Fields Therapy (TTFields) (Optune™). TTFields utilizes a portable, battery-operated device that delivers a low-intensity, alternating electric field to the tumor via surface electrodes (transducer arrays) [ 4 ]. The electric field disrupts the normal mitotic process for tumor cells and leads to cancer cell death [ 5 ]. In patients with recurrent glioblastoma brain tumors, TTFields has shown clinical efficacy comparable to that of active chemotherapies, without many of the side effects of chemotherapy [ 6 , 7 ]. TTFields was first FDA approved in the recurrent setting after it showed non-inferiority in a phase 3 trial compared to “physician’s best choice” treatment [ 8 ]. Subsequently, a first line randomized Phase 3 trial compared TTFields plus TMZ to TMZ alone among 695 glioblastoma patients who had completed radiochemotherapy. The TTFields treatment arm showed a significant improvement in both progression-free survival (median progression-free survival was 6.7 months in the TTFields plus TMZ group and 4.0 months in the TMZ alone group) and overall survival (median overall survival 20.9 months versus 16.0 months), leading to FDA approval of TTFields in the first line setting [ 9 , 10 ]. Side effects reported in the TTFields plus TMZ group were limited to mild to moderate skin toxicity under the transducer arrays [ 10 ]. Following FDA approval to use TTFields for glioblastoma and, subsequently, mesothelioma [ 11 ], the National Comprehensive Cancer Network (NCCN) added TTFields to its guidelines for evidence-based management of new or recurrent glioblastoma in 2018 [ 12 , 13 ].
Despite regulatory and national guideline support for TTFields, evidence demonstrating improved survival with TTFields, no severe side effects from the device, and limited treatments for glioblastoma, not all patients who qualify for TTFields choose to use the device. Moreover, there has been reluctance among neuro-oncologists to adopt TTFields [ 12 ]. This qualitative study aimed to grow our understanding of glioblastoma patients’ decision on whether or not to use TTFields, the role of clinicians in their decisions, and clinicians’ views of TTFields.
Materials and methods
Patient enrollment.
The study protocol was approved by the institutional review board of Northwestern University and all patients enrolled on study provided written informed consent prior to any study-related procedures. Patients with a glioblastoma receiving treatment at the Malnati Brain Tumor Institute at the Lurie Comprehensive Cancer Center of Northwestern University who had been offered treatment with TTFields and had decided whether to initiate TTFields therapy were eligible to participate in the study. Other eligibility criteria included: able to speak and understand English, age 18 or older, and cognitively able to complete a study interview. We aimed to interview up to 50 glioblastoma patients who had been offered TTFields. In 2020, 180 new glioblastoma patients were seen at the Malnati Brain Tumor Institute and 51 TTFields prescriptions were written.
Patients were enrolled consecutively between June of 2020 and February of 2021, the entirety of which occurred during Covid-19 pandemic; therefore, consenting and interviews occurred remotely. In the first month of the project, clinicians provided the names of glioblastoma patients who had been offered TTFields for study inclusion; subsequently, a study coordinator (co-author LL) identified glioblastoma patients in the electronic medical record who had been offered or who had decided to use TTFields. Clinicians then confirmed patients were physically and cognitively able to participant and the study coordinator contacted eligible patients via telephone, explained the study, and obtained informed consent electronically. The approximately 30-minute study interview was subsequently conducted via phone by the study coordinator, who had extensive experience conducting patient interviews. A semi-structured interview guide was used to gather patient input on their views of TTFields, factors that influenced their TTFields decision, and their perceptions of whether their clinician wanted them to use TTFields. Patients also completed the Control Preference Scale, which is a one-item measure of preferred role in medical decision making that has been tested and validated with cancer patients [ 14 , 15 , 16 ]. Patients received a $25 Visa gift card following participation. Interviews were audio recorded to ensure comprehensive capture of all relevant patient-reported information.
Clinician sample
Clinicians in the Malnati Brain Tumor Institute of Northwestern University who offer and prescribe TTFields therapy received an invitation via email to participate in a study interview. This included physicians (neuro-oncologists) and advanced practitioners (Advanced Practice Nurses and Physicians Assistants). All eligible physicians and advanced practitioners interviewed were specifically trained and certified to prescribe tumor treating fields by Novocure through the company-run training program. This is required to be able to prescribe this device to patients. Clinician participants provided verbal consent via telephone prior to participating in a telephone interview. As with the patient interviews, clinicians’ interviews were audio recorded. A semi-structured interview guide was used to gather their views of TTFields. Clinicians were not compensated for participating.
Data analysis
The interviewer entered detailed notes into an Excel database following each interview. The database became the basis for a preliminary analysis of each interview question. Notes for each question were reviewed by the study coordinator, an experienced qualitative analyst (co-author ML), and a qualitative researcher (co-author KK) to identify preliminary themes. Next, the three study team members reviewed the interview transcripts to finalize themes, confirm themes were comprehensive and reflected the data, and to identify supporting quotations.
Patient results
One-hundred and five glioblastoma patients were identified via physician recommendation or medical record review between June of 2020 and February of 2021. Of these, a total of 11 (10.5%) patients were deemed ineligible because they were not offered TTFields ( n = 2), had gone to another center for treatment ( n = 1), had entered hospice ( n = 6), or died prior to recruitment ( n = 2). Twenty-one patients (20.0%) were excluded per clinician recommendation. Reasons for clinician-recommended exclusion included cognitive issues, speech difficulties, and illness severity. Twenty (19.1%) patients were unresponsive to recruitment efforts, and 13 (12.4%) patients declined to participate. Individual interviews were conducted with 40 (38.1%) individuals with glioblastoma. Among the 40 participants (Table 1 ), the mean age was 53 years (range 21–77 years). Most participants were white (92.5%), married (80.0%), and male (60.0%). The study coordinator confirmed each patient’s TTFields status at the time of recruitment. Thirty-two participants (80.0%) chose to pursue TTFields therapy, while eight (20.0%) did not use TTFields. The TTFields group and the no-TTFields group were similar in age and gender. Patients who declined TTFields were less likely to use TTFields resources (Table 1 ); however, we would expect that TTFields users would be more apt to seek out information about TTFields.
Control Preference Scale results are shown in Table 2 . In both groups, patients most often preferred to make decisions for themselves after considering their doctors opinion ( n = 15, 46.9% among patients who utilized TTFields, n = 5, 62.5% among patients who declined TTFields). Six (18.8%) of the patients who chose TTFields preferred to have their doctor make their medical decisions either with consideration for the patient’s opinion ( n = 3, 9.4%) or on their own ( n = 3, 9.4%). In contrast, none of the patients who declined TTFields preferred to have their doctor make their decisions.
Participants who chose TTFields
Participants who chose TTFields noted downsides associated with the treatment. The most frequently mentioned downside of TTFields was the burden of changing the TTFields arrays, which happened frequently (every few days) and could be painful. The heat of the device on one’s head was also noted as a downside, along with the discomfort of wearing the cap and the burden on caregivers who assist them when changing their cap and arrays. Some users of TTFields experience skin reactions, such as blisters or itching. Participants also noted it could be difficult to sleep or shower with the device, and carrying the device was cumbersome.
However, many of the patients who chose TTFields came to accept the burdens of using the device. For example, some noted that shaving their head for TTFields was easy and/or worth the trouble. “The head shaving part was easy because I had lost most of my hair already.” Another participant said, “I used it (TTFields) for two years, and if they told me that I had to re-shave my head and use it longer, I would do it.” Likewise, participants who chose TTFields said that the appearance of the device could be bothersome, but they were not deterred by it. In fact, one participant had a positive experience due to the visible nature of TTFields: “Pretty much right after I was fitted for it, I think the next day, I was back at work. So, it was kind of awkward at first, but I actually had some good conversations with people about it in the days and weeks after that.”
For the patients who chose TTFields, the efficacy of TTFields was the most frequently cited reason for choosing to use the device. As shown in Table 3 , they described efficacy in several ways, including extension of life, shrinking one’s tumor, and the device being supported by clinical studies. Extension of life was cited by over a third ( n = 13, 40.6%) of those who chose TTFields (Table 3 ). One participant stated, “I don’t want to die. And I feel that if I don’t have this, that I will die.” Another participant spoke of the value of extending life even with potential negative effects: “Am I willing to be slightly inconvenienced for an additional five months of life? Yeah, I’ll go with that deal.” For others, clinical evidence supporting the efficacy of TTFields, particularly the extension of life, was pivotal in their decision to undergo TTFields. One participant stated that the biggest factor in their decision was “without question, FDA approved that this treatment does extend your life by a significant percentage.”
The second most influential factor reported by those who chose TTFields was their doctor’s opinion ( n = 9, 28.1%). As one participant stated, “We (participant and their spouse) absolutely believe in both the physicians who recommended it (TTFields). So, we really trust them a lot.” All participants who reported that their doctor’s opinion was the most influential factor in their decision to undergo TTFields also reported that their doctor recommended TTFields.
Familial considerations were cited as the most influential factor for four (12.5%) participants. Three of the four people in this group noted that they wanted to extend time with their families. Several other influences were mentioned by one person each (Table 3 ). For example, one participant said she chose TTFields after hearing about the experience of a family friend who had used TTFields and recommended it despite the inconveniences of wearing the device.
Participants who declined TTFields
For those glioblastoma patients who chose not to use TTFields, the most influential factor in their decision was the requirement to shave their head ( n = 4, 50.0%) (Table 4 ). “I know some people probably think that’s kind of silly, like, ‘You have cancer, so who cares if you have hair or not?’ But it’s just been really hard for me.” Another influential factor was the visibility of TTFields ( n = 3, 37.5%). For example, two participants did not like the idea of wearing the device at work. One of them said, “I was still working, and at that time, I did not share with them everything that was going on. So, it would have definitely exposed things, and who knows what would have happened after that.”
Other reasons for declining TTFields included the inconvenience of continuously wearing the device and carrying the battery pack. One participant expressed a personal concern about the idea of simultaneously receiving chemo and TTFields, while another reported that multiple doctors recommended against going on TTFields because of an existing surgical implant. Additional reasons for not going on TTFields included thinking it would not be needed, that it would not improve quality of life, and that the increased lifespan would not outweigh the negative impact of TTFields. As one participant explained:
Yes, there’s no negative impact, I guess, physically. However, the idea of having something attached to my head and then having to carry around the battery pack doesn’t really mesh well with my relatively physical quality of life…(TTFields) would actually have quite significant negative impacts on how I live my life.
Questions about TTFields
When asked if there was anything about TTFields that was confusing to them, most participants ( N = 33, 85.5%) said no. The aspects of TTFields reported as unclear by seven (17.5%) participants are shown in Table 5 . Participants questions centered around efficacy of the device, how the device works, and what to do if the device gets wet.
Participants views of extension of life from TTFields
We asked participants to describe their understanding of how long TTFields would extend one’s life. Of the 30 participants who answered this question (the question was added to the interview guide after 9 interviews had been completed; one participant chose to skip this question), the most common response was that they did not know how long TTFields extends life ( n = 12, 40.0%). The next most common response was that TTFields extended life several months (e.g., “2–4 months”, “3–6 months”) ( n = 8, 26.6%). Five participants (16.6%) said that they did not have a specific number in mind, but they believed that TTFields extended life. Three participants (10.0%) said TTFields extend life by years (“2 years”, “2–5 years”, “3–14 years”) and two participants (6.6%) provided an answer based on a percentage (e.g., 20–30%, 15–18%); it was unclear what those percentages meant.
Six participants who did not choose TTFields answered the question about extension of life. Of these, 4 (66.6%) said they did not know the extension of life provided by TTFields.
Impact of physician recommendations for TTFields
Among participants who chose TTFields, the majority reported that their clinician recommended TTFields ( n = 25, 78.1%) (Fig. 1 ). The remaining seven (58.3%) participants who chose TTFields said their clinician was neutral towards TTFields. Participants described their physicians’ neutrality as not “pushing” or wanting to “force” a decision on them. According to one participant, “[My doctor] didn’t want to push it, he did say, ‘It’s just another tool in the toolbox,’ and I’m one of these guys who wants to use all the tools.”

Clinician’s Recommendations for TTFields: Patients who Chose TTFields ( N = 32)
For those who did not choose TTFields, 5 (62.5%) reported that their clinician was neutral regarding the patient’s decision, 2 (25.0%) reported that their clinician advised against TTFields, and 1 (12.5%) reported that their clinician recommended TTFields (Fig. 2 ). While the 2 participants whose clinician advised against TTFields did not report their doctor’s opinion as the most influential factor in their decision, one of them stated, “I will use the Optune (TTFields) device if the doctor recommends it.”

Clinician’s Recommendations for TTFields: Patients who did not Choose TTFields ( N = 8)
One participant who did not utilize TTFields described how their clinician presented the information about TTFields:
He had also said it’s the type of thing where you have to really commit to it long-term. And, he also said he likes for his patients to really feel committed to it if they want to do it, just because it’s going to be more effective if you really buy into it. And if I didn’t feel like I was there, then that was okay.
Only one participant went against their doctor’s recommendation by deciding not to undergo TTFields. This participant did not want to wear the TTFields device while working, shave their head, or wear the backpack to carry the device. The most influential factor for this participant, however, was their belief that their cancer would not come back after initial treatment. At the time of the interview, this participant was re-considering TTFields and awaiting the doctor’s recommendation based on pending test results.
Clinician results
Clinician participants ( N = 9) were predominantly male ( n = 6, 66.7%) and included five neuro-oncologists, three advanced practitioners, and a physician assistant. The clinicians had been treating glioblastoma patients for an average of 14 years (range 1–30 years) and saw an average of 38 glioblastoma patients per month (range 17–60 patients). In a typical month, they treated an average of 11 glioblastoma patients with TTFields (range 1–25 patients).
Views of TTFields: benefits and caveats
When asked if they considered TTFields to be a good treatment option for glioblastoma patients, every clinician ( N = 9, 100%) said yes, although their enthusiasm for TTFields varied. Clinicians noted that it was a good option because it has been shown to have an impact, there are few treatment options available, and it is less toxic than other treatment options. Below are example comments from clinicians regarding the benefits of TTFields:
No question (it is a good treatment option). All of the treatment options have somewhat modest efficacy but it’s better than nothing. I will tell them when I start a treatment, when all we had was radiation, I had 90% of my patients dead within less than two years. Now, I have close to 50% of patients doing well at two years. I think that’s pretty straightforward from my perspective. It’s a good treatment because it’s a treatment that’s been shown to improve progression-free survival and improve landmark survival…So, you put those points together and it seems as if it has a real impact. I try not to say in so many words that we don’t have a lot of options for them with this disease and that this is one that we know works for whatever true benefit it provides for each patient, we know that it provides a benefit, and that of the options we have, this is the least-toxic, the one that will be the least likely to cause them any ill effects, will mold into their lifestyles the easiest, and that it does work.
However, some clinicians noted caveats to their endorsement of TTFields. For example, some noted that TTFields is not feasible for certain patients, such as the elderly or patients with poor performance status. This clinician noted the best candidates are patients who have a caregiver to help them with the device or are very functional and motivated to manage the device themselves. Likewise, another clinician emphasized the need for patient motivation to use TTFields:
This (TTFields) is kind of part of you all the time, so I think people just have to kind of accept that. I think the website does a good job of showing people living their normal life with the device, so if people feel like they can be like that, then I think it’s a great treatment, but they have to be willing… and buy into shaving their head, changing the arrays, having the device on 18-plus hours a day, taking it with them when they leave the house, being connected to the plug when they’re at home.
Several clinicians described a neutral approach to advising patients about TTFields. These clinicians said that evaluating whether the burden of TTFields is worth the benefit is the patient’s decision.
I typically frame it in a way where if the patient feels that the burden outweighs the benefit, then they’re the ones in the driver’s seat and they can say, I don’t want to do it because of their perception that this has too much of a negative impact on their quality of life.
One oncologist noted that patients’ views of TTFields are influenced by how clinicians present TTFields:
I think none of us have hesitation presenting to somebody whom we meet who we suspect has a brain tumor that, “You need surgery. There’s no way around this.” Right? And so, we tell them that and we’re comfortable. We have no problem telling them, “You need radiation therapy, or we need to give you this chemotherapy.” But I think culturally, within the neuro-oncology community, there is some hesitancy to say, “Oh, you also need TTFields.” It’s strange to me that that’s the case, because all these other things that are much bigger-gun therapeutics with higher risk profiles, we have no problem recommending.
When asked why clinicians are hesitant to endorse TTFields, this oncologist noted two reasons. First, he noted that changing behavior that is ingrained in one’s work culture is difficult. Second, TTFields is foreign to the oncology world:
Clinician: I think the other aspect that makes tumor treating fields a little bit strange and odd is…it’s coming from the electrical engineering world. And almost none of us have a background in that…. Interviewer: Okay. Do you think physicians are hesitant to use TTFields because they doubt the evidence behind it, or just because it is different? Clinician: I think some people doubt the evidence and I think it’s easier to doubt the evidence when something is different. When you have an outlier idea, the body of proof that you need to and should have to present becomes much higher. So, if you’re presenting a concept that’s not that far removed from everything else that is rapidly accepted as dogma, the burden of proof doesn’t have to be huge… I think there are critics that come at it from the neuro-oncology community that it’s a treatment that didn’t have a sham control, which one could argue we had no problem accepting the lack of blinded study design for temozolomide, which everyone is comfortable administering. So, we have a precedent, but I think people sometimes forget that.
When were asked if they would recommend TTFields for a family member or use it themselves if they had glioblastoma, four of the nine (44%) clinicians said yes, citing reasons such as the minimal risks and the desire to do everything possible to extend their life. Three clinicians (33%) said maybe, noting that it would depend upon whether they would want to go to hospice or obtain treatment, upon the condition of themself or their loved one, and that they probably would not want to be attached to the device but if in that situation they may feel differently. Two clinicians (22%) said no, they would not use TTFields themselves or recommend it for a family member. Of the two who said no, one explained that they would not want to extend life in a compromised state; three months of survival without TTFields vs. 15 months of survival on TTFields was not worth the burden of the device. Similarly, the other physician noted that the added survival does not outweigh the negative quality of life impacts of TTFields.
Discussing survival benefits of TTFields
All clinicians noted that TTFields has a proven benefit for patient lifespan. When asked how they describe the lifespan benefits to patients, clinicians described TTFields benefits in general terms, as evidenced in the quotes below:
(I tell patients) it has sort of become a standard of care for patients after radiation. There’s data that says it improves overall survival and most times it is tolerated pretty well. I don’t (talk to them about benefits to their lifespan), except to say generally that it can add—that really the advantage is that it can buy them some time that is of quality. The problem is that if you talk about time, the time itself isn’t super-significant, in my opinion. And everyone is different. I don’t know what someone’s progression might be with or without Optune (TTFields)… I do tell them that it will add time to their lives, theoretically…but I can’t talk about specific times.
One clinician noted that he tells patients that TTFields can increase two-year survival. However, he felt that discussing months of life extension was not appropriate:
I usually don’t quote months because I think at that moment (the initial meeting) they’re probably too fragile…I rarely quote months at the initial meeting. So, I keep things broader. I don’t say, ‘Well data supports that using this, it improves survival by four months or something.’ I don’t say that.
Another clinician also felt that it would be detrimental to patients to tell them the number of months of extended life provided by TTFields:
It’s tough to do without deflating the patient. And the goal is to infuse the patient with a reasonable hope and not overinflate their expectations. So, keep it reasonable, but at the same time give them things that I feel hopeful about.
Clinicians noted that they typically provided specific data on life extension only if asked. As one clinician noted, “If the patient asks for specific data around the treatment, I’m happy to give that to them. But I tend to avoid talking about statistics.” According to another clinician, “I would say it’s the rare patient who wants a lot more detail than– they usually don’t want to get super-scientific about it.”
This is the first study of views of TTFields among glioblastoma patients and clinicians. Our findings indicate that TTFields is burdensome for patients who use the device, particularly due to changing the arrays and carrying the device. Because there is no cure for glioblastomas, treatment decisions involve prioritizing length of life (LOL) or quality of life (QOL). However, our participants who chose TTFields reported a willingness to accept the burden of TTFields because of its proven efficacy. These results are consistent with the phase three clinical trials of TTFields in which patients receiving TTFields did not report worse social role, social functioning, or physical functioning despite the physical burden of carrying the device and the social impact of the visibility of the device [ 17 ]. Thus, for patients motivated to use this device, the quality of life burden may not be excessive [ 18 ].
Patients who declined TTFields stated that its QOL impacts, such as shaving one’s head or the visibility of TTFields, outweighed the potential LOL benefits. Interestingly, many participants who declined TTFields reported not knowing its impact on survival. It may be that for these patients, no extension of life would outweigh the burden of TTFields. These findings are consistent with observations made by other glioblastoma research: “It appears that, for some, the inconvenience and/or possible stigma associated with the device may be easily mitigated by the potential survival benefit; however, for others, a survival benefit without the promise of a cure may not justify the need for continuous use of the device.” [ 12 ] (p.859).
When presenting TTFields to their glioblastoma patients, clinicians in this sample typically described TTFields’s lifespan advantages in general terms rather than by providing specific prognostic information. Some clinicians noted a desire to balance the fragility of patients diagnosed with a terminal illness with the need to provide information. These findings are consistent with prior work on decision making in advanced cancer wherein clinicians are hesitant to discuss survival and treatment outcomes, [ 19 , 20 , 21 ] physicians make implicit judgements about patients’ desired level of information, [ 22 ] and the central characteristics of shared decision making are often absent [ 23 ]. Although advanced cancer patients, including glioblastoma patients, often report satisfaction with treatment decision making [ 23 ], most patients with incurable cancer want information on life expectancy, including typical, best, and worst case scenarios [ 24 , 25 , 26 , 27 ]. Moreover, awareness of cancer prognosis is linked to improved patient quality of life, goal-concordant care, and lower healthcare costs [ 20 , 28 , 29 ]. Thus, glioblastoma patients may benefit from tools designed to assist them in asking questions about their prognosis [ 30 ].
Patients’ preferred decision-making roles may impact the decision to use TTFields. Patients who declined TTFields were more likely to report a preference for independent decision-making. This preliminary finding should be confirmed in future work with a larger sample of patients. Additionally, these data suggest clinicians could utilize patient decision making preferences to frame the discussion when presenting the TTFields option.
Patients’ TTFields decisions tended to align with their perception of what the physician recommended for them. Clinicians in our sample were generally supportive of using TTFields for glioblastoma patients. The level of support for TTFields among clinicians in this sample is unusual; [ 12 ] future work should consider clinician support of TTFields in other institutions and with larger samples. Our clinician sample noted that TTFields was an appropriate treatment option for glioblastoma because it was shown to be efficacious, there are few treatment options available for glioblastoma, and it is less toxic than other treatment options. While some clinicians enthusiastically endorsed TTFields for their eligible patients, others presented it as an option but noted that they want patients to consider whether the burden of TTFields is worth the benefits of the treatment and emphasized that patients needed to be motivated to commit to using the device.
Our sample consisted primarily of patients who chose to use TTFields. The large number of TTFields users in our sample is due, in part, to the fact that patients interested in trying all forms of treatment often seek out clinicians at the Malnati Brain Tumor Institute. Additionally, patients who declined TTFields may have been in poorer health and deemed ineligible for this study. Additional work is needed to confirm preliminary findings among a sample of patients who decline TTFields. Finally, future work can build upon our findings to develop decision tools for patients and clinicians considering TTFields. These tools should incorporate patients’ desired decision-making role and assess patients’ openness to receiving specific information about survival benefits.
Qualitative research within healthcare aims to uncover meaning, listen to the perspectives of key stakeholders, and build theories [ 31 ]. Without qualitative exploration, subsequent quantitative work may overlook or misrepresent key factors for a particular health problem. We sought to identify factors in the social environment or in patient beliefs that shape TTFields decisions for adult glioblastoma patients.
The decision to use TTFields is a highly personal one for glioblastoma patients. Our findings, which come from the first study of views of TTFields among glioblastoma patients and clinicians, indicate that for some patients who refuse the device, the extension of life gained from using TTFields cannot outweigh the burden of the device. However, the quality-of-life burden of the device may not be excessive for patients who are motivated to use it. Increasing provider support of TTFields may lead to increased use of the device as patients’ TTFields decisions tended to align with their perception of what the physician recommended. Future work should consider the extent to which glioblastoma patients desire more specific prognostic information.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
Tumor Treating Fields
Temozolomide
National Comprehensive Cancer Network
Length of life
Quality of life
Central Brain Tumor Registry of the United States. CBTRUS Statistical Report:Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2004–2008. 2012.
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893–917.
Article CAS PubMed Google Scholar
Stupp R, Roila F, Group EGW. Malignant glioma: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann Oncol. 2009;20(Suppl 4):126–8.
Article PubMed Google Scholar
Novocure O. Elevate Expectations. Available from: https://www.optune.com/ .
Swanson KD, Lok E, Wong ET. An overview of Alternating Electric fields Therapy (NovoTTF Therapy) for the treatment of malignant glioma. Curr Neurol Neurosci Rep. 2016;16(1):8.
Article PubMed PubMed Central Google Scholar
Jain KK. A critical overview of targeted therapies for Glioblastoma. Front Oncol. 2018;8:419.
Oldfield EH, Ram Z, Culver KW, Blaese RM, DeVroom HL, Anderson WF. Gene therapy for the treatment of brain tumors using intra-tumoral transduction with the thymidine kinase gene and intravenous ganciclovir. Hum Gene Ther. 1993;4(1):39–69.
Kanner AA, Wong ET, Villano JL, Ram Z, Investigators EF. Post Hoc analyses of intention-to-treat population in phase III comparison of NovoTTF-100A system versus best physician’s choice chemotherapy. Semin Oncol. 2014;41(Suppl 6):25–34.
Article Google Scholar
Stupp R, Taillibert S, Kanner AA, Kesari S, Steinberg DM, Toms SA, et al. Maintenance Therapy with Tumor-Treating Fields Plus Temozolomide vs Temozolomide alone for Glioblastoma: a Randomized Clinical Trial. JAMA. 2015;314(23):2535–43.
Stupp R, Taillibert S, Kanner A, Read W, Steinberg D, Lhermitte B, et al. Effect of Tumor-Treating Fields Plus maintenance temozolomide vs maintenance temozolomide alone on survival in patients with glioblastoma: a Randomized Clinical Trial. JAMA. 2017;318(23):2306–16.
Article CAS PubMed PubMed Central Google Scholar
U.S, Food. & Drug Administration. NovoTTF™-100L System - H180002 2019. Available from: https://www.fda.gov/medical-devices/recently-approved-devices/novottftm-100l-system-h180002 .
Thomas AA, Rauschkolb PK. Tumor treating fields for glioblastoma: should it or will it ever be adopted? Curr Opin Neurol. 2019;32(6):857–63.
National Comprehensive Cancer Network. NCCN Guidelines: Central Nervous System Cancers 2021. Available from: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1425 .
Degner LF, J. KL DB, et al. Information needs and decisional preferences in women with breast cancer. JAMA. 1997;277(18):1485–92.
Degner LF, Sloan JA. Decision making during serious illness: what role do patients really want to play? J Clin Epidemiol. 1992;45(9):941–50.
Tariman JD, Berry DL, Cochrane B, Doorenbos A, Schepp K. Preferred and actual participation roles during health care decision making in persons with cancer: a systematic review. Ann Oncol. 2010;21(6):1145–51.
Taphoorn MJB, Dirven L, Kanner AA, Lavy-Shahaf G, Weinberg U, Taillibert S, et al. Influence of Treatment with Tumor-Treating fields on Health-related quality of life of patients with newly diagnosed glioblastoma: a secondary analysis of a Randomized Clinical Trial. JAMA Oncol. 2018;4(4):495–504.
Halasz LM, Mitin T. Tumor-treating fields: answering the concern about quality of life. JAMA Oncol. 2018;4(4):504–5.
Audrey S, Abel J, Blazeby JM, Falk S, Campbell R. What oncologists tell patients about survival benefits of palliative chemotherapy and implications for informed consent: qualitative study. BMJ. 2008;337:a752.
Bloom JR, Marshall DC, Rodriguez-Russo C, Martin E, Jones JA, Dharmarajan KV. Prognostic disclosure in oncology - current communication models: a scoping review. BMJ Supportive Palliat Care. 2022;12(2):167.
Liu PH, Landrum MB, Weeks JC, Huskamp HA, Kahn KL, He Y, et al. Physicians’ propensity to discuss prognosis is associated with patients’ awareness of prognosis for metastatic cancers. J Palliat Med. 2014;17(6):673–82.
De Snoo-Trimp JC, Brom L, Pasman HR, Onwuteaka-Philipsen BD, Widdershoven GA. Perspectives of medical specialists on sharing decisions in Cancer Care: a qualitative study concerning chemotherapy decisions with patients with recurrent glioblastoma. Oncologist. 2015;20(10):1182–8.
Brom L, De Snoo-Trimp JC, Onwuteaka-Philipsen BD, Widdershoven GA, Stiggelbout AM, Pasman HR. Challenges in shared decision making in advanced cancer care: a qualitative longitudinal observational and interview study. Health Expect. 2017;20(1):69–84.
Kiely BE, Stockler MR, Tattersall MH. Thinking and talking about life expectancy in incurable cancer. Semin Oncol. 2011;38(3):380–5.
Hagerty RG, Butow PN, Ellis PA, Lobb EA, Pendlebury S, Leighl N, et al. Cancer patient preferences for communication of prognosis in the metastatic setting. J Clin Oncol. 2004;22(9):1721–30.
Greisinger AJ, Lorimor RJ, Aday LA, Winn RJ, Baile WF. Terminally ill cancer patients. Their most important concerns. Cancer Pract. 1997;5(3):147–54.
CAS PubMed Google Scholar
Parker SM, Clayton JM, Hancock K, Walder S, Butow PN, Carrick S, et al. A systematic review of prognostic/end-of-life communication with adults in the advanced stages of a life-limiting illness: patient/caregiver preferences for the content, style, and timing of information. J Pain Symptom Manage. 2007;34(1):81–93.
Epstein AS, Prigerson HG, O’Reilly EM, Maciejewski PK. Discussions of life expectancy and changes in illness understanding in patients with Advanced Cancer. J Clin Oncol. 2016;34(20):2398–403.
Mack JW, Cronin A, Keating NL, Taback N, Huskamp HA, Malin JL, et al. Associations between End-of-life discussion characteristics and Care received Near Death: a prospective cohort study. J Clin Oncol. 2012;30(35):4387–95.
Clayton JM, Butow PN, Tattersall MHN, Devine RJ, Simpson JM, Aggarwal G, et al. Randomized Controlled Trial of a prompt list to help Advanced Cancer patients and their caregivers to ask questions about prognosis and end-of-Life Care. J Clin Oncol. 2007;25(6):715–23.
Renjith V, Yesodharan R, Noronha JA, Ladd E, George A. Qualitative methods in Health Care Research. Int J Prev Med. 2021;12:20.
PubMed PubMed Central Google Scholar
Download references
Acknowledgements
We are grateful to the patients and physicians from the Lou and Jean Malnati Brain Tumor Institute Cancer Institute of Northwestern University who generously gave their time to participate in this study.
Funding was obtained via an investigator-initiated grant funded by Novocure.
Author information
Authors and affiliations.
Department of Neurology, Northwestern University Feinberg School of Medicine, Abbott Hall Suite 1122 710 N Lake Shore Drive, Chicago, IL, 60611, USA
Priya Kumthekar, Rimas V. Lukas, Karan Dixit, Roger Stupp, Jeff Raizer, Margaret Schwartz, Jessica Bajas PA, Ray Lezon & Karyn Schmidt
Lou and Jean Malnati Brain Tumor Institute, Robert H. Lurie Comprehensive Cancer Center of Northwestern University, Chicago, United States
Priya Kumthekar, Rimas V. Lukas, Karan Dixit, Roger Stupp, Jeff Raizer, Sean Sachdev, Margaret Schwartz, Ray Lezon & Christina Amidei
Department of Neurological Surgery, Northwestern University Feinberg School of Medicine, 676 N. St. Clair Street, Suite 2210, Chicago, IL, 60611, USA
Madison Lyleroehr & Karen Kaiser
Department of Radiation Oncology, Northwestern University Feinberg School of Medicine, 676 N. St. Clair Street, Suite 1820, Chicago, IL, 60611, USA
Christina Amidei
Northwestern University Feinberg School of Medicine, 420 E. Superior St, Chicago, IL, 60611, USA
Sean Sachdev
Department of Human Oncology, University of Wisconsin Carbone Cancer Center, 600 Highland Ave, Madison, WI, 53705, USA
Alexander Hou
Equal Hope, 300 South Ashland Avenue, Chicago, IL, 60607, USA
Leilani Lacson & Timothy Kruser
You can also search for this author in PubMed Google Scholar
Contributions
PK was instrumental to the project and was involved in all aspects: designing the project, drafting the manuscript, acquisition/patient accrual and analysis and interpretation of data. ML analyzed and interpreted patient interview data and wrote parts of the manuscript. LL conducted execution of the study and analysis of the data. RVL, KD, RS, JR, SS, MS, JB, RL, KS all supported the acquisition of data through patient accrual. TK, AH, and CA contributed to the study design while CA was also involved in data acquisition. KK was involved in the study design, acquisition, analysis and interpretation of data, and drafting the manuscript.
Corresponding author
Correspondence to Karen Kaiser .
Ethics declarations
Ethics approval and consent to participate.
The study protocol was approved by the institutional review board of Northwestern University (STU00210799) and all patients enrolled on study provided written informed consent prior to any study-related procedures.
Consent for publication
Not applicable.
Competing interests
PK has received research and grant support from Genentech, Novocure, DNAtrix and Orbus Therapeutics. PK has served on medical advisory boards for Biocept, Sintetica, Novocure, Janssen, Affinia, Celularity, and SDP Oncology. PK has provided consulting to Bliss Bio, Biocept, Enclear Therapies, Angiochem, Affinia Therapeutics. TK serves on an advisory board and speakers bureau for AstraZeneca, and a consultant for Radialogica LLC, none of which relate to this work. MS is in the Novocure speakers bureau. RVL serves on the speakers’ bureaus for Novocure and Merck. RVL has received research support (drug only) from BMS. RVL has received honoraria for medical editing for EBSCO Publishing, and Medlink Neurology. RVL also serves on advisory boards for Novocure, AstraZeneca, Cardinal Health, Servier, and Merck. SS has served on advisory boards for Lantheus, Astellas, and Pfizer. KK has served as a consultant for PTC Therapeutics. All other authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Kumthekar, P., Lyleroehr, M., Lacson, L. et al. A qualitative evaluation of factors influencing Tumor Treating fields (TTFields) therapy decision making among brain tumor patients and physicians. BMC Cancer 24 , 527 (2024). https://doi.org/10.1186/s12885-024-12042-x
Download citation
Received : 29 September 2023
Accepted : 22 February 2024
Published : 25 April 2024
DOI : https://doi.org/10.1186/s12885-024-12042-x
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Glioblastoma
- Tumor treating fields
- Decision-making
ISSN: 1471-2407
- Submission enquiries: [email protected]
- General enquiries: [email protected]
Factbox-Key Quotes From Trump's Criminal Hush Money Trial
Factbox-Key Quotes From Trump's Criminal Hush Money Trial

FILE PHOTO: Former U.S. President Donald Trump sits as final jurors are sworn in during his criminal trial on charges that he falsified business records to conceal money paid to silence porn star Stormy Daniels in 2016, in Manhattan state court in New York City, U.S. April 19, 2024 in this courtroom sketch. REUTERS/Jane Rosenberg/Pool/File Photo
By Luc Cohen and Jack Queen
NEW YORK (Reuters) - Opening statements kicked off on Monday in the criminal hush money trial of Donald Trump and the first prosecution witness, the former publisher of the National Enquirer, took the stand. Trump has pleaded not guilty to falsifying business records to cover up a hush money payment made by Trump's former lawyer Michael Cohen to porn star Stormy Daniels ahead of the 2016 election.
Here are some key quotes from the proceedings:
-"This case is about a conspiracy and a cover-up, an illegal conspiracy to undermine the integrity of a presidential election, and then the steps that Donald Trump took to conceal that illegal election fraud,” prosecutor Matthew Colangelo told the jury during his opening statement.
-“No politician wants bad press, but the evidence at trial will show that this was not spin or communications strategy. This was a planned, coordinated, long-running conspiracy to influence the 2016 election, to help Donald Trump get elected through illegal expenditures to silence people who had something bad to say about his behavior,” Colangelo said. “It was election fraud, pure and simple.”
“The defendant disguised his reimbursements to Michael Cohen through 11 falsified invoices, 12 falsified ledger entries, and 11 falsified checks,” Colangelo said.
Colangelo also described an alleged scheme to “catch and kill” Playboy model Karen McDougal’s story of a months-long affair she says she had with Trump, which is not a formal part of the indictment.
“The evidence will show that the defendant desperately did not want this info about Karen McDougal to become public because he was worried about its impact on the election,” Colangelo said.
Trump has denied the affair.
-Trump lawyer Todd Blanche countered that Trump, whom he referred to as President Trump, is innocent.
"President Trump did not commit any crimes. The Manhattan District Attorney’s office should never have brought this case,” Trump lawyer Todd Blanche told the jury during his opening statement.
-"There’s nothing wrong with trying to influence an election. It’s called democracy. They put something sinister on this idea, as if it’s a crime,” Blanche said.
-Blanche said that despite Trump’s celebrity and stature as a former president, he is also a husband and father.
“He is in some ways larger than life, but he’s also here in this courtroom doing what any of us would do: defending himself,” Blanche said.
"President Trump fought back like he always does and like he’s entitled to do to protect his family, his reputation and his brand - and that is not a crime,” Blanche told the jury.
-Blanche asserted that Stormy Daniels is lying about the former president for financial gain.
“She saw her chance to make a lot of money, and it worked,” Blanche said, referring to the hush money payout.
He also said Cohen was not trustworthy.
-"He has a goal - an obsession - with getting Trump,” Blanche said of Cohen, adding that he had lied under oath during previous testimony in other cases. “I submit to you that he cannot be trusted.”
-David Pecker, the former publisher of the National Enquirer and the first prosecution witness to take the stand said he had the final say over publishing decisions.
"Yes. I had the final say on the celebrity side of the magazine industry, at least on the tabloid side. We used checkbook journalism and we paid for stories," he said.
(Reporting by Luc Cohen and Jack Queen; Writing by Noeleen Walder; Editing by Nick Zieminski)
Copyright 2024 Thomson Reuters .
Join the Conversation
Tags: United States , crime , New York
America 2024

Health News Bulletin
Stay informed on the latest news on health and COVID-19 from the editors at U.S. News & World Report.
Sign in to manage your newsletters »
Sign up to receive the latest updates from U.S News & World Report and our trusted partners and sponsors. By clicking submit, you are agreeing to our Terms and Conditions & Privacy Policy .
You May Also Like
The 10 worst presidents.
U.S. News Staff Feb. 23, 2024

Cartoons on President Donald Trump
Feb. 1, 2017, at 1:24 p.m.

Photos: Obama Behind the Scenes
April 8, 2022

Photos: Who Supports Joe Biden?
March 11, 2020

The Status of the Cases Against Trump
Lauren Camera and Kaia Hubbard April 25, 2024

Economy Slows in First Quarter
Tim Smart April 25, 2024

A ‘Fork in the Road’ for Democracy
Lauren Camera April 24, 2024

Johnson at Columbia: ’Stop the Nonsense’
Aneeta Mathur-Ashton April 24, 2024

What to Know: Bird Flu Virus in Milk
Cecelia Smith-Schoenwalder April 24, 2024

High Court to Again Weigh Abortion Law
Laura Mannweiler April 23, 2024

IMAGES
VIDEO
COMMENTS
Beyond the default colon: Effective use of quotes in qualitative research. In the Writer's Craft section we offer simple tips to improve your writing in one of three areas: Energy, Clarity and Persuasiveness. Each entry focuses on a key writing feature or strategy, illustrates how it commonly goes wrong, teaches the grammatical underpinnings ...
While the terms "quotations" and "quotes" are sometimes used as synonyms, they originally represent a noun and a verb, respectively. Further, both terms have several connotations, but, as applied in qualitative research, the term "quotation" generally signifies "passages reproduced or repeated," whereas it can also indicate the act of quoting—that is, "to quote," which ...
Abstract. For qualitative researchers, quotes are the heart of the results section. However, they are evidence, not argument. They do not speak for themselves and readers cannot infer what you intend them to illustrate. Using two principles, this chapter offers suggestions to help you choose the right quotes and integrate them with coherence ...
6.1 Authenticity. At the point of manuscript writing, a qualitative researcher is swimming in sea of data. Innumerable transcript excerpts have been copied and pasted into data analysis software or (for the more tactile among us) onto multi-colored sticky notes. Some of these excerpts we like very much.
Smith, 2015, p. 35). According to Patton (2002), verbatim quo-. tations are synonymous with direct quotations, which are a. basic source of raw data in qualitative research that serve to. reveal ...
Kevin W. Rockmann is a Professor of Management at the Donald G. Costello College of Business at George Mason University, where his research involves studying working relationships in organizations, including how relationships are generated, maintained, and dissolve. He has used qualitative methods to study these questions across a variety of contexts including hospitals, gig workers, remote ...
The use of quotes in qualitative research. Dr. Margarete Sandelowski PhD, RN, FAAN, Corresponding Author. Dr. Margarete Sandelowski PhD, RN, FAAN. Professor. ... Quoted words and phrases from research participants are a common feature of qualitative research reports. Quoting is a process that requires the achievement of the proper balance ...
The use of quotes in qualitative research. Dr. Margarete Sandelowski PhD, RN, FAAN, Corresponding Author. Dr. Margarete Sandelowski PhD, RN, FAAN. Professor. ... Quoted words and phrases from research participants are a common feature of qualitative research reports. Quoting is a process that requires the achievement of the proper balance ...
It is common in qualitative research for investigators to share only a few exemplifying quotes from a much larger body of data in an effort to give an authentic voice to the larger group of ...
Introduction. This paper presents findings from one component of an ESRC funded research study of the theory, practice and impact of using verbatim quotations from research participants in reporting qualitative social research for policy. The study was conducted by the authors during 2003-05.
The use of quotes or verbatims from participants is a typical and necessary component to any qualitative research report. It is by revealing participants' exact language that the researcher helps the user of the research to understand the key takeaways by clarifying through illustration the essential points of the researcher's interpretations. . The idea is not to display an extensive list ...
Abstract. For qualitative researchers, quotes are the heart of the results section. However, they are evidence, not argument. They do not speak for themselves and readers cannot infer what you ...
The proliferation of respondent quotes used as research titles in peer reviewed journals. This article has been inspired by the authors' recognition that the use of respondent quotes as research titles appears to have become standard practice within a wide range of social science/health-focused journals that are sympathetic toward publishing qualitative research articles.
Qualitative research was historically employed in fields such as sociology, history, ... Data consists of verbatim quotations and sufficient content/context to be interpretable". Researchers may use a structured or unstructured interview approach. Structured interviews rely upon a predetermined list of questions framed algorithmically to ...
Often, new qualitative researchers will too liberally use block quotations. In other words, a key phrase or sentence may be all they really want to convey but they include a paragraph to "provide context.". Avoid this trap. If you need to provide context for a quote, then put this in your own words rather than in the participants.
Quoted words and phrases from research participants are a common feature of qualitative research reports and involve researchers in acts of choosing that lie in the domains of aesthetics and ethics. Quoted words and phrases from research participants are a common feature of qualitative research reports. Quoting is a process that requires the achievement of the proper balance between the ...
when an author has said something memorably or succinctly, or. when you want to respond to exact wording (e.g., something someone said). Instructors, programs, editors, and publishers may establish limits on the use of direct quotations. Consult your instructor or editor if you are concerned that you may have too much quoted material in your paper.
This is a nice example of how 'Tab. 1', conventionally used in quantitative research papers for demographic details of the research sample, can be re-conceptualized to feature the key findings from a qualitative analysis. Tables should be supplemented, however, with narrative explanation in which the writer contextualizes and interprets the ...
When quoting research participants, abide by any ethical agreements regarding confidentiality and/or anonymity agreed to between you and your participants during the consent or assent process. Take care to obtain and respect participants' consent to have their information included in your report. To disguise participant information, you may ...
Conclusions. Today, a variety of ways to use quotations is observed in the practices of reporting qualitative research. Quotations are see-mingly applied for several purposes: as evidence, explanation, illustration, impression, representation, and/or to enhance readability.
17. "The power of statistics and the clean lines of quantitative research appealed to me, but I fell in love with the richness and depth of qualitative research." - Brené Brown. Brown is a researcher and storyteller studying courage, shame, empathy and vulnerability. She is a best-selling author and inspirational speaker.
Quotes tagged as "qualitative-research" Showing 1-8 of 8. "I want to understand the world from your point of view. I want to know what you know in the way you know it. I want to understand the meaning of your experience, to walk in your shoes, to feel things as you feel them, to explain things as you explain them.
Background Tumor Treating Fields (TTFields) Therapy is an FDA-approved therapy in the first line and recurrent setting for glioblastoma. Despite Phase 3 evidence showing improved survival with TTFields, it is not uniformly utilized. We aimed to examine patient and clinician views of TTFields and factors shaping utilization of TTFields through a unique research partnership with medical neuro ...
US News is a recognized leader in college, grad school, hospital, mutual fund, and car rankings. Track elected officials, research health conditions, and find news you can use in politics ...