Home > AACR Cancer Progress Report > AACR Cancer Progress Report 2022: Contents > Cancer in 2022

Cancer in 2022
In this section, you will learn:
- In the United States, the age-adjusted overall cancer death rate has been steadily declining since the 1990s, with the reductions between 1991 and 2019 translating into nearly 3.5 million cancer deaths avoided.
- In the past three years, the number of cancer survivors living in the United States increased by more than a million, reaching greater than 18 million as of January 1, 2022.
- Certain U.S. populations have not benefited equally from the advances against cancer.
- The personal burden of cancer and its economic toll both on individuals and the U.S. health care system are expected to rise in the coming decades, highlighting the urgent need for more research to accelerate the pace of progress against cancer.
Research: Driving Progress Against Cancer
Cancer: an ongoing public health challenge in the united states and worldwide, variable progress among stages at diagnosis and types of cancer, disparities in progress for certain population groups, the growing burden of cancer, the global challenge of cancer, funding cancer research: a vital investment.

Medical research is the foundation of progress against the collection of many diseases we call cancer. Research improves survival and quality of life for people around the world because it is the driving force behind every advance in cancer science and medicine and every legislative action designed to improve public health. Each breakthrough against cancer is the culmination of a complex, multifaceted process that takes long-term commitment and years of effort by individuals from all segments of the medical research community (see sidebar on The Medical Research Community: Driving Progress Together ).
The remarkable progress being made against cancers—in particular, improvements in reducing smoking rates and developments in early detection and treatment—is resulting in cancer death rates falling steadily and in a rising number of people who survive a cancer diagnosis. In fact, the age-adjusted overall cancer death rate has declined by 32 percent between 1991 and 2019 in the United States, a reduction that translates into nearly 3.5 million cancer deaths avoided ( 1 ) Siegel RL, et al. Cancer statistics, 2022. CA Cancer J Clin 2022;72:7-33. [LINK NOT AVAILABLE] . Among children and adolescents with cancer, overall death rates have declined by more than half between 1970 and 2019, largely due to advances in treatment ( 1 ) Siegel RL, et al. Cancer statistics, 2022. CA Cancer J Clin 2022;72:7-33. [LINK NOT AVAILABLE] . In addition, in the past three years, the number of adults and children living in the United States with a history of cancer rose by more than a million, exceeding an estimated 18 million on January 1, 2022 ( 2 ) Miller KD, et al. Cancer Treatment and Survivorship Statistics, 2022. CA Cancer J Clin 2022;0:1-28. [LINK NOT AVAILABLE] .

The steady decline in the overall cancer death rate can be attributed mainly to the unprecedented progress against lung, colorectal, breast, and prostate cancer, the four most common cancer types in the United States. In fact, during the past three decades, age-adjusted death rates from lung, female breast, and colorectal cancers have decreased by 44, 42, and 53 percent, respectively ( 3 ) Kratzer TB, et al. Progress against cancer mortality 50 years after passage of the National Cancer Act. JAMA Oncol 2022;8:156-9. [LINK NOT AVAILABLE] . Furthermore, there have been significant developments against previously intractable cancers, such as melanoma, the deadliest form of skin cancer, fueled by a range of innovative new therapeutics that have moved rapidly from the bench to the clinic and received approval by the U.S. Food and Drug Administration (FDA) (see Figure 1 ). Collectively, these advances have led to the increase in five-year relative survival rate for all cancers combined from 49 percent in the mid-1970s to nearly 70 percent from 2011 to 2017, which are the most recent data available ( 1 ) Siegel RL, et al. Cancer statistics, 2022. CA Cancer J Clin 2022;72:7-33. [LINK NOT AVAILABLE] .
Among the major advances made across the clinical cancer care continuum from August 1, 2021, to July 31, 2022, are the eight new anticancer therapeutics approved for use by FDA (see Table 4 ). During this period, FDA also approved two new imaging agents to help visualize cancerous cells, several artificial intelligence-based tools to improve detection and diagnosis of cancers, and new uses for 10 previously approved anticancer therapeutics.
The research that drives progress against cancer is made possible by investments from governments, philanthropic individuals and organizations, and the private sector. In the United States, government investments in medical research are administered mostly through the 27 institutes and centers of the National Institutes of Health (NIH). The largest component of NIH is the National Cancer Institute (NCI), which is the federal government’s principal agency for cancer research and training. Medical research funded by the public sector contributes significantly to novel drug development, which is critical to saving and improving lives ( 6 ) Nayak RK, et al. Public-sector contributions to novel biologic drugs. JAMA Intern Med 2021;181:1522-5. [LINK NOT AVAILABLE] ( 7 ) Galkina Cleary E, et al. Contribution of NIH funding to new drug approvals 2010-2016. Proc Natl Acad Sci U S A 2018;115:2329-34. [LINK NOT AVAILABLE] . Federal investments in government agencies conducting research, such as FDA and the Centers for Disease Control and Prevention (CDC), are also of particular importance.
Although we have made incredible progress against cancers, this group of devastating diseases continues to be an enormous public health challenge in the United States and around the world. In the United States alone, it is predicted that 1,918,030 new cases of cancer will be diagnosed in 2022 and that 609,360 people will die from the disease ( 1 ) Siegel RL, et al. Cancer statistics, 2022. CA Cancer J Clin 2022;72:7-33. [LINK NOT AVAILABLE] (see Table 1 ). These estimates do not account for the consequences of COVID-19, which has proven to have an adverse impact across the spectrum of cancer research and patient care including significant declines in cancer screening and diagnosis ( 8 ) American Association for Cancer Research. AACR Report on the Impact of COVID-19 on Cancer Research and Patient Care. Accessed: June 30, 2022.[cited 2020 Jul 15]. . In addition, data from the past two years have clearly shown the heightened risks of SARS-CoV-2 infection and severe COVID-19 among patients with cancer, albeit COVID-19-related mortality among this population has decreased over time ( 8 ) American Association for Cancer Research. AACR Report on the Impact of COVID-19 on Cancer Research and Patient Care. Accessed: June 30, 2022.[cited 2020 Jul 15]. ( 9 ) Dieci MV, et al. Clinical profile and mortality of Sars-Cov-2 infection in cancer patients across two pandemic time periods (Feb 2020-Sep 2020; Sep 2020-May 2021) in the Veneto Oncology Network: The ROVID study. Eur J Cancer 2022;167:81-91. [LINK NOT AVAILABLE] . Ongoing research will uncover the long-term effects of COVID-19 on cancer outcomes ( 10 ) National Cancer Institute. NCI COVID-19 in Cancer Patients Study (NCCAPS). Accessed: Nov 27, 2021.[cited 2020 Jul 15]. .

Progress against cancers has not been uniform for all stages of a given type of disease ( 5 ) National Cancer Institute. Surveillance, Epidemiology, and End Results program explorer. Accessed: June 30, 2022.[cited 2020 Jul 15]. . This issue is illustrated by the fact that the five-year relative survival rates for U.S. patients vary widely depending on the stage at diagnosis ( 5 ) National Cancer Institute. Surveillance, Epidemiology, and End Results program explorer. Accessed: June 30, 2022.[cited 2020 Jul 15]. . As one example, among women with breast cancer and people with colorectal cancer, those whose cancer is confined to the breast, or to the colon or rectum, have five-year relative survival rates of 99 percent and 92 percent, respectively, while those whose cancer has spread to a distant site have five-year relative survival rates of 30 percent and 16 percent, respectively ( 5 ) National Cancer Institute. Surveillance, Epidemiology, and End Results program explorer. Accessed: June 30, 2022.[cited 2020 Jul 15]. .

An additional challenge that we face is the uneven progress against various cancer types ( 5 ) National Cancer Institute. Surveillance, Epidemiology, and End Results program explorer. Accessed: June 30, 2022.[cited 2020 Jul 15]. . For example, the overall five-year relative survival rates of nearly 91 percent for women with breast cancer and 97 percent for men with prostate cancer stand in stark contrast to the overall five-year relative survival rates of 21 percent for people with liver cancer and less than 12 percent for those with pancreatic cancer ( 5 ) National Cancer Institute. Surveillance, Epidemiology, and End Results program explorer. Accessed: June 30, 2022.[cited 2020 Jul 15]. . While some of these differences could be attributed to early detection of breast and prostate cancers through population level screening (see sidebar on Ways to Screen for Cancer ), disparities in five-year relative survival rates hold true for patients with these four cancer types even when their diseases are diagnosed at an advanced stage. The five-year relative survival rates of greater than 30 percent for advanced-stage female breast and male prostate cancers are significantly higher than the five-year relative survival rates of less than five percent for those with advanced-stage liver or pancreatic cancer ( 5 ) National Cancer Institute. Surveillance, Epidemiology, and End Results program explorer. Accessed: June 30, 2022.[cited 2020 Jul 15]. .
Among children ages one to 14 years, cancer is the second-leading cause of death, and the most diagnosed cancers are leukemia and brain tumors ( 1 ) Siegel RL, et al. Cancer statistics, 2022. CA Cancer J Clin 2022;72:7-33. [LINK NOT AVAILABLE] . Thanks to extraordinary advances in treatments for childhood leukemia, the age-adjusted mortality rate from the disease has almost halved in the past two decades. Unfortunately, mortality rates from childhood brain and other central nervous system tumors have essentially remained unchanged ( 5 ) National Cancer Institute. Surveillance, Epidemiology, and End Results program explorer. Accessed: June 30, 2022.[cited 2020 Jul 15]. .
Developing new and effective tests for early detection of more types of cancer as well as better treatment options for all cancer types and for all stages of diagnosis could help address the challenges of variable progress against different types of cancer.

Cancer health disparities are one of the most pressing public health challenges in the United States. NCI defines cancer health disparities as adverse differences in cancer such as number of new cases, number of deaths, cancer-related health complications, survivorship and quality of life after cancer treatment, screening rates, and stage at diagnosis that exist among certain population groups ( 12 ) Cancer health disparities definitions and examples. Accessed: April 22, 2022.[cited 2020 Jul 15]. (see sidebar on Which U.S. Population Groups Experience Cancer Health Disparities? ).
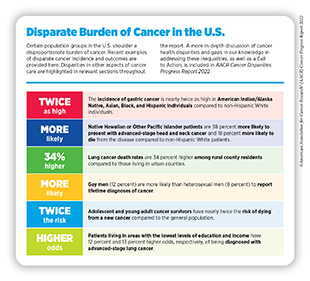
As outlined in the AACR Cancer Disparities Progress Report 2022, racial and ethnic minorities and other medically underserved U.S. populations shoulder a disproportionately higher burden of cancer (see sidebar on Disparate Burden of Cancer in the U.S. ) ( 13 ) American Association for Cancer Research. AACR Cancer Disparities Progress Report 2022. Accessed: June 30, 2022.[cited 2020 Jul 15]. . As one example, the U.S. Black population has long experienced cancer health disparities.
In 1990, the overall cancer death rates for Black people were 33 percent higher than for White people ( 5 ) National Cancer Institute. Surveillance, Epidemiology, and End Results program explorer. Accessed: June 30, 2022.[cited 2020 Jul 15]. . There has been some progress in recent years as evidenced by the narrowing of the gap in cancer death rates between the Black and White populations to 13 percent in 2019, a 60 percent decline in the disparities since 1990 ( 5 ) National Cancer Institute. Surveillance, Epidemiology, and End Results program explorer. Accessed: June 30, 2022.[cited 2020 Jul 15]. ( 14 ) Lawrence WR, et al. Trends in cancer mortality among black individuals in the US from 1999 to 2019. JAMA Oncol 2022. [LINK NOT AVAILABLE] . However, even in 2019, overall cancer death rates were higher among Black men and women compared to all other U.S. racial and ethnic groups ( 14 ) Lawrence WR, et al. Trends in cancer mortality among black individuals in the US from 1999 to 2019. JAMA Oncol 2022. [LINK NOT AVAILABLE] .
Sexual and gender minorities (SGM) are another U.S. population that experiences cancer health disparities. According to a new report, gay men are more likely than heterosexual men to report lifetime diagnoses of cancers, and gay men and lesbian women are more frequently unable to afford many types of health care services compared to heterosexual men and women ( 15 ) Heslin KC, et al. Sexual orientation differences in access to care and health status, behaviors, and beliefs: Findings from the National Health and Nutrition Examination Survey, National Survey of Family Growth, and National Health Interview Survey. Natl Health Stat Report 2022:1-16. [LINK NOT AVAILABLE] . Unfortunately, there are limited data on the epidemiology of cancer incidence and outcomes among SGM individuals making it difficult to evaluate the true burden of cancer in this underserved population. It is imperative that researchers collect disaggregated data by sexual orientation and gender identity, as well as within sexual minority groups (e.g., gay versus bisexual) and gender minority groups (e.g., transgender versus nonbinary) to accurately capture cancer epidemiology in these heterogeneous populations ( 13 ) American Association for Cancer Research. AACR Cancer Disparities Progress Report 2022. Accessed: June 30, 2022.[cited 2020 Jul 15]. .
Research has identified complex and interrelated factors, often referred to as the social determinants of health, including socioeconomic, cultural, behavioral, environmental, and clinical factors that contribute to cancer health disparities. It is increasingly evident that structural racism and systemic injustices cause adverse differences in social determinants of health, creating conditions that perpetuate health inequities, including cancer health disparities (see sidebar on Why Do U.S. Cancer Health Disparities Exist? ).

One of the drivers of cancer health disparities is general health of a population group. For instance, individuals with underlying health conditions, such as diabetes, or those infected with certain pathogens, such as human immunodeficiency virus (HIV), experience a greater burden of cancer (see sidebar on Cancer Burden Among People Living with HIV ). It should be noted that individuals with intersectional identities often experience multilevel barriers to optimal health care that adversely impact cancer incidence and outcomes. As one example, among individuals living with HIV, those who are from racial and ethnical minority populations may experience worse cancer health disparities ( 20 ) Elizabeth Read-Connole, et al. Basic/Translational research on Health Disparities in HIV/AIDS and cancer (Clinical trial optional). 2022. [LINK NOT AVAILABLE] . Understanding the biological drivers of cancer health disparities in marginalized populations with an underlying HIV/AIDS diagnosis is an area of active investigation ( 20 ) Elizabeth Read-Connole, et al. Basic/Translational research on Health Disparities in HIV/AIDS and cancer (Clinical trial optional). 2022. [LINK NOT AVAILABLE] .

Considering that a significant proportion of the U.S. population is affected by cancer health disparities, it is important that public health experts intensify research efforts designed to improve our understanding and mitigating of these disparities. Only with new insights obtained through innovative research, including basic science using biospecimens from diverse populations, clinical trials involving participants from all sociodemographic backgrounds, and health care delivery research, will we develop and implement interventions that may eventually eliminate cancers for all populations.
The public health challenge posed by cancer is predicted to grow considerably in the coming decades unless we develop and implement more effective strategies for cancer prevention, early detection, and treatment ( 26 ) International Agency for Research on Cancer. Global Cancer Observatory. Accessed: July 15, 2022.[cited 2020 Jul 15]. . In the United States alone, the number of new cancer cases diagnosed each year is expected to reach nearly 2.3 million by 2040 ( 26 ) International Agency for Research on Cancer. Global Cancer Observatory. Accessed: July 15, 2022.[cited 2020 Jul 15]. . This is largely because cancer is primarily a disease of aging; 80 percent of U.S. cancer diagnoses occur among those who are 55 or older; 57 percent of diagnoses occur among those 65 and older ( 1 ) Siegel RL, et al. Cancer statistics, 2022. CA Cancer J Clin 2022;72:7-33. [LINK NOT AVAILABLE] , and this segment of the U.S. population is expected to grow from 54.1 million in 2019 to nearly 81 million in 2040 ( 27 ) U.S. Department of Health and Human Services. Administration for Community Living. 2020 Profile of Older Americans. Accessed: Jul 6, 2022.[cited 2020 Jul 15]. . Also contributing to the projected increase in the number of U.S. cancer cases are high rates of obesity and physical inactivity, which are both linked to some common types of cancer, and the continued use of tobacco products among certain U.S. populations.

Progress has been made toward reducing cancer incidence in the United States; new cancer cases have declined 10 percent from their peak in 1992 to 2019, the year for which the most recent data are reported ( 5 ) National Cancer Institute. Surveillance, Epidemiology, and End Results program explorer. Accessed: June 30, 2022.[cited 2020 Jul 15]. . However, overall cancer incidence has been rising among the U.S. adolescent and young adult (AYA) population (ages 15 to 39), which has seen nearly a 20 percent increase in cancer incidence from 2000 to 2019 ( 5 ) National Cancer Institute. Surveillance, Epidemiology, and End Results program explorer. Accessed: June 30, 2022.[cited 2020 Jul 15]. . In addition, the incidence of certain cancer types is steadily increasing, specifically among people younger than 50. As one example, many recent studies have reported an increase in the incidence of early-onset colorectal cancer among those age 49 and younger ( 28 ) Sinicrope FA. Increasing incidence of early-onset colorectal cancer. N Engl J Med 2022;386:1547-58. [LINK NOT AVAILABLE] ( 29 ) Calip GS, et al. Colorectal cancer incidence among adults younger than 50 years-understanding findings from observational studies of lower gastrointestinal endoscopy. JAMA Oncol 2022;8:981-3. [LINK NOT AVAILABLE] . The reasons behind rising cases of early-onset colorectal cancers are not completely understood but is presumed to be multifactorial, including contributions of modifiable lifestyle factors such as unhealthy diet and physical inactivity as well as factors that alter the gut microbiome such as use of antibiotics. To reduce the burden of early-onset colorectal cancer, many professional societies have modified their screening guidelines to recommend starting colorectal cancer screening at an earlier age. Additionally, researchers are evaluating new and improved strategies including genetic testing and others for prevention and early detection of colorectal cancer in the younger population ( 28 ) Sinicrope FA. Increasing incidence of early-onset colorectal cancer. N Engl J Med 2022;386:1547-58. [LINK NOT AVAILABLE] .

Beyond the United States, cancer is an ongoing global challenge (see sidebar on Global Burden of Cancer ). According to a new analysis, there were an estimated 17.2 million new cancer cases (excluding nonmelanoma skin cancer) and 10 million cancer deaths globally, in 2019 ( 30 ) Kocarnik JM, et al. Cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life years for 29 cancer groups from 2010 to 2019: A systematic analysis for the global burden of disease study 2019. JAMA Oncol 2022;8:420-44. [LINK NOT AVAILABLE] . The study evaluated cancer burden from 204 countries and territories as indicated by cancer-related deaths, as well as disability-adjusted life years (DALYs) and years of life lost (YLLs), which are two measures of cancer morbidity. Researchers found that among the 22 groups of diseases and injuries analyzed, cancer was second only to cardiovascular disease in the number of deaths, DALYs, and YLLs ( 30 ) Kocarnik JM, et al. Cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life years for 29 cancer groups from 2010 to 2019: A systematic analysis for the global burden of disease study 2019. JAMA Oncol 2022;8:420-44. [LINK NOT AVAILABLE] . The five leading causes of cancer-related morbidity among men and women combined were lung cancer, colorectal cancer, stomach cancer, breast cancer, and liver cancer.
The study also indicated that, although there were increases in the absolute numbers of both global cancer deaths and new cases from 2010 to 2019, the age-standardized mortality and incidence rates decreased by six percent and one percent, respectively ( 30 ) Kocarnik JM, et al. Cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life years for 29 cancer groups from 2010 to 2019: A systematic analysis for the global burden of disease study 2019. JAMA Oncol 2022;8:420-44. [LINK NOT AVAILABLE] . These trends, however, precede the setbacks in cancer care and outcomes that have been caused by the COVID-19 pandemic. Global health experts are also concerned about the consequences of the ongoing wars that have displaced populations, further destroying health care systems, disrupting social services, and increasing risk of infectious disease transmission ( 31 ) The ASCO Post Staff. War is hell. It’s also a public health disaster, especially for people with cancer. Accessed: July 6, 2022.[cited 2020 Jul 15]. . Considering the devastating impact of these global crises on the entire continuum of cancer research and patient care as well as the growth of the global population age 65 and older ( 32 ) United Nations. Ageing. Accessed: July 6, 2022.[cited 2020 Jul 15]. , researchers caution that the burden of cancer worldwide may rise significantly in the coming decades.
Another concern among global public health experts is that, while age-standardized mortality and incidence rates are declining overall, the reduction in rates appears to be driven by countries with a higher sociodemographic index (SDI)—a composite measure of the social and economic development of a country that considers income per capita, average years of education, and total fertility rate for people younger than 25. The data indicate that age-standardized cancer incidence and mortality rates are increasing in countries with lower SDI ( 33 ) Pramesh CS, et al. Priorities for cancer research in low- and middle-income countries: a global perspective. Nat Med 2022;28:649-57. [LINK NOT AVAILABLE] .
To ensure that progress against cancer is equitable worldwide, it is imperative that the global medical research community work together and share best practices to implement newer and more effective strategies that incorporate local needs and knowledge into tailored national cancer control plans. Public health experts have identified several priorities based on present and future needs of low resource countries, including reducing the burden of advanced cancers; improving access, affordability, and outcomes of treatment, utilizing value-based care; fostering implementation research; and leveraging technology to improve cancer control ( 33 ) Pramesh CS, et al. Priorities for cancer research in low- and middle-income countries: a global perspective. Nat Med 2022;28:649-57. [LINK NOT AVAILABLE] .
Cancer exerts an immense toll because of the number of lives it affects each year and through its significant economic impact. The direct medical costs of cancer care are one measure of the financial impact of cancer, and in the United States alone, they were estimated to be $183 billion in 2015, the last year for which these data are currently available; this cost is projected to increase to $246 billion by 2030 ( 1 ) Siegel RL, et al. Cancer statistics, 2022. CA Cancer J Clin 2022;72:7-33. [LINK NOT AVAILABLE] . These numbers do not include the indirect costs of lost productivity due to cancer-related morbidity and mortality, which are also extremely high. Notably, cancer patients in the United States shouldered an economic burden of $21 billion in 2019 from out-of-pocket costs and other related expenses, which is nearly 3.5 times the amount of approximately $6 billion in NCI funding for cancer research in the same year ( 38 ) Yabroff KR, et al. Annual Report to the Nation on the Status of Cancer, part 2: Patient economic burden associated with cancer care. J Natl Cancer Inst 2021;113:1670-82. [LINK NOT AVAILABLE] .

With the number of cancer cases projected to increase in the coming decades, we can be certain that both the direct and indirect costs will also escalate. The rising personal and economic burden of cancer underscores the urgent need for more research so that we can accelerate the pace of progress against cancer.
Recent advances in cancer prevention, detection, and treatment, many of which are highlighted in this report, were made as a direct result of the cumulative efforts of researchers from across the spectrum of cancer science and medicine. Much of their work, as well as that of FDA—the federal regulatory agency that assures the safety and efficacy of medical devices and therapeutic advances—is supported by funds from the federal government. The consecutive increases for the NIH budget in the last seven fiscal years have helped maintain the momentum of progress (see Investments in Research Fuel a Healthier Future ). To keep up with the pace of scientific and technological innovation, it is imperative, however, that Congress continue to provide sustained, robust, and predictable increases in investments in the federal agencies that are vital for fueling progress against cancer, in particular, NIH, NCI, FDA, and CDC, in the years ahead (see AACR Call to Action ).
- A Message from AACR
- Executive Summary
- A Snapshot of a Year in Progress
- Cancer in 2023
- Understanding the Path to Cancer Development
- Reducing the Risk of Cancer Development
- Screening for Early Detection
- Advancing the Frontiers of Cancer Science and Medicine
- Spotlight on Immunotherapy: Pushing the Frontier of Cancer Medicine
- Perspective: Looking to the Future of Immunology
- Supporting Cancer Patients and Survivors
- Envisioning the Future of Cancer Science and Medicine
- Advancing the Future of Cancer Research and Care Through Evidence-based Policies
- AACR Call to Action
- AACR President’s Vision: Future of Cancer Research and Care
- AACR Cancer Progress Report 2023: Steering Committee
Your donation to the American Association for Cancer Research helps our more than 58,000 members worldwide drive progress against cancer.


- WHO Classification of Tumours
- IAC-IARC-WHO Cytopathology Reporting Systems
- IARC Monographs on the Identification of Carcinogenic Hazards to Humans
- IARC Monographs Supplements
- IARC Scientific Publications
- IARC Technical Publications
- IARC Handbooks of Cancer Prevention
- IARC Working Group Reports
- IARC Biennial Reports
World Cancer Reports
- The History of IARC
- IARC Selected Scientific Activities
- Directories of Agents Being Tested for Carcinogenicity
- Other Non-Series Publications
- IARC CancerBases
- Journal Articles
World Cancer Reports are recognized as an authoritative source of global perspective and information on cancer, including cancer patterns, causes, biological processes, and prevention. The latest World Cancer Report , published in 2020, has a specific focus on cancer prevention and the recent research that underpins prevention, and includes a section on inequalities that affect the distribution of cancer within communities. The World Cancer Report Updates learning platform provides learning resources and opportunities related to content from the 2020 World Cancer Report , as well as on current developments in cancer research for cancer prevention.
- World Cancer Reports (5)
- The History of IARC (2)
- IARC Selected Scientific Activities (4)
- Directories of Agents Being Tested for Carcinogenicity (17)
- Other Non-Series Publications (42)

World Cancer Report: Cancer Research for Cancer Prevention
Edited by Wild CP, Weiderpass E, Stewart BW
Formats: Buy Print Book, Download Free PDF

World Cancer Report 2014
Edited by Stewart BW, Wild CP
Formats: Buy Print Book, Download Free PDF, EPUB

World Cancer Report 2008
Edited by Boyle P, Levin B

Le cancer dans le monde 2003
Edited by Stewart BW, Kleihues P

World Cancer Report 2003
- Cancer Topics
- Research Branches
- Research Teams
- Knowledge Transfer
- Research Project Websites
- International Research Collaborations
- Useful Links
- Press Releases
- Featured News
- Videos and Podcasts
- Infographics and Photos
- Questions and Answers
- Publications
- Scientific Meetings and Lectures
- IARC Seminar Series
- IARC/NCI Tumour Seminars
- Medals of Honour
- Professional Staff
- General service Staff
- Talent Pools
- Visiting Scientist and Postdoctoral Opportunities
- Postdoctoral Fellowships
- Call for Tenders
- Office of the Director
- Organization and Management
- Supporters and Friends
- IARC Newsletter
- Visitor Information
- Terms of use
- Privacy Policy
- iarc newsletter
World Cancer Report
Content overview.
Section 1: The global cancer burden
The impact of cancer on the world community is most immediately clear from the number of new cases and mortality. Information currently available presents cancer occurrence in relation to a broad perspective on disease prevention. Beyond this, data from cancer registries in almost all countries enable changes over time (trends) in particular tumour types to be documented. Once recognized, changes in cancer incidence can often be attributed to patterns of human development, and such relationships in turn provide clear opportunities for cancer prevention.
Section 2: Causes of cancer, including hazardous circumstances
The fact that a proportion of most tumour types are caused by particular chemicals, radiation, or biological organisms offers, in most instances, an opportunity for cancer prevention. Some causes of cancer have been known for many decades, although exploitation of this knowledge to prevent cancer has rarely been optimal, particularly from a global perspective. Research findings on cancer causation encompass new insights for both well-recognized carcinogens and those cancer-causing agents that have been recently described. A daunting aspect of research is the extent to which carcinogen exposure – and a consequential burden of disease – that has been controlled in one country or community then emerges in another, even to a greater extent.
Section 3: Biological processes in cancer development
Exposure to a particular carcinogen – or, more commonly, multiple circumstances of exposure – accounts for a proportion of human cancers, acting through different biological pathways at a cellular and molecular level. However, not all people known to be at risk after carcinogen exposure develop cancer. Independently, some people are at greater than average risk of developing cancer because of cancer in earlier generations, but not all members of affected families are afflicted. Finally, cancer may be diagnosed in people not known to have been exposed to relevant carcinogens or whose family has no relevant history. These various scenarios can be explained to varying degrees by biological processes that affect some or all tissues; some of these processes may themselves be the result of environmental or lifestyle exposures. Certain of these processes are described in this section, with particular reference to how available knowledge might be used for prevention.
Section 4: Inequalities affecting cancer prevention
Inequalities, specifically as determined by educational attainment and limitations on circumstances, including nutrition and housing determined by financial income, may perturb the efficacy of virtually all initiatives calculated to reduce the burden of cancer. Relevant factors may be particular to certain countries or regions. Means for investigating such associations, and the manner in which adverse outcomes may be minimized, have improved in recent times. Typically, data are available on variations within a particular country, and certain such data are described in this section.
Section 5: Preventing particular tumour types
The truism that cancer is not a single disease but a multiplicity of different diseases is as valid for cancer prevention as it is for clinical management. Broad understandings about cancer causation, development, detection, and avenues to prevention must be qualified to the extent that no specific list of characteristics (e.g. tumour subtypes) and interventions (e.g. methods of early detection) can be applied with equal relevance to all tumour types. Thus, for example, exogenous causes of prostate cancer are not evident; for now, prevention must focus on sporadic disease or detection of precancerous lesions. For many cancers, there are no recognized screening methods applicable to the whole population. However, success with any research undertaking or preventive measure with one tumour type indicates a means to approach the same challenge for other types.
Section 6: The basis for, and outcomes from, prevention strategies
The burden of death from the multiple different tumour types can be reduced in all communities and countries. The incidence of cancer can be reduced by decreasing or eliminating exposure to carcinogens in multiple contexts. Success in reducing smoking-related cancers in some countries indicates a range of measures that may be researched for efficacy in other situations. Changing behaviour related to nutrition, exercise, and weight gain is being actively researched. Vaccination is effective in relation to some cancers caused by infectious agents. Deaths from sporadic cancer may be reduced through chemoprevention and diagnosis of early disease through screening and emerging molecular methods of early diagnosis. Increased risk of cancer may be indicated by family history and addressed by monitoring affected individuals. The extent to which the options summarized here are realized across national boundaries warrants continuing research.
Published in section: Publications
Publication date: 8 November, 2018, 15:01
Direct link: https://www.iarc.who.int/world-cancer-report-content-overview/
Cancer Research

Driving discovery. Powering progress.
Nci research areas.
- Cancer Biology
- Causes of Cancer
- See All Research Areas
Cancer Research & Infrastructure at NCI
- NCI's Clinical Trials Programs
- NCI-Designated Cancer Centers
- Frederick National Laboratory for Cancer Research
- Intramural Research
- Extramural Research
- Cancer Research Workforce
Research Resources & NCI Initiatives
- Resources for Researchers
- The Cancer Moonshot℠
- Childhood Cancer Data Initiative
- Equity and Inclusion Program
- See All Key Initiatives
Research Advances

The 2022 report includes data on new cancer cases and deaths plus a detailed examination of trends in pancreatic cancer and its subtypes.

NCI joins the cancer community in advancing the goals of the National Cancer Plan as part of its research programs.

Studying cancer and its burden on a population-wide scale can provide information that directly affects the health of millions of people.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Ecancermedicalscience
Innovative approaches for cancer treatment: current perspectives and new challenges
Carlotta pucci.
1 Smart Bio-Interfaces, Istituto Italiano di Tecnologia, 56025 Pisa, Italy
a https://orcid.org/0000-0002-8976-3711
Chiara Martinelli
b https://orcid.org/0000-0001-9360-1689
Gianni Ciofani
2 Department of Mechanical and Aerospace Engineering, Politecnico di Torino, 10129 Torino, Italy
c https://orcid.org/0000-0003-1192-3647
Every year, cancer is responsible for millions of deaths worldwide and, even though much progress has been achieved in medicine, there are still many issues that must be addressed in order to improve cancer therapy. For this reason, oncological research is putting a lot of effort towards finding new and efficient therapies which can alleviate critical side effects caused by conventional treatments. Different technologies are currently under evaluation in clinical trials or have been already introduced into clinical practice. While nanomedicine is contributing to the development of biocompatible materials both for diagnostic and therapeutic purposes, bioengineering of extracellular vesicles and cells derived from patients has allowed designing ad hoc systems and univocal targeting strategies. In this review, we will provide an in-depth analysis of the most innovative advances in basic and applied cancer research.
Introduction
Cancer is one of the main causes of death worldwide, and in the past decade, many research studies have focused on finding new therapies to reduce the side effects caused by conventional therapies.
During cancer progression, tumours become highly heterogeneous, creating a mixed population of cells characterised by different molecular features and diverse responsivity to therapies. This heterogeneity can be appreciated both at spatial and temporal levels and is the key factor responsible for the development of resistant phenotypes promoted by a selective pressure upon treatment administration [ 1 ]. Usually, cancer is treated as a global and homogeneous disease and tumours are considered as a whole population of cells. Thus, a deep understanding of these complex phenomena is of fundamental importance in order to design precise and efficient therapies.
Nanomedicine offers a versatile platform of biocompatible and biodegradable systems that are able to deliver conventional chemotherapeutic drugs in vivo , increasing their bioavailability and concentration around tumour tissues, and improving their release profile [ 2 ]. Nanoparticles can be exploited for different applications, ranging from diagnosis to therapy [ 2 ].
Recently, extracellular vesicles (EVs), responsible for cancer development, microenvironment modification and required for metastatic progression, have been widely investigated as efficient drug delivery vehicles [ 3 ].
Natural antioxidants and many phytochemicals have been recently introduced as anti-cancer adjuvant therapies due to their anti-proliferative and pro-apoptotic properties [ 4 , 5 ].
Targeted therapy is another branch of cancer therapy aiming at targeting a specific site, such as tumour vasculature or intracellular organelles, leaving the surroundings unaffected. This enormously increases the specificity of the treatment, reducing its drawbacks [ 6 ].
Another promising opportunity relies on gene therapy and expression of genes triggering apoptosis [ 7 ] and wild type tumour suppressors [ 8 ], or the targeted silencing mediated by siRNAs, currently under evaluation in many clinical trials worldwide [ 9 ].
Thermal ablation of tumours and magnetic hyperthermia are opening new opportunities for precision medicine, making the treatment localised in very narrow and precise areas. These methods could be a potential substitute for more invasive practices, such as surgery [ 10 , 11 ].
Furthermore, new fields such as radiomics and pathomics are contributing to the development of innovative approaches for collecting big amounts of data and elaborate new therapeutic strategies [ 12 , 13 ] and predict accurate responses, clinical outcome and cancer recurrence [ 14 – 16 ].
Taken all together, these strategies will be able to provide the best personalised therapies for cancer patients, highlighting the importance of combining multiple disciplines to get the best outcome.
In this review, we will provide a general overview of the most advanced basic and applied cancer therapies, as well as newly proposed methods that are currently under investigation at the research stage that should overcome the limitation of conventional therapies; different approaches to cancer diagnosis and therapy and their current status in the clinical context will be discussed, underlining their impact as innovative anti-cancer strategies.
Nanomedicine
Nanoparticles are small systems (1–1,000 nm in size) with peculiar physicochemical properties due to their size and high surface-to-volume ratio [ 17 ]. Biocompatible nanoparticles are used in cancer medicine to overcome some of the issues related to conventional therapies, such as the low specificity and bioavailability of drugs or contrast agents [ 2 ]. Therefore, encapsulation of the active agents in nanoparticles will increase their solubility/biocompatibility, their stability in bodily fluids and retention time in the tumour vasculature [ 18 – 20 ]. Furthermore, nanoparticles can be engineered to be extremely selective for a precise target [ 21 , 22 ] (see the “Targeted therapy and immunotherapy” section) and to release the drug in a controlled way by responding to a specific stimulus [ 18 , 23 – 25 ]. This is the case of ThermoDox, a liposomal formulation that can release doxorubicin as a response to an increment of temperature [ 26 ].
Inorganic nanoparticles are generally used as contrast agents for diagnosis purposes. Among them, quantum dots are small light-emitting semiconductor nanocrystals with peculiar electronic and optical properties, which make them highly fluorescent, resistant to photobleaching and sensitive for detection and imaging purposes [ 27 ]. Combined with active ingredients, they can be promising tools for theranostic applications [ 27 ]. In a recent study, quantum dots coated with poly(ethylene glycol) (PEG) were conjugated to anti-HER2 antibody and localised in specific tumour cells [ 28 ].
Superparamagnetic iron oxide nanoparticles (SPIONs) are usually exploited as contrast agents in magnetic resonance imaging (MRI) because they interact with magnetic fields [ 29 , 30 ]. Five types of SPIONs have been tested for MRI: ferumoxides (Feridex in the US, Endorem in Europe), ferucarbotran (Resovist), ferucarbotran C (Supravist, SHU 555 C), ferumoxtran-10 (Combidex) and NC100150 (Clariscan). Ferucarbotran is currently available in few countries, while the others have been removed from the market [ 25 ]. SPIONs have also been studied for cancer treatment by magnetic hyperthermia (see the “Thermal ablation and magnetic hyperthermia” section), and a formulation of iron oxide coated with aminosilane called Nanotherm has been already approved for the treatment of glioblastoma [ 31 ].
Gold nanoparticles have raised interest because of their optical and electrical properties and low toxicity [ 32 – 34 ]. They are mainly used as contrast agents for X-ray imaging, computed tomography [ 25 ], photoacoustic imaging [ 35 ] and photodynamic therapy [ 36 ]. A nanoshell made of a silica core and a gold shell coated with PEG was approved by the Food and Drug Administration (FDA) in 2012 and commercialised as AuroShell (Nanospectra) for the treatment of breast cancer by photodynamic therapy [ 25 ].
Organic nanoparticles are mainly used as delivery systems for drugs. Liposomes and micelles are both made of phospholipids, but they differ in their morphology. Liposomes are spherical particles having at least one lipid bilayer, resembling the structure of cell membranes. They are mainly used to encapsulate hydrophilic drugs in their aqueous core, but hydrophobic drugs can also be accommodated in the bilayer or chemically attached to the particles [ 37 ]. Micelles, instead, own a hydrophobic core that can encapsulate hydrophobic drugs [ 38 ]. Doxil, doxorubicin-loaded PEGylated liposomes, were the first nanoparticles approved by the FDA in 1995 to treat AIDS-associated Kaposi’s sarcoma [ 39 ]. This formulation drastically reduces doxorubicin side effects. Since then, other liposomal formulations have been approved by the FDA for cancer therapy, such as Myocet and DaunoXome [ 40 – 42 ]. Polymeric nanoparticles are made of biocompatible or natural polymers, such as poly(lactide-co-glycolide), poly(ε-caprolactone), chitosan, alginate and albumin [ 43 ]. Some formulations have already been accepted by the FDA, such as Abraxane (albumin-paclitaxel particles for the treatment of metastatic breast cancer and pancreatic ductal adenocarcinoma) and Ontak (an engineered protein combining interleukin-2 and diphtheria toxins for the treatment of non-Hodgkin’s peripheral T-cell lymphomas).
As well as these systems, which have been either accepted or are under clinical investigation, it is worth mentioning some new nanoparticles currently undergoing testing at the research level, which should improve treatment performance. For example, solid lipid nanoparticles, made of lipids that are solid at body temperature [ 44 ], and fabricated to load hydrophobic drugs [ 45 ] have been demonstrated to give a higher drug stability and prolonged release compared to other systems; however, the encapsulation efficiency is often low because of their high crystallinity [ 46 ]. To overcome this issue, one or more lipids, liquid at room temperature (like oleic acid, for example), are included in the formulation [ 47 ]. Lipid nanoparticles are good candidates for brain tumour therapy as they are able to cross the blood–brain barrier (BBB) [ 48 ]. A recent work showed that lipid nanoparticles loaded with SPIONs and temozolomide are efficient to treat glioblastoma since they combine the effect of the conventional chemotherapy and hyperthermia [ 49 , 50 ]. Dendrimers are another family of nanoparticles composed of polymers with a repetitive branched structure and characterised by a globular morphology [ 51 , 52 ]. Their architecture can be easily controlled, making their structure extremely versatile for many applications. For example, some recent studies show that poly-L-lysine (PLL) dendrimers loaded with doxorubicin induce anti-angiogenic responses in in vivo tumour models [ 53 ]. Currently, there is only one clinical trial for a formulation named ImDendrim based on a dendrimer and on a rhenium complex coupled to an imidazolium ligand, for the treatment of inoperable liver cancers that do not respond to conventional therapies [ 54 ].
Extracellular vesicles for cancer diagnosis and therapy
EVs are classified in two categories based on their biogenesis. Specifically, exosomes are small vesicles of around 30–150 nm originated from endosomes in physiological and pathological conditions and released by a fusion of multivesicular bodies (MVBs) to the cell membrane [ 55 , 56 ], while shed microvesicles (sMVs), with a typical size of 50–1,300 nm, are present in almost any extracellular bodily fluid and are responsible for the exchange of molecular materials between cells [ 57 , 58 ]. Exosomes are involved in cancer development and spreading [ 3 , 59 , 60 ], in the bidirectional communication between tumour cells and surrounding tissues, and in the construction of the microenvironment needed for pre-metastatic niche establishment and metastatic progression [ 61 ]. Hence, circulating vesicles are clinically relevant in cancer diagnosis, prognosis and follow up. Exosomes are actually recognised as valid diagnostic tools, but they can also be isolated and exploited as anti-cancer vaccines or nanosized drug carriers in cancer therapy [ 62 ].
Nowadays, one of the main issues in cancer diagnosis is the early identification of biomarkers by non-invasive techniques. Obtaining a significant amount of information, before and during tumour treatment, should allow the monitoring of cancer progression and the efficacy of therapeutic regimens. Liquid biopsies to detect circulating tumour cells, RNAs, DNAs and exosomes have been used as indicators for personalised medicine [ 63 ]. In recent years, exosomes detection has been validated as a reliable tool for preclinical practice in different cancer types [ 64 ], thanks to the identification of their content: double-stranded DNA (dsDNA) [ 65 , 66 ], messenger RNA (mRNA), micro RNA (miRNA), long non-coding RNA (lncRNA) [ 67 ], proteins and lipids [ 68 ]. DsDNA has been detected in exosomes isolated from plasma and serum of different cancer cell types, and mutated genes involved in tumorigenesis, such as mutated KRAS and TP53 [ 69 , 70 ], have been identified as disease predictors. Similarly, exosomal AR-V7 mRNA has been used as a prognostic marker of resistance to hormonal therapy in metastatic prostate cancer patients [ 71 ]. Gene expression profiling of multiple RNAs from urinary exosomes has been adopted as an efficient diagnostic tool [ 72 ]. LncRNAs isolated from serum exosomes have been exploited for disease prognosis in colorectal cancer patients [ 73 ], and multiple miRNAs allow one to distinguish between different lung cancer subtypes [ 74 ]. GPC1-positive exosomes have been employed to detect pancreatic cancer [ 75 ], while circulating exosomal macrophage migration inhibitory factor (MIF) was able to predict liver metastasis onset [ 76 ]. Finally, multiple lipids present in urinary exosomes have been approved as prostate cancer indicators [ 77 ]. Due to the high variability of patient classes and sample size, and in order to obtain clinically significant results for a fast and effective diagnosis, huge investments in exosome research will be required in the near future.
Exosomes could also be exploited as natural, biocompatible and low immunogenic nanocarriers for drug delivery in cancer therapy. They can be passively loaded by mixing purified vesicles with small drugs [ 78 – 82 ], or actively loaded by means of laboratory techniques, such as electroporation and sonication [ 83 , 84 ]. Superparamagnetic nanoparticles conjugated to transferrin have been tested for the isolation of exosomes expressing transferrin receptor from mice blood. After incubation with doxorubicin, they have been used to target liver cancer cells in response to external magnetic fields, inhibiting cell growth both in vitro and in vivo [ 80 ]. Kim et al. [ 83 ] engineered mouse macrophage-derived exosomes with aminoethyl anisamide-PEG to target sigma receptor, overexpressed in lung cancer cells and passively loaded them with paclitaxel. These systems acted as targeting agents able to suppress metastatic growth in vivo .
Three clinical trials with loaded exosomes are currently ongoing for the treatment of different tumours [ 85 – 87 ]: a phase I trial is evaluating the ability of exosomes to deliver curcumin to normal and colon cancer tissues [ 85 ]; a phase II trial is investigating the in vivo performance of autologous tumour cell-derived microparticles carrying methotrexate in lung cancer patients [ 86 ] and a clinical inquiry is focusing on autologous erythrocyte-derived microparticles loaded with methotrexate for gastric, colorectal and ovarian cancer treatment [ 87 ].
Recently, new strategies to produce ad hoc exosomes have been developed. Cells releasing exosomes have been genetically engineered to overexpress specific macromolecules, or modified to release exosomes with particular targeting molecules [ 88 – 90 ].
Exosomes derived from different cancer cells have already been exploited as cancer vaccines. Autologous dendritic cell-derived exosomes with improved immunostimulatory function have been tested in a phase II clinical trial for the activation of CD8 + T cells [ 91 ] in non-small cell lung cancer (NSCLC) patients, observing disease stabilisation and a better overall survival [ 92 ]. In a phase I trial, ascites-derived exosomes supplemented with granulocyte-macrophage colony stimulating factor (GM-CSF) have been administered to colorectal cancer patients, soliciting a tumour-specific immune response [ 93 ].
Many issues related to exosomes clinical translation remain open and are mostly connected to the definition of preclinical procedures for isolation, quantification, storage and standard protocols for drug loading. It is becoming even more necessary to distinguish between tumour and healthy blood cell-derived vesicles to characterise their post-isolation half-life and to perform standard content analyses. For these purposes, innovative approaches and technologies have been set up, such as microarrays and specific monoclonal antibodies and RNA markers amplification strategies [ 94 ].
Natural antioxidants in cancer therapy
Every day, the human body undergoes several exogenous insults, such as ultraviolet (UV) rays, air pollution and tobacco smoke, which result in the production of reactive species, especially oxidants and free radicals, responsible for the onset of many diseases, including cancer. These molecules can also be produced as a consequence of clinical administration of drugs, but they are also naturally created inside our cells and tissues by mitochondria and peroxisomes, and from macrophages metabolism, during normal physiological aerobic processes.
Oxidative stress and radical oxygen species are able to damage DNA (genetic alterations, DNA double strand breaks and chromosomal aberrations [ 95 , 96 ]) and other bio-macromolecules [ 97 ], such as lipids (membrane peroxidation and necrosis [ 98 ]) and proteins (significantly changing the regulation of transcription factors and, as a consequence, of essential metabolic pathways [ 99 ]).
The protective mechanisms our body has developed against these molecules are sometimes insufficient to counteract the huge damages produced. Recently, in addition to research into the roles of the physiological enzymes superoxide dismutase (SOD), catalase (CAT) and glutathione peroxidase (GP), natural antioxidants such as vitamins, polyphenols and plant-derived bioactive compounds are being studied in order to introduce them as preventive agents and potential therapeutic drugs [ 100 , 101 ]. These molecules have anti-inflammatory and anti-oxidant properties and are found in many vegetables and spices [ 102 ]. Vitamins, alkaloids, flavonoids, carotenoids, curcumin, berberine, quercetin and many other compounds have been screened in vitro and tested in vivo , displaying appreciable anti-proliferative and pro-apoptotic properties, and have been introduced as complementary therapies for cancer [ 4 , 5 , 103 ].
Despite the advantages of using natural drugs, their translation into clinical practice remains difficult due to their limited bioavailability and/or toxicity. Curcumin, a polyphenolic compound extracted from turmeric ( Curcuma longa ), is a traditional Southeast Asian remedy with anti-inflammatory, anti-oxidant and chemopreventive and therapeutic activities [ 104 ]. It has been shown to have cytotoxic effects in different kinds of tumours, such as brain, lung, leukaemia, pancreatic and hepatocellular carcinoma [ 105 , 106 ], with no adverse effects in normal cells at the effective therapeutic doses [ 107 ]. Curcumin can modulate a plethora of cellular mechanisms [ 108 , 109 ]; however, its biological properties, and as a consequence, the treatment duration and the efficient therapeutic doses, have not been completely elucidated yet. This molecule is highly lipophilic, poorly soluble in water and not very stable [ 110 ]. Different strategies and specific carriers, such as liposomes and micelles [ 111 , 112 ], have been developed to improve its bioavailability. Currently, 24 clinical trials involving curcumin are ongoing and 23 have been already completed [ 113 ].
Berberine is an alkaloid compound extracted from different plants, such as Berberis . Recently, it has been demonstrated to be effective against different tumours and to act as a chemopreventive agent, modulating many signalling pathways [ 114 , 115 ]. Like curcumin, it is poorly soluble in water; therefore, different nanotechnological strategies have been developed to facilitate its delivery across cell membranes [ 116 – 119 ]; six clinical trials are open and one has been completed [ 120 ].
Quercetin, a polyphenolic flavonoid found in fruits and vegetable, has been proven to be effective to treat several tumours, such as lung, prostate, liver, colon and breast cancers [ 121 – 123 ], by binding cellular receptors and interfering with many signalling pathways [ 124 ]. Interestingly, it has been shown to be effective also in combination with chemotherapeutic agents [ 125 ]. Presently, seven clinical trials are open and four have been completed [ 126 ].
Targeted therapy and immunotherapy
One of the main problems of conventional cancer therapy is the low specificity of chemotherapeutic drugs for cancer cells. In fact, most drugs act both on healthy and diseased tissues, generating severe side effects. Researchers are putting a lot of effort into finding a way to target only the desired site. Nanoparticles have raised great interest for their tendency to accumulate more in tumour tissues due to the enhanced permeability and retention effect (EPR) [ 127 ]. This process, called passive targeting, relies on the small size of nanoparticles and the leaky vasculature and impaired lymphatic drainage of neoplastic tissues [ 6 ]. Passive targeting, however, is difficult to control and can induce multidrug resistance (MDR) [ 128 ]. Active targeting, on the other hand, enhances the uptake by tumour cells by targeting specific receptors that are overexpressed on them [ 129 , 130 ]. Nanoparticles, for example, can be functionalized with ligands that univocally bind particular cells or subcellular sites [ 6 ]. Several kinds of ligands can be used, such as small molecules, peptides, proteins, aptamers and antibodies.
Folic acid and biotin are small molecules, whose receptors are overexpressed in tumour tissues. Several nanocarriers have been functionalized with folic acid to target ovarian and endometrial cancers [ 131 ]: folic acid-conjugated polyethylene glycol-poly(lactic-co-glycolic acid) nanoparticles delivering docetaxel increased drug cellular uptake by human cervical carcinoma cells [ 132 ]. Small ligands are cheap and can be linked to nanoparticles by simple conjugation chemistry [ 133 , 134 ].
Different kinds of small peptides and proteins are also effective in active targeting. Angiopep-2 is a peptide that has raised great interest in the treatment of brain cancer [ 135 ], because it binds to low-density lipoprotein receptor-related protein-1 (LRP1) of endothelial cells in the BBB, and it is also overexpressed in glioblastoma cancer cells [ 136 ]. Bombesin peptide conjugated to poly(lactic-co-glycolic acid) (PLGA) nanoparticles loaded with docetaxel was used to target the gastrin-releasing peptide receptor, overexpressed on cell surface of prostate, breast, ovarian, pancreatic and colorectal cancer cells [ 137 , 138 ]. Transferrin is a serum glycoprotein overexpressed on many solid tumours, especially on glioblastoma multiforme cells [ 139 ], and on epithelial cells of the BBB [ 6 , 140 ]. Transferrin-conjugated chitosan-PEG nanoparticles delivering paclitaxel exhibited a higher cytotoxicity towards transferrin-overexpressing human non-small cell lung cancer cells (NSCLCs) (HOP-62) [ 141 ].
Aptamers are small synthetic single-stranded RNA or DNA oligonucleotides folded into specific shapes that make them capable of binding specific targets [ 142 ]. Farokhzad et al. [ 143 ] reported that the use of A10 RNA aptamer conjugated to docetaxel-loaded nanoparticles significantly enhances in vitro cytotoxicity. The same aptamer has been also used to prepare quantum dot-doxorubicin conjugates [ 144 ].
Antibodies are currently the most exploited ligands for active targeting. These proteins have a typical ‘Y’ shape, where the two arms are responsible for the selective interaction with the antigen [ 145 ]. Antibodies can be used as immunoconjugates, when conjugated to a drug or nanoparticle, or naked. In the first case, their function is mainly to target a specific antigen overexpressed on cancer cells. Antibodies used for this purpose include those ones that bind to the human epidermal growth factor receptor 2 (HER2), the epidermal growth factor receptor (EGFR), the transferrin receptor (TfR) and the prostate-specific membrane antigen (PSMA) [ 6 ]. Rapamycin-PLGA nanoparticle conjugated to EGFR antibody exhibited higher cellular uptake by human breast adenocarcinoma cells (MCF-7), with enhanced apoptotic activity [ 146 ]. Loperamide-loaded human serum albumin nanoparticles conjugated to antibodies that specifically bind transferrin receptor successfully crossed the BBB and delivered the drug to the desired site [ 147 ].
Naked antibodies or immunoconjugates can also be used in immunotherapy, which is a cancer treatment that aims at stimulating or restoring the immune system of the patient against cancer cells [ 148 ]. Antibodies can act as markers for cancer cells to make them more vulnerable to the immune system response (non-specific immune stimulation), or as inhibitors for immune checkpoint proteins on cancer cell surface, that can modulate the action of T-cells [ 148 ]. Several antibodies have been already tested and accepted by FDA for immunotherapy, such as rituximab (1997, [ 149 ]), ibritumomab tiuxetan (2002, [ 150 ]), trastuzumab emtansine (2013, [ 151 ]), nivolumab (2014, [ 152 ]) and pembrolizumab (2014, [ 153 ]).
Immunotherapy can be achieved by another strategy called adoptive cell transfer (ACT) and it consists of isolating T-lymphocytes (T-cells) with the highest activity against cancer directly from the patient’s blood, expanding them ex vivo , and reinfusing them again into the patient [ 154 ]. Autologous T-cells can be genetically engineered in vitro to express a chimaeric antigen receptor (CAR), which makes them more specific against cancer cell antigens [ 148 ]. Different CARs can be designed to be directed against a certain cancer antigen. The genetic modification of T-cells can be achieved by different methods such as viral transduction, non-viral methods like DNA-based transposons, CRISPR/Cas9 or other plasmid DNA and mRNA transfer techniques (i.e., electroporation, encapsulation in nanoparticles) [ 155 ]. ACT protocols have been already adopted in clinical practice for advanced or recurrent acute lymphoblastic leukaemia and for some aggressive forms of non-Hodgkin’s lymphoma [ 148 ]. For example, it has been shown that the treatment of end-stage patients affected by acute lymphocytic leukaemia with CAR T-cells led to a full recovery in up to 92% of patients [ 155 ]. Despite these very promising results, much research is currently devoted to understanding the long-term side effects of CAR T-cell therapies and their fate within tumours, and to improving CAR T-cell expansion technologies.
Gene therapy for cancer treatment
Gene therapy is intended as the introduction of a normal copy of a defective gene in the genome in order to cure specific diseases [ 156 ]. The first application dates back to 1990 when a retroviral vector was exploited to deliver the adenosine deaminase (ADA) gene to T-cells in patients with severe combined immunodeficiency (SCID) [ 157 ]. Further research demonstrated that gene therapy could be applied in many human rare and chronic disorders and, most importantly, in cancer treatment. Approximately 2,900 gene therapy clinical trials are currently ongoing, 66.6% of which are related to cancer [ 158 ]. Different strategies are under evaluation for cancer gene therapy: 1) expression of pro-apoptotic [ 159 , 160 ] and chemo-sensitising genes [ 4 ]; 2) expression of wild type tumour suppressor genes [ 5 ]; 3) expression of genes able to solicit specific antitumour immune responses and 4) targeted silencing of oncogenes.
One approach relied on thymidine kinase (TK) gene delivery, followed by administration of prodrug ganciclovir to activate its expression and induce specific cytotoxicity [ 161 ]. This has been clinically translated for the treatment of prostate cancer and glioma [ 162 – 164 ]. In recent decades, different vectors carrying the p53 tumour suppressor gene have been evaluated for clinical applications. ONYX-015 has been tested in NSCLC patients and gave a high response rate when administered alone or together with chemotherapy [ 165 ]. Gendicine, a recombinant adenovirus carrying wild-type p53 in head and neck squamous cell cancer had a similar success, inducing complete disease regression when combined with radiotherapy [ 166 ].
Despite many achievements, there are still some challenges to face when dealing with gene therapy, such as the selection of the right conditions for optimal expression levels and the choice of the best delivery system to univocally target cancer cells. Gene therapy also presents some drawbacks linked to genome integration, limited efficacy in specific subsets of patients and high chances of being neutralised by the immune system. Therefore, particular interest has been elicited by targeted gene silencing approaches.
RNA interference (RNAi) has been recently established as an efficient technology both for basic research and medical translation. Small interfering RNAs (siRNAs) consist of double-stranded RNAs [ 167 ] able to produce targeted gene silencing. This process is intracellularly mediated by the RNA-induced silencing complex (RISC), responsible for cleaving the messenger RNA (mRNA), thus leading to interference with protein synthesis [ 168 ]. This physiological mechanism has been demonstrated in many eukaryotes, including animals. A few years after RNAi discovery, the first clinical application for wet-age related macular degeneration treatment entered phase I clinical trial [ 169 ]. Since cancer is triggered by precise molecular mechanisms, siRNAs can be rationally designed to block desired targets responsible for cell proliferation and metastatic invasion. This strategy relies on siRNA-mediated gene silencing of anti-apoptotic proteins [ 170 ], transcription factors (i.e., c-myc gene) [ 171 , 172 ] or cancer mutated genes (i.e., K-RAS ) [ 173 ]. Most of the clinical trials currently ongoing are based on local administration of siRNA oligonucleotides in a specific tissue/organ or on systemic delivery throughout the entire body [ 9 , 174 ]. Using siRNA-based drugs has several advantages: 1) safety, since they do not interact with the genome; 2) high efficacy, because only small amounts can produce a dramatic gene downregulation; 3) possibility of being designed for any specific target; 4) fewer side effects when compared to conventional therapies and 5) low costs of production [ 175 , 176 ]. However, siRNAs are relatively unstable in vivo and can be phagocytosed during blood circulation, excreted by renal filtration, or undergo enzymatic degradation [ 177 ]. Occasionally, they can induce off-target effects [ 178 ] or elicit innate immune responses, followed by specific inflammation [ 179 , 180 ]. Since naked siRNAs are negatively charged hydrophilic molecules, they cannot spontaneously cross cell membranes. Consequently, different delivery strategies are currently under study, such as chemical modification, encapsulation into lipid or polymeric carriers or conjugation with organic molecules (polymers, peptides, lipids, antibodies, small molecules [ 181 ], for efficient targeting [ 182 , 183 ]). Chemical modifications include the insertion of a phosphorothioate at 3’ end to reduce exonuclease degradation [ 184 ], the introduction of 2’ O-methyl group to obtain longer half-life in plasma [ 185 ] and the modification by 2,4-dinitrophenol to favour membrane permeability [ 186 ]. Nevertheless, the degradation of modified siRNAs often elicits cytotoxic effects; therefore, it is preferable to design ad hoc nanocarriers.
Different cationic lipid nanoparticles, such as liposomes, micelles and solid lipid nanoparticles [ 183 ], have been exploited for siRNA loading. Cationic liposomes interact with negatively charged nucleic acids, which can be easily transfected by simple electrostatic interactions [ 187 , 188 ]. They can be constituted by 1,2-dioleoyl-3-trimethylammonium propane (DOTAP) and N-{1-(2,3-dioleoyloxy) propyl]-N,N,N-trimethylammonium methyl sulphate (DOTMA) [ 189 ]. A theranostic agent consisting of an anticancer survivin siRNA entrapped in PEGylated liposomes has been developed to achieve simultaneous localisation inside tumour cells by means of entrapped MR agents and fluorophores and reduction of proliferation in vivo [ 190 ].
Neutral liposomes based on 1,2-dioleoyl-sn-glycero-3-phosphatidylcholine (DOPC) have shown high efficacy in mice models of ovarian carcinoma and colorectal cancer [ 191 , 192 ]. A phase I clinical trial is currently recruiting patients for evaluating the safety of siRNA-EphA2-DOPC when administered to patients with advanced and recurrent cancer [ 193 ].
Stable nucleic acid lipid particles (SNALPs) have been evaluated in non-human primates [ 194 ]. SiRNAs have been encapsulated in a mixture of cationic lipids coated with a shell of polyethylene glycol (PEG) [ 195 ]. SNALPs entered a phase I clinical trial in patients affected by advanced solid tumours with liver involvement [ 196 ] and a phase I/II trial for treating neuroendocrine tumours and adrenocortical carcinoma patients refractory to standard therapy [ 197 ].
SiRNAs can be condensed in cationic polymers such as chitosan, cyclodextrin and polyethylenimine (PEI). Chitosan is a natural polysaccharide that, due to its cationic charge, has been exploited as carrier for nucleic acids in vitro and in vivo [ 198 ]. Specifically, a targeted siRNA has been delivered in mice xenografts of breast cancer [ 199 ]. Cyclodextrin polymers coated with PEG, conjugated with human transferrin and carrying a siRNA called CALAA-01, inhibit tumour growth by reducing the expression of M2 subunit of ribonucleotide reductase (R2), and have entered a phase I clinical trial [ 200 ]. PEI is able to form small cationic nanoparticles containing siRNAs and it has been exploited as antitumoural, upon loading with HER-2 receptor-specific siRNA [ 201 ]. A phase II clinical trial is presently starting to evaluate siG12D LODER directed to mutated KRAS oncogene and encapsulated into a biodegradable polymeric matrix for locally treating advanced pancreatic cancer patients in combination with chemotherapy [ 202 ].
SiRNAs may be conjugated to peptides, antibodies and aptamers in order to improve their stability during circulation and to enhance cellular uptake [ 203 ]. A success is represented by siRNAs targeting PSMA, overexpressed in this type of cancer [ 204 ].
The introduction of nanocarriers has largely improved siRNAs stability, pharmacokinetics and biodistribution properties, and the targeting specificity [ 205 , 206 ]. Smart nanomaterials responsive to external (i.e., magnetic field, ultrasounds) and tumour-specific stimuli (i.e., acidic pH, redox conditions) are currently under the development for controlled release and reduction of undesired negative effects [ 207 , 208 ]. Nanocarriers delivering siRNAs undergo a series of pH variations from blood circulation to intracellular environment and, for this reason, many pH responsive materials have been designed to favour cargo release under specific pH conditions [ 209 ]. Poly(allylamine) phosphate nanocarriers, stable at physiological pH, have been developed to release siRNAs in the cytoplasm after disassembly at low endosomal pH [ 210 ].
Although there have been many successes, some questions remain open and make the clinical translation of the siRNA-based approach very challenging, such as the correct doses to be delivered to patients and the many variabilities observed between individuals and different stages of disease. Further research towards controlled release to reach only specific targets, and the set-up of the best personalised therapy for cancer patients will be necessary in the near future.
Thermal ablation and magnetic hyperthermia
Thermal ablation of tumours includes a series of techniques that exploit heat (hyperthermia) or cold (hypothermia) to destroy neoplastic tissues [ 13 ]. It is known that cell necrosis occurs at temperatures lower than -40°C or higher than 60°C. Long exposures to temperatures between 41°C and 55°C are also effective for tumour cell damage. Moreover, it has been shown that cancer cells are more sensitive to high temperatures than healthy ones [ 211 ].
Hypothermic ablation is due to the formation of ice crystals upon cooling, which destroy cell membranes and finally kill cells. Argon gas is the preferred cooling agent because it can cool down the surrounding tissues to -160°C. Also, gases at their critical point, such as nitrogen, can be exploited since they have a higher heat capacity than argon. However, the technology to control and direct them is not well developed yet [ 10 ].
Hyperthermic ablation currently comprises radiofrequency (RF), microwave and laser ablation [ 10 ].
RF ablation is the most used in clinics, because it is effective and safe [ 212 ]. An alternated current of RF waves is applied to a target zone by an insulated electrode tip, while a second electrode, needed to close the circuit, is placed on the skin surface [ 10 ]. The interaction with the current causes the oscillation of ions in the extracellular fluid, which, in turns, produces heat. The more conductive the medium, the more effective the process. For this reason, RF ablation works very well in the liver and in other areas with a high content of water and ions, whereas it has a poor effect in lungs [ 10 ]. Moreover, the efficiency of the treatment decreases with the size of the lesion, giving the best results for areas not larger than 3 cm 2 [ 213 , 214 ].
Microwave ablation is based on the electromagnetic interaction between microwaves and the polar molecules in tissues, like water, that causes their oscillation and the consequent increase in temperature. Unlike the electrical current in RF ablation, microwaves can propagate through any kind of tissue [ 215 , 216 ], and this allows high temperatures to be reached in a short amount of time, to have a deeper penetration and to treat larger areas of tumours [ 217 ].
Laser therapy exploits the properties of laser beams of being very narrow and extremely focused at a specific wavelength. This makes the treatment very powerful and precise, thus a promising alternative to conventional surgery [ 218 ]. The absorption of the light emitted by the laser results in the heating and subsequent damage of the treated area [ 219 ]. Depending on the specific application, different kinds of lasers can be used. Neodymium:yttrium-aluminium-garnet (Nd:YAG) lasers (wavelength of 1064 nm) and diode lasers (wavelength of 800–900 nm) are used to treat internal organs, since they have a penetration depth up to 10 cm [ 218 ]. Conversely, CO 2 lasers (10,600 nm), with a penetration depth of 10 μm up to 1 mm maximum are used for superficial treatments. Laser therapy is receiving a lot of attention in research because of its advantages compared to other ablation techniques, such as a higher efficacy, safety and precision, and a shorter treatment session needed to achieve the same results [ 220 , 221 ]. Moreover, the fibres to transmit laser light are compatible with MRI, allowing for a precise measure of the temperature and the thermal dose [ 222 ]. However, there are still some limitations to overcome, such as the need of a very skilled operator to place the fibre in the correct position [ 218 ].
Finally, a new way to heat tumour tissues, currently under study, is through magnetic hyperthermia. This technique exploits superparamagnetic or ferromagnetic nanoparticles that can generate heat after stimulation with an alternating magnetic field. The most studied systems in nanomedicine are SPIONs [ 11 ]. The production of heat, in this case, is due to the alignment of magnetic domains in the particles when the magnetic field is applied, and the subsequent relaxation processes (Brownian and/or Neel relaxations) during which heat is released, when the magnetic field is removed and the magnetisation of the particles reverts to zero [ 223 ]. Magnetic hyperthermia can reach any area of the body and SPIONs can also act as MRI contrast agents to follow their correct localisation before the stimulation. The particles can be coated with biocompatible polymers and/or lipid and functionalized with specific ligands to impart targeting properties [ 224 ]. As already mentioned, until now, just a formulation of 15-nm iron oxide nanoparticles coated with aminosilane (Nanotherm) obtained approval for the treatment of glioblastoma [ 31 ]. SPIONs have also been successfully encapsulated in lipid nanocarriers together with a chemotherapeutic agent to combine chemotherapy and hyperthermia [ 49 , 50 ].
Recent innovations in cancer therapy: Radiomics and pathomics
Efficient cancer therapy currently relies on surgery and, in approximately 50% of patients, on radiotherapy, that can be delivered by using an external beam source or by inserting locally a radioactive source (in this case, the approach is named brachytherapy), thus obtaining focused irradiation. Currently, localisation of the beam is facilitated by image-guided radiotherapy (IGRT), where images of the patient are acquired during the treatment allowing the best amount of radiation to be set. Thanks to the introduction of intensity-modulated radiotherapy (IMRT), radiation fields of different intensities can be created, helping to reduce doses received by healthy tissues and thus limiting adverse side effects. Finally, by means of stereotactic ablative radiotherapy (SABR), it has become feasible to convey an ablative dose of radiation only to a small target volume, significantly reducing undesired toxicity [ 225 ].
Unfortunately, radioresistance can arise during treatment, lowering its efficacy. This has been linked to mitochondrial defects; thus, targeting specific functions have proven to be helpful in restoring anti-cancer effects [ 226 ]. A recent study has shown, for example, that radioresistance in an oesophageal adenocarcinoma model is linked to an abnormal structure and size of mitochondria, and the measurement of the energy metabolism in patients has allowed discrimination between treatment resistant and sensitive patients [ 227 ]. Targeting mitochondria with small molecules acting as radiosensitizers is being investigated for gastrointestinal cancer therapy [ 228 ].
Cancer is a complex disease and its successful treatment requires huge efforts in order to merge the plethora of information acquired during diagnostic and therapeutic procedures. The ability to link the data collected from medical images and molecular investigations has allowed an overview to be obtained of the whole tridimensional volume of the tumour by non-invasive imaging techniques. This matches with the main aim of precision medicine, which is to minimise therapy-related side effects, while optimising its efficacy to achieve the best individualised therapy [ 229 ].
Radiomics and pathomics are two promising and innovative fields based on accumulating quantitative image features from radiology and pathology screenings as therapeutic and prognostic indicators of disease outcome [ 12 , 13 , 230 ]. Many artificial intelligence technologies, such as machine learning application, have been introduced to manage and elaborate the massive amount of collected datasets and to accurately predict the treatment efficacy, the clinical outcome and the disease recurrence. Prediction of the treatment response can help in finding an ad hoc adaptation for the best prognosis and outcome. Nowadays, personalised medicine requires an integrated interpretation of the results obtained by multiple diagnostic approaches, and biomedical images are crucial to provide real-time monitoring of disease progression, being strictly correlated to cancer molecular characterisation.
Radiomics is intended as the high throughput quantification of tumour properties obtained from the analysis of medical images [ 14 , 15 , 231 ]. Pathomics, on the other side, relies on generation and characterisation of high-resolution tissue images [ 16 , 232 , 233 ]. Many studies are focusing on the development of new techniques for image analysis in order to extrapolate information by quantification and disease characterisation [ 234 , 235 ]. Flexible databases are required to manage big volumes of data coming from gene expression, histology, 3D tissue reconstruction (MRI) and metabolic features (positron emission tomography, PET) in order to identify disease phenotypes [ 236 , 237 ].
Currently, there is an urgent need to define univocal data acquisition guidelines. Some initiatives to establish standardised procedures and facilitate clinical translation have been already undertaken, such as quantitative imaging network [ 238 ] or the German National Cohort Consortium [ 239 ]. Precise description of the parameters required for image acquisition and for the creation and use of computational and statistical methods are necessary to set robust protocols for the generation of models in radiation therapy. According to the US National Library of Medicine, approximately 50 clinical trials involving radiomics are currently recruiting patients, and a few have already been completed [ 240 ].
Conclusions and future perspectives
In recent years, research into cancer medicine has taken remarkable steps towards more effective, precise and less invasive cancer treatments ( Figure 1 ). While nanomedicine, combined with targeted therapy, helped improving the biodistribution of new or already tested chemotherapeutic agents around the specific tissue to be treated, other strategies, such as gene therapy, siRNAs delivery, immunotherapy and antioxidant molecules, offer new possibilities to cancer patients. On the other hand, thermal ablation and magnetic hyperthermia are promising alternatives to tumour resection. Finally, radiomics and pathomics approaches help the management of big data sets from cancer patients to improve prognosis and outcome.

At the moment, the most frequent entries concerning cancer therapies in the database of clinical trials ( www.clinicaltrials.gov ) involve the terms targeted therapy, immunotherapy and gene therapy, highlighting that these are the most popular methodologies under investigation, especially because, as already mentioned before, they have been shown to be very promising and effective ( Figure 2A ). However, Figure 2B shows that the clinical trials started in the past decade on different therapies mentioned in this review (except for liposomes-based therapies) have increased in number, showing how the interest on these new approaches is quickly growing in order to replace and/or improve conventional therapies. In particular, radiomics, immunotherapy and exosomes are the entries whose number has increased the most in the last 10 years.

The current scenario for cancer research is wide, offering many possibilities for the constant improvement of treatment, considering not only patient recovery but also caring for their well-being during therapy. As summarised in Table 1 , these new approaches offer many advantages compared to conventional therapies. However, some disadvantages still have to be overcome to improve their performances. Much progress has been made, but many others are likely to come in the near future, producing more and more ad hoc personalised therapies.
Conflicts of interest
The authors declare that they have no conflict of interest.
Funding declaration
This work was partially supported by the Fondazione CaRiPLo, grant no. 2018-0156 (Nanotechnological countermeasures against Oxidative stress in muscle cells Exposed to Microgravity—NOEMI) and by the European Research Council (ERC) under the European Union’s Horizon 2020 Research and Innovation Programme (grant agreement N°709613, SLaMM).
Authors’ contributions
Carlotta Pucci and Chiara Martinelli contributed equally to this work.
Together we are beating cancer
About cancer
Cancer types
- Breast cancer
- Bowel cancer
- Lung cancer
- Prostate cancer
Cancers in general
- Clinical trials
Causes of cancer
Coping with cancer
- Managing symptoms and side effects
- Mental health and cancer
- Money and travel
- Death and dying
- Cancer Chat forum
Health Professionals
- Cancer Statistics
- Cancer Screening
- Learning and Support
- NICE suspected cancer referral guidelines
Get involved
- Make a donation
By cancer type
- Leave a legacy gift
- Donate in Memory
Find an event
- Race for Life
- Charity runs
- Charity walks
- Search events
- Relay For Life
- Volunteer in our shops
- Help at an event
- Help us raise money
- Campaign for us
Do your own fundraising
- Fundraising ideas
- Get a fundraising pack
- Return fundraising money
- Fundraise by cancer type
- Set up a Cancer Research UK Giving Page
- Find a shop or superstore
- Become a partner
- Cancer Research UK for Children & Young People
- Our We Are campaign
Our research
- Brain tumours
- Skin cancer
- All cancer types
By cancer topic
- New treatments
- Cancer biology
- Cancer drugs
- All cancer subjects
- All locations
By Researcher
- Professor Duncan Baird
- Professor Fran Balkwill
- Professor Andrew Biankin
- See all researchers
- Our achievements timeline
- Our research strategy
- Involving animals in research
Funding for researchers
Research opportunities
- For discovery researchers
- For clinical researchers
- For population researchers
- In drug discovery & development
- In early detection & diagnosis
- For students & postdocs
Our funding schemes
- Career Development Fellowship
- Discovery Programme Awards
- Clinical Trial Award
- Biology to Prevention Award
- View all schemes and deadlines
Applying for funding
- Start your application online
- How to make a successful application
- Funding committees
- Successful applicant case studies
How we deliver research
- Our research infrastructure
- Events and conferences
- Our research partnerships
- Facts & figures about our funding
- Develop your research career
- Recently funded awards
- Manage your research grant
- Notify us of new publications
Find a shop
- Volunteer in a shop
- Donate goods to a shop
- Our superstores
Shop online
- Wedding favours
- Cancer Care
- Flower Shop
Our eBay store
- Shoes and boots
- Bags and purses
- We beat cancer
- We fundraise
- We develop policy
- Our global role
Our organisation
- Our strategy
- Our Trustees
- CEO and Executive Board
- How we spend your money
- Early careers
Cancer news
- Cancer News
- For Researchers
- For Supporters
- Press office
- Publications
- Update your contact preferences
ABOUT CANCER
GET INVOLVED
NEWS & RESOURCES
FUNDING & RESEARCH
You are here
Our reports and publications

What's new?
Check here for the latest reports and publications updates
February 2024
January 2024
Explore a selection of reports and publications from the Cancer Intelligence experts at Cancer Research UK, and through various collaborations.
Local Stats Data Hub
The local stats data hub gives provides information across the cancer pathway for each constituency area based on publicly available data. It includes information on smoking prevalence, childhood overweight and obesity, bowel screening, cancer waiting times, cancer incidence and cancer mortality.
Cancer Waiting Times and Diagnostic Activity Data Hub
The CRUK Cancer Intelligence Team’s Cancer Waiting Times and Diagnostic Activity Data Hub gathers the latest data from across the UK on cancer waiting times performance and diagnostic activity and waiting times. You can view breakdowns for some of this information by a specific cancer site and country.
Early Diagnosis Data Hub
The CRUK Cancer Intelligence Team’s Early Diagnosis Data Hub gathers information and statistics across a number of cancer early diagnosis measures including incidence and survival by stage at diagnosis, screening uptake, urgent GP referrals and routes to diagnosis. You can view breakdowns for some of this information by a specific cancer site and country.
Children and Young People’s Cancers Data Hub
The CRUK Cancer Intelligence Team’s Children and Young People Cancer data hub uses data from Public Health England to provide a dashboard for cancer incidence and survival for 0–24-year-olds in the UK and its constituent nations. You can view data for each country by sex, age, main ICCC-3 diagnostic group and diagnostic subgroups.
Cancer Waiting Times

Performance measures across the cancer pathway: Key Stats
COVID-19’s effect on cancer patients is a key concern to the cancer community with delayed or decreased diagnosis, tests and treatment. To understand this variable and rapidly changing landscape the Cancer Intelligence team are regularly monitoring published data around the impact of the pandemic across the cancer pathway. We have prepared some key insights which reports latest data across the UK (and where possible for the devolved nations) on screening, urgent suspected referrals, diagnostic tests and treatment.
Cancer Intelligence Team, Cancer Research UK. Performance measures across the cancer pathway: Key Stats Updated January 2024
Covid-19 and Cancer

Impact of the COVID-19 pandemic on cancer surgery and cancer mortality
This research report from Telstra Health UK and Cancer Research UK explores the potential impact of the COVID-19 pandemic on cancer surgery and cancer mortality, both at the very beginning and throughout 18 months of living with the disruption, fear, and strain. The analysis reveals a general decrease in patients undergoing cancer surgery at the start of the pandemic for all demographic groups, but shows that for the most part the recovery period of the COVID-19 pandemic has not exacerbated inequalities in access to cancer surgery. However we know that there are disparities in access to treatment particularly by age, as well as some evidence of variation by deprivation and region. The report also highlights changes in cancer mortality and place of death. Overall it is shown that there was a profound and sustained impact on cancer services and patients but the true extent of these effects is not yet fully understood.
View the report here
Cancer & COVID-19 Research Summit
Cancer Research UK (CRUK), The National Cancer Research Institute (NCRI) and Public Health England’s National Disease Registration Service (PHE NCRAS) hosted a Cancer/COVID-19 Research Summit with researchers from different disciplines to identify key research themes or questions around COVID-19’s impact on cancer prevention, early diagnosis and screening. Also, to discuss how the impact of COVID-19 on cancer patients can be mitigated through effective research.
Several areas in which further research is needed were identified, as well as lessons from the pandemic to improve research, cancer care, and help prepare for future crises. These include understanding the biological and psychological effects of COVID-19 on cancer patients, risk factors associated with COVID-19 and cancer, the influence of COVID-19 on health-related behaviours and the impact of COVID-19 on cancer care pathways. The full meeting report can be found here.

The impact of COVID-19 on cancer patients’ experience
This report summarises the findings from the CRUK patient experience survey (PES), which collected data from 1st May to 28th May 2020. The findings indicate the impact of COVID-19 on cancer patients, and their testing, treatment and care. For many cancer patients the COVID-19 pandemic appears to have had a significant impact on their testing and treatment, and most notably their care. This has resulted in a negative impact on the emotional well-being of many cancer patients whether they were hoping to finish their treatment, find out the results of their test, have their regular screening, or continue with care that could support them, in some cases for the remainder of their life.
Cancer Research UK. Cancer Research UK Cancer Experience Survey 2020: The impact of COVID-19 on Cancer patients in the UK . July 2020.
Treatment and post diagnosis
Geographic variation in treatment of endometrial Cancer
Our CRUK-PHE partnership team have investigated the geographic variation in the use of lymphonodectomy and external beam radiotherapy (EBRT) in the treatment of endometrial cancer. Significant variation was found between 19 Cancer Alliances using population level cancer registry data collected between 2013-2016, which is likely due to ambiguity in existing endometrial cancer management guidelines.
White B, Nordin A, Fry A et al. Geographic variation in the use of lymphadenectomy and external‐beam radiotherapy for endometrial cancer: a cross‐sectional analysis of population‐based data. BJOG 2019 doi: 10.1111/1471-0528.15914
Risk factors and symptom awareness

Smoking prevalence projections 2021
Smoking is the leading cause of cancer and preventable death in the UK. Smoking prevalence has been declining across the UK for some decades, but remains higher in more deprived groups. The UK Government has set a smokefree ambition (to achieve 5% average adult smoking prevalence) for 2030 in England. There is currently no ambition to achieve smokefree in all deprivation groups.
In this report we estimate whether the smokefree 2030 ambition is likely to be realised based on recent trends, and when smokefree will be achieved for each deprivation decile. We have projected average adult smoking prevalence, and smoking prevalence by deprivation decile, for England until 2050. These projections use smoking prevalence data up to 2021, from the Office for National Statistics’ Annual Population Survey.
The results suggest that if recent trends continue, England will not reach smokefree until 2039, and to achieve the 2030 smokefree target, the pace of change needs to be around 70% faster than projected. The most deprived tenth of the population In England may be almost three decades behind the least deprived tenth, in achieving 5% smoking prevalence. This analysis suggests the pace of decline in smoking prevalence has slowed overall, and the deprivation gap has widened, since our previous projections using data to 2018.
Socio-economic deprivation and cancer incidence in England: Quantifying the role of smoking
Smoking is the leading cause of preventable cancer and death in the UK. Deprived populations typically experience higher rates of smoking and cancer incidence. We calculated the proportion and number of smoking-related cancer cases by deprivation quintile in England and modelled how smoking contributes to the deprivation gap for cancer incidence. We found a strong deprivation gradient for the proportion of cancer cases attributable to smoking in England. Our modelling suggests that more than half (61%) of the deprivation gap for cancer incidence could have been prevented if nobody smoked, indicating smoking to be the key driver for cancer incidence inequality in England.
Payne NWS, Brown KF, Delon C et al. Socio-economic deprivation and cancer incidence in England: Quantifying the role of smoking. PLOS ONE 2022 17(9): e0272202

Adult overweight and obesity prevalence projections for the UK
Overweight and obesity is a major risk factor for the leading causes of death in the world and is causally associated with at least 13 different types of cancer. Overweight and obesity prevalence has increased markedly in the UK in recent decades. We provide projections for overweight and obesity prevalence by sex and deprivation quintile in the UK (where possible) and its constituent nations. These projections, based on current trends in nationally representative health surveys, suggest that there could be more people who are obese than healthy weight in the UK by 2040. In England and Scotland, the deprivation gap for obesity between the least and most deprived is projected to increase by more than half.
Patients with non-specific symptoms
The CRUK-PHE partnership have published a paper comparing patients presenting with non-specific but concerning symptoms with patients presenting with more obvious symptoms. Cancer registration data was linked to the National Cancer and Diagnosis Audit (NCDA) data, which has information about primary care for over 17,000 cancers. The work found that patients with non-specific symptoms had longer primary care intervals, more complex diagnostic pathways and were more likely to be diagnosed at stage 4 and after an emergency presentation. This work supports the evaluation of Multi-Disciplinary Centres (MDCs) by the ACE Programme, an early diagnosis imitative supported by CRUK, MacMillan Cancer Support and NHS England.
Pearson C, Poirier V, Fitzgerald K, et al. Cross-sectional study using primary care and cancer registration data to investigate patients with cancer presenting with non-specific symptoms. BMJ Open 2020; 10: e033008. doi: 10.1136/bmjopen-2019-033008

Cancers attributable to overweight and obesity by deprivation
This report investigates to what extent the proportion of overweight and obesity attributable cancer cases in the UK varies with deprivation. For females, the proportion of cancer cases attributable to overweight and obesity showed a 10-29% relative increase from the least deprived quintile to the most deprived. The deprivation gap was generally much smaller for males. There is a stronger deprivation gradient for obesity prevalence in UK females compared to males, and more overweight and obesity-associated cancer types in females compared to males, which explains the differences observed between sexes.
Cancer Intelligence Team, Cancer Research UK. The fraction of cancer attributable to overweight and obesity by deprivation quintile in the UK . October 2020.

Smoking prevalence projections
UK smoking prevalence has been declining overall for some decades, and ambitions to achieve 5% average adult smoking prevalence (‘smoke-free’) have been set by England for 2030, and Scotland for 2034. These projections, based on current trends in nationally-representative smoking surveys, suggest that 5% average adult smoking prevalence could be reached in 2037 for England and Wales, the late 2040s for Northern Ireland, and after 2050 for Scotland. There could be millions fewer UK smokers than projected in the 2030s, if smoke-free ambitions were achieved; however to do this the pace of change needs to increase markedly in all UK nations. Socioeconomic inequalities are a key concern: the projections indicate that in England, smoke-free could be achieved by the most deprived fifth of the population around 20 years later than in the least-deprived fifth; and in Scotland and Northern Ireland this deprivation gap may be markedly longer.
Cancer Intelligence Team, Cancer Research UK. Smoking prevalence projections for England, Scotland, Wales, and Northern Ireland based on data to 2018/19 . February 2020.

Smoking trends by occupation group
The proportion of current smokers in the population (smoking prevalence) has been falling for decades in the UK, However a clear deprivation gradient remains: smoking prevalence is around twice as high in routine and manual (R&M) workers compared with managerial and professional (M&P) workers. That gap has widened in recent decades, because smoking prevalence has fallen more slowly among R&M workers compared with M&P workers. This reflects both higher rates of uptake and lower rates of quitting in R&M workers compared with M&P workers. Occupation group is associated with smoking behaviour independent of other characteristics like age, sex, region, education, marital status, ethnicity, alcohol consumption and general perceived health. If the R&M worker population had experienced the same pace of decline in smoking prevalence as the M&P population, there would now be almost a million fewer R&M worker smokers.
Cancer Intelligence Team 2019 Smoking prevalence trends by occupation group in health survey for England
Diagnosis and Screening
Relationship between ethnicity and stage at diagnosis
Our CRUK-NHS E partnership team have evaluated whether certain ethnic groups in England are more likely to be diagnosed at a later stage. Reviewing diagnoses of 6 cancer types from 2012-2016 in people belonging to one of 5 ethnic groups, we found that Caribbean, African and Asian women and Caribbean men had increased odds of late-stage disease for certain cancer types compared to the White British cohort. Reasons behind increased late diagnoses may include poorer symptom awareness, delays in seeking help and having to present to the GP multiple times before being referred for tests.
Fry A, White B, Nagarwalla D, et al. Relationship between ethnicity and stage at diagnosis in England: a national analysis of six cancer sites . BMJ Open 2023. doi: 10.1136/bmjopen-2022-062079
10-Year survival by stage for the East of England
In partnership with the National Cancer Registration Services (NCRAS), we have produced 10 year survival by stage estimates for the East of England. 10 year survival gives cancer patients a more accurate reflection of their long term survival experience and this work focuses on the differences in survival by stage at diagnosis. The work highlights the need for continued efforts to achieve diagnosis at earlier stages to improve longer term cancer outcomes. The results for lung, breast, bowel and prostate cancer are shown indicating 10 year survival is much poorer when diagnosed at the latest stage compared to the earlier stages. More information about the method used and wider range of site estimates produced can be found in this technical report.
See the infographic here

Diagnostic Intervals in England
Our CRUK-PHE partnership team have calculated diagnostic intervals for the first time for patients of 25 different cancer sites diagnosed in 2014 & 2015. Significant variation in these intervals were found by stage of disease, route to diagnosis and comorbidity score. An online tool demonstrates variation by these and other factors by cancer site and cancer alliance. A paper describing the methodology and results for colorectal and lung cancer was published in Cancer Epidemiology in June 2019. Two blogs detailed the project, one by CRUK and one at Public Health Matters.
Pearson C, Fraser J, Peake M. Establishing population-based surveillance of diagnostic timeliness using linked cancer registry and administrative data for patients with colorectal and lung cancer . Cancer Epidemiology 2019.
Cancer in the UK

Cancer in the UK: Overview 2024
This report sets out the key challenges facing cancer services and people affected by cancer. We’ve made huge progress on cancer in the last 50 years, but new analysis indicates that improvements in survival have slowed. This next instalment in the Cancer in the UK series highlights the need for political leadership to deliver long-term solutions to the challenges facing cancer research and care.
Devolved nation summaries are also available:
Cancer in the UK: Scotland Overview 2024
Cancer in the UK: Wales Overview 2024
Cancer in the UK: Northern Ireland Overview 2024

Cancer in the UK: Overview 2023
This report sets out the top line view of key challenges facing cancer services, and people affected by cancer today, looking at where progress is being made and the many challenges we face. With cancer cases projected to rise, ensuring we have a long term, comprehensive plan for cancer that tackles these challenges and harnesses the opportunities is vital.
This report is a call to action – all of us must come together to make progress in our ambition to beat cancer. People affected by cancer deserve no less.
Cancer in the UK: Scotland Overview 2023
Cancer in the UK: Wales Overview 2023
Cancer in the UK: Northern Ireland Overview 2023

Cancer in the UK: Deprivation and cancer inequalities in Scotland
This report focuses on the impact of deprivation across the cancer pathway in Scotland. Generally, populations with higher deprivation have greater risk factors for cancer, are less aware of symptoms of cancer and report more barriers to seeking help. Their participation in screening programmes is lower and they are more likely to be diagnosed with late-stage disease. People from more deprived populations have worse cancer outcomes, including survival. We need to make sure we push to achieve lower levels of cancer risk factors, better engagement with the health system and improved cancer outcomes for everyone and close the deprivation gap, because beating cancer must mean beating it for everyone.
Cancer Intelligence Team, Cancer Research UK. Cancer in the UK: Deprivation and cancer inequalities in Scotland . November 2022.

Cancer in the UK: socio-economic deprivation
This report brings together the available evidence across the UK of inequalities in cancer by socio-economic variation and shows the negative experiences and outcomes that people from more deprived groups experience. Generally, populations with higher deprivation have higher prevalence of cancer risk factors, are less aware of symptoms of cancer and report more barriers to seeking help. Their participation in screening programmes is lower and they have higher proportions of cancer diagnosed through routes with worse survival. People from more deprived populations report worse experiences of care and experience inequalities in treatment options. They have worse outcomes. This report presents the evidence for each part of the cancer pathway with examples from all four UK nations.
Cancer Intelligence Team, Cancer Research UK. Cancer in the UK 2020: Socio-economic deprivation . September 2020.
Behavioural Science

Obesity Campaign Evaluation
Overweight and obesity’ is the second biggest preventable cause of cancer after smoking. In 2018, Cancer Research UK launched an awareness raising campaign about the link between overweight and obesity and cancer risk. This study aimed to evaluate the reach and impact of the campaign.The campaign consisted of six elements including the main message that ‘Obesity is a cause of cancer’. UK adults and Members of Parliament (MPs) were surveyed before the campaign (W1; n = 2124 and n = 151), 1 month (W2; n = 2050 and n = 151) and 3 months after the campaign (W3; n = 2059 and MPs not surveyed). Outcome measures were campaign reach, awareness of overweight and obesity as risk factors for cancer, attitudes towards individuals who are overweight or obese, support for policies to reduce obesity and reactions to the campaign. This evaluation suggests that the campaign achieved the primary objective of increasing awareness of the link between obesity and cancer without increasing negative attitudes towards individuals who are overweight or obese.

The effect and cost-effectiveness of mass media campaigns on health behaviour change: A narrative systematic review
Mass media campaigns can reach a large number of people with health messages, but it is unclear how effective these are at changing health behaviours. We conducted a narrative review of systematic reviews to examine the impact of mass media campaigns on eight health behaviours, as well as their cost-effectiveness. Specifically, we explored the impact of mass media campaigns on tobacco use, dietary behaviours, alcohol use, physical activity, sun and UV-protection, HPV vaccination, cancer screening uptake, and symptomatic GP presentation. We concluded that mass media campaigns should be used as part of multi-component, community-based interventions and more research is needed to assess the cost-effectiveness of these types of campaign.
View the full report
Cancer Research UK Lung Cancer screening project
This report presents the data from the 2022 Lung Cancer Screening survey, led by Cancer Research UK (CRUK), conducted by YouGov and with the costs of the project covered by ScottishPower.
This piece of research aims to inform CRUK’s work in the lung cancer space. This may include taking action to support possible widespread introduction of targeted lung cancer screening by the NHS. It could also include work to mitigate any unintended consequences of targeted lung screening – such as impact on perceptions of the risk of lung cancer amongst people who have never smoked.
A bespoke survey was conducted to explore public perceptions around lung cancer and its risks, as well as knowledge and perceptions of screening, including eligibility and the impact of screening. This project built on previous work conducted by CRUK in order to optimise development of targeted lung cancer screening and ensure success of any future programme with minimised unintended consequences.
View the report

Cancer Awareness Measure move to online
The Cancer Awareness Measure (CAM) is a survey designed to assess public awareness of cancer warning signs/symptoms, cancer risk factors and barriers to help seeking. Data has been collected every two years from 2008 to 2014 from a representative face to face sample of Great Britain via the Office of National Statistics (ONS) Opinions and Lifestyle Survey.
In 2017, we analysed the extent to which public awareness of cancer and attitudes toward seeking help vary by online and face-to-face data collection methods. Results showed that online participants were more likely to recall cancer warning signs and risk factors and were also more likely to endorse barriers to help seeking than face to face responders. As a result of this analysis CRUK moved the CAM survey online and the first survey wave took place in 2019.
Cancer Intelligence. Cancer Awareness Measure (CAM) Key Findings Report: Comparing data collected online and face-to-face . October 2019.
Connor K, Hudson B, Power E. Awareness of the Signs, Symptoms, and Risk Factors of Cancer and the Barriers to Seeking Help in the UK: Comparison of Survey Data Collected Online and Face-to-Face. JMIR Cancer 2020;6(1):e14539.
Evaluation: e-cigarette relative harms pilot campaign 2018
An advertising campaign piloted by Cancer Research UK in 2018 aimed to promote quit attempts by increasing awareness of the relative harms of e-cigarettes compared with smoking. A cross-sectional survey evaluation was conducted surveying adults (≥16 years, n = 2217) living in the campaign region and the comparison/control regions. We tested interactions between time (pre, post) and region (campaign, control).
Compared with the control region, the campaign was associated with an increase in smokers’ motivation to quit but a smaller increase in adults’ perception of e-cigarettes as an effective cessation aid. It was identified that using mass media to communicate accurate information about the relative harms of e-cigarettes compared with smoking may be an effective strategy in increasing smokers’ motivation to quit. Further research is needed to evaluate effects on quit attempts and success.
Harry Tattan-Birch, Sarah E Jackson, Charlotte Ide, et al. Evaluation of the Impact of a Regional Educational Advertising Campaign on Harm Perceptions of E-Cigarettes, Prevalence of E-Cigarette Use, and Quit Attempts Among Smokers. Nicotine Tob Res 2019. doi: 10.1093/ntr/ntz236

Image of standard packaging on cigarette boxes
In the United Kingdom, standardised packaging for cigarettes was phased in between May 2016 and May 2017. A cross-sectional online survey was conducted with current smokers aged 16+ in two regions of England when both standardised and fully-branded packs were available. The study found that standardised packaging was associated with increased warning salience and thoughts about risks and quitting. Specifically, compared with never users, current users were more likely to have noticed the warnings on packs often/very often, read them closely often/very often, thought somewhat/a lot about the health risks of smoking and thought somewhat/a lot about quitting. These findings provided support for standardised packaging during the transition period.
Moodie C, Brose LS, Lee HS et al. How did smokers respond to standardised cigarette packaging with new, larger health warnings in the United Kingdom during the transition period? A cross-sectional online survey . Addiction Research & Theory 2019.

Cancer awareness training evaluation
CRUK's training (“Talk Cancer”) aims to increase awareness of screening programmes and risk factors, promote more positive beliefs about cancer and increase confidence to discuss cancer with members of the public, among people working across the health service, local government, community and voluntary sectors who are appropriately placed to have these discussions with the public.
The evaluation found that the trainees' more positive beliefs about cancer, their increased confidence in discussing cancer and their increased awareness of bowel cancer screening were all maintained at 2 months.
Roberts A, Crook L, George H etc al. Two-month follow-up evaluation of a cancer awareness training workshop (“Talk Cancer”) on cancer awareness, beliefs and confidence of front-line public health staff and volunteers . Prev Med Rep 2019.

Exploring public views about delays in cancer screening
This report summarises the findings from an online survey (n=2,115), which contributes to discussions about the ethics of cancer screening in a pandemic situation. It aims to build an understanding of public attitudes towards cancer screening and any potential delays in cancer screening. The majority of participants (86%) wanted to know about any potential delays, and nearly half (48%) would prefer to experience a delay to their invitation over other parts of the screening pathway. The earlier in the pathway a delay is experienced the less anxiety participants anticipated.
This report supports a strategic delaying of cancer screening invitations under the proviso it ensures a shorter wait for follow-up tests and treatment. Ethical considerations about screening should include an emphasis on allowing the public to make an informed decision on their participation.

Exploring public attitudes towards the new Faster Diagnosis Standard for cancer
An exploration into public attitudes towards the new Faster Diagnosis Standard for cancer, due to be introduced in England in 2020, within the context of a patients’ recent referral experiences.
It found that waiting for test results and responsibility for meeting the standard were the main concerns and it was concluded that patients should be asked what they would like to know about their referral and that GPs should be more transparent about the referral process and the potential for a lack of clarity around next steps.
Piano M, Black G, Amelung D et al. Exploring public attitudes towards the new Faster Diagnosis Standard for cancer: a focus group study with the UK public . Br J Gen Pract 2019.
Want to generate bespoke preventable cancers stats statements? Download our interactive statement generator.

A theory and evidence-based redevelopment of a tool to support behaviour change
Research shows that leading a healthy lifestyle can help prevent cancer. Further, diagnosing cancer at an early stage can increase survival rates. Cancer Research UK (CRUK)'s nurse-led outreach activity supports cancer prevention, early diagnosis and screening in deprived community settings. CRUK developed a habit-based behaviour change tool to support this activity and better enable conversations about behaviour change.

Cancer Research UK’s Patient Survey 2021
Mass media campaigns can reach a large number of people with health messages, but it is unclear how effective these are at changing health behaviours. We conducted a narrative review of systematic reviews to examine the impact of mass media campaigns on eight health behaviours, as well as their cost-effectiveness. Specifically, we explored the impact of mass media campaigns on tobacco use, dietary behaviours, alcohol use, physical activity, sun and UV-protection, HPV vaccination, cancer screening uptake, and symptomatic GP presentation. We concluded that mass media campaigns should be used as part of multi-component, community-based interventions and more research is needed to assess the cost-effectiveness of these types of campaign. This report summarises the key findings from the CRUK Patient Survey, which collected data from December 2020 to March 2021. Findings are from patients who share their stories and experiences and give an indication of the impact COVID-19 has had on their testing, treatment and care. New data on remote consultations and COVID-19 safety measures have been collected.
The barriers to timely cancer diagnosis and treatment identified by people affected by cancer in this report are not an entirely new phenomenon that have emerged only in the pandemic. Even before COVID-19, cancer services were on the verge of crisis, and the vast majority of patients surveyed supported governments taking steps required to make expanding capacity in cancer services a reality.

Evaluating the impact of a community-based cancer awareness roadshow on awareness, attitudes and behaviors
Improving public awareness of cancer and encouraging health behavior change are important aspects of cancer control. We investigated whether a community-based roadshow was an effective way of communicating with the public about cancer and encouraging behavior change. Data were from 1196 people who completed questionnaires at a Cancer Research UK Cancer Awareness Roadshow in 2013. Of these, 511 (43%) completed questionnaires immediately before their visit (pre-visit group) and 685 (57%) completed questionnaires immediately after their visit (post-visit group). Among the post-visit sample, 217 (32%) were retained after two months. Self-reported data were available on risk factor and symptom awareness, help-seeking barriers, use of healthcare services and health behaviors. Compared with the pre-visit sample, the post-visit group had greater awareness of cancer risk factors and was more positive about aspects of help-seeking but awareness of potential symptoms was similar. Most effects were maintained over two months. Intentions to eat more fruit and vegetables and to exercise more were comparable between the groups but more people in the post-visit sample intended to quit smoking. At 2-month follow-up, smoking prevalence had significantly reduced but fruit and vegetable consumption decreased and there was no change to physical activity. User of weight loss services and general practitioner visits were high at follow-up and largely attributed to the Roadshow. The Cancer Research UK Roadshow appears to improve risk factor awareness, promote positive attitudes towards help-seeking and increase smoking cessation. This approach could be a useful building block for additional cancer prevention and control strategies.
View the full report
What Drives Public Perceptions of E-cigarettes?
Despite growing evidence that e-cigarettes are less harmful than cigarettes, perceptions of equal or more harm have increased worldwide. This study aimed to identify the most common reasons behind people’s perceptions of the (i) relative harm of e-cigarettes compared with cigarettes and (ii) effectiveness of e-cigarettes for smoking cessation.
View the full report here
Cancer symptom experience and help-seeking behaviour during the COVID-19 pandemic in the UK
Objectives To understand self-reported potential cancer symptom help-seeking behaviours and attitudes during the first 6 months (March–August 2020) of the UK COVID-19 pandemic.
Design UK population-based survey conducted during August and September 2020. Correlates of help-seeking behaviour were modelled using logistic regression in participants reporting potential cancer symptoms during the previous 6 months. Qualitative telephone interviews with a purposeful subsample of participants, analysed thematically.
Read the full report

Intentions to participate in cervical and colorectal cancer screening during the COVID-19 pandemic
Worldwide, cancer screening faced significant disruption in 2020 due to the COVID-19 pandemic . If this has led to changes in public attitudes towards screening and reduced intention to participate, there is a risk of long-term adverse impact on cancer outcomes. In this study, we examined previous participation and future intentions to take part in cervical and colorectal cancer (CRC) screening following the first national lockdown in the UK.
Read the full report

Cancer Awareness Measure September 2022 Findings
The most recent CAM that we have results for is the September 2022 CAM. The next CAM data will be collected in February 2023 and results will be available later in the year.
Key findings from September 2022 CAM
*Note that some figures in the slides have been updated since they were presented at the spotlight session.
Join us on X (previously known as Twitter)
Earlier versions of recurrent reports and surveys may be found on our archived reports and publications page
See all the publications from our policy teams and and current research tenders relevant to policy
Report highlights inequalities and hidden suffering among people living with breast cancer
Many people with breast cancer ‘systematically left behind’, say researchers.

Experts predict 3 million new cases a year of breast cancer worldwide by 2040 and a million deaths, with people living in low- and middle-income countries disproportionately affected. Despite major advances in the diagnosis and treatment, inequalities mean that many women worldwide still experience significant suffering related to physical symptoms, emotional despair, and financial burden.
These are among the conclusions of the new Lancet Commission , led by Professor Charlotte Coles from the University of Cambridge , which sets out recommendations to tackle these urgent challenges in breast cancer. The Commission builds on previous evidence, presents new data, and integrates patient voices to shed light on a large unseen burden.
"Recent improvements in breast cancer survival represent a great success of modern medicine. However, we can’t ignore how many patients are being systematically left behind."
Professor Charlotte Coles, University of Cambridge and Cambridge University Hospitals NHS Foundation Trust
Professor Coles added: "We hope that, by highlighting these inequities and hidden costs and suffering in breast cancer, they can be better recognised and addressed by health care professionals and policymakers in partnership with patients and the public around the world."
At the end of 2020, 7.8 million women were alive having been diagnosed with breast cancer in the previous five years. Progress in research and cancer management has led to a decrease of over 40% in breast cancer mortality in most high-income countries. Estimates suggest that global breast cancer incidence will rise from 2.3 million new cases in 2020 to over 3 million by 2040.
Although breast cancer is the most common cancer, gaps in knowledge continue to prevent effective action.

Professor Charlotte Coles

Lack of information on number of people with metastatic breast cancer
Even though 20-30% of patients with early breast cancer experience relapse, relapse is not typically recorded by most national cancer registries. Therefore, the number of patients living with metastatic breast cancer is not known. Meeting the needs of an under-measured patient population is difficult, and as a result, feelings of abandonment and isolation are common among those living with the condition.
"Metastatic breast cancer remains poorly understood by the public, policymakers, and even health care professionals. Some patients have told me that they feel ‘written off’. This sense of being ignored and left behind can mean they are less likely to seek help or engage with research that could help them."
Lesley Stephen, collaborator and patient advocate
Lesley added: "Patients with metastatic disease need more support and information in order to feel valued."
In the last decade, metastatic breast cancer outcomes have improved considerably. The median overall survival for the two major subtypes, which include approximately 85% of metastatic breast cancer patients, has reached five years where recommended therapies are made available. In a Commission survey of 382 healthcare professionals, more than half (55%) agreed that specific subtypes of metastatic breast cancer may become curable, and three-quarters agreed that it will become a chronic disease.
The authors make a case for a minimum of 70% of registries worldwide to record cancer stage and relapse. These data could drive significant improvements in metastatic breast cancer care, outcomes, and emotional wellbeing among patients. Initiatives that promote societal inclusion of people living with metastatic breast cancer are also paramount; for example, changes to labour market laws that empower more flexible working arrangements. With a shift in perception, it may be possible to treat most, alleviate suffering for all, and forget no-one living with the disease, the Commission argues.
The hidden costs of breast cancer
The associated costs of breast cancer – including physical, psychological, social, and financial costs – are immense but under-recognised. Many of these costs are not captured by current global health metrics.
In response, the Commission established a UK-based pilot study that provides a snapshot of the economic burden and supportive care needs for people affected by breast cancer. Nearly all of the 606 people living with breast cancer and carers surveyed by the Commission stated physical or well-being issues related to breast cancer. One participant described losing their job as as result of being unable to cope during chemotherapy, while another experienced sexual dysfunction but found it difficult to ask for help.
Additionally, a fifth of participants with early breast cancer and a quarter of those with metastatic breast cancer reported difficulty in covering the costs of travel for treatment. 27% with early breast cancer and 35% with metastatic breast cancer said they had financial problems.
This pilot research suggests that, even in countries with a health care system free at the point of care, people with breast cancer can incur hidden costs.
Building on previous work, the Commission report also discusses serious health-related suffering, an indicator of the need for palliative care, with estimates provided by a small expert group. In 2020, an estimated 120 million days were spent with serious health-related suffering per year for people who died of their cancer. A further 520 million days were estimated for patients living with the disease. Behind these numbers are individuals experiencing pain, shortness of breath, fatigue, and other, often resolvable, distressing symptoms.
"Even in countries with well-developed health care systems, patients with breast cancer experience inadequate support and care. In countries lacking affordable health care facilities, patients experience these costs more commonly and intensely, too often leading to catastrophic spending and impoverishment."
Dr Carlos Barrios, Oncology Research Center, Hospital São Lucas, Brazil
The Commission advocates the development of new tools and metrics that capture the many costs associated with the disease. This measurement should guide policymakers to invest in breast cancer prevention, early detection, cost-effective therapy, optimal management, financial protection, and other interventions that relieve suffering.

Better communication for better patient outcomes
Many patients describe breast cancer as robbing them of power. Therefore, healthcare professional-patient communication that empowers is highlighted by the authors as an important intervention. A review of research by the Commission suggests better communication with patients can improve quality of life, decision-making, body image, and even adherence to therapy – with positive impacts on survival.
"Improving the quality of communication between patients and health professionals, though seemingly simple, could have profound positive impacts that extend far beyond the specific setting of breast cancer management."
Professor Reshma Jagsi, Emory University School of Medicine, USA
Professor Jagsi added: "Patients should be encouraged to exercise their voices, choosing their level of involvement in care decisions."
The Commission calls for every healthcare professional in every country to receive communication skills training and for patient involvement in all stages of clinical research on breast cancer – from concept to translation into clinical practice. To support these transitions, the report outlines a framework based on strategies to build rapport and empathy, share information, check understanding, and jointly agree next steps with patients.
Collaborate to improve prevention and early detection
Up to a quarter of breast cancer in high income countries could be prevented by modifying risk factors for breast cancer. While education and awareness-raising efforts are important in this respect, bold policy changes that minimise population exposure to modifiable risk factors (including alcohol consumption, being overweight, and physical inactivity) are vital to reduce cancer incidence, suggests the Commission.
In addition, systematic approaches that identify those at increased risk of the disease are essential to enable equitable access to personalised prevention strategies, including cheap and effective medications that can avert breast cancer for many women.
The authors also argue for improved early detection programmes, beginning with efforts to promote stage shifting in diagnosis so that at least 60% of confirmed invasive cancers are early disease (stages one or two).
"Access to evidence-based prevention and care that isn’t dependent on where an individual lives or their ability to pay would reap wide-ranging benefits for patients, families, and health care systems striving to achieve universal health coverage."
Professor Benjamin Anderson, Departments of Surgery and Global Health, University of Washington, USA

Published 16 April 2024
Adapted from a press release by The Lancet.
Reference Coles, CE et al. The Lancet Breast Cancer Commission . Lancet; 15 Apr 2024; DOI: 10.1016/S0140-6736(24)00747-5
- Woman in white bath towel holding her hair (National Cancer Institute/Unsplash)
- Professor Charlotte Coles (Patrick Harrison/Cancer Research UK)
- Young breast cancer patient (Rebekah Voz/Unsplash)
- Oncology Portrait - stock photo (FatCamera/Getty Images)
- Asian woman with cancer meeting with female physician - stock photo (FatCamera/Getty Images)
- Nurse with young women having a mammography - stock photo (choja/Getty Images)

Relay for Life returns to campus, raises $15,000 for cancer research
- April 16, 2024
- Elizabeth Scoone , Kyle Quinlan and Nathan Mader
Paper bags filled the Siebert Hall lawn Sunday, each representing someone who died from cancer.
Over 100 people lit candles in each of the bags and drew encouraging pictures as part of the American Cancer Society Buckeye chapter’s annual Relay for Life, which had been paused since 2019 due to the pandemic. This year, the event raised more than $15,000, with proceeds dedicated to fund cancer research.
“As a community, every step taken and every dollar raised helps the American Cancer Society fight cancer on all fronts,” said Rahaf Shalash, Relay for Life event lead, member of the Buckeye chapter and a third-year in human nutrition. “While each of us has a unique reason for being here, we all have something very much in common. We want to make a difference in the fight against cancer and we are doing that, you all are doing that.”
Participants walked around the lawn twice, once as a dedication for survivors and the second for supporters and caregivers. Cancer survivors shared their personal battles, including Brenda George, a thyroid cancer survivor who has since dedicated her time to advocate for cancer research as a Voice of Hope Speaker with the American Cancer Society.
“Leading the fight for a world without cancer will take power, courage, time, money and sacrifice, just like it does to survive cancer,” George said. “But it is possible.”
Prior to the walk, George offered words of inspiration to the participants.
“You might feel weak today, but the fire within you — your passion, your determination, your strength, your courage, even on the days that seem overwhelmingly defeating — that is going to rule the fire within you and enable you to rise above this present situation and help you look to the future with hope and anticipation for better days to come,” George said.
Due to the challenges brought on by the COVID-19 pandemic, Isabelle Castillo-Anderson, a senior development manager at the American Cancer Society, said the Buckeye chapter encountered difficulties in regaining momentum. However, the latest group of students stepped up to the plate, working to promote the event through fundraising, networking and initiatives such as making blankets for cancer patients.
“We launched this committee of students late last semester, so within these last three to four months [we have gone] from nothing to building out that awareness and presence back on campus,” Castillo-Anderson said.
Castillo-Anderson said this allowed participants to celebrate, remember, fight back and honor the people lost to cancer. This allowed people to connect with others affected by cancer, said Yusuf Rasheed, a third-year in biology and president of the group’s Buckeye chapter.
“We’re all here for the same purpose. Over these next few hours, let’s fight as one community against our number one enemy, cancer,” Rasheed said.
These reasons contribute to why the group is defined as “more than just a walk,” according to the American Cancer Society website .
Related Posts

Columbus-based artist Befriend Strange Creatures to release new EP and play celebratory house show Friday
Men’s tennis: no. 1 buckeyes dominate michigan, remain atop big ten standings, opinion: search for kelly’s inside-zone quarterback continues as no man stands out at spring game.

Football: Running back room shows versatility and poise in spring game
Women’s lacrosse: buckeyes fall to no. 1 northwestern, marking fourth big ten loss, president ted carter reflects on first semester in q&a with the lantern.

Rock band Mamadog strives to create distinct sound, carve out niche in Columbus
Softball: buckeyes avoid shutout, ultimately lose northwestern series 1-2, comedic moments and lessons on mortality dominate the contemporary theatre of ohio’s take on ‘ride the cyclone’.
Search Our Jobs
Radius Miles 5 miles 15 miles 25 miles 35 miles 50 miles
Match Jobs with
Associate scientist, risk factors & screening research.
At the American Cancer Society, we're leading the fight for a world without cancer. Our employees and 1.5 million volunteers are raising the bar every single day. We actively seek candidates from diverse backgrounds including communities of color, the LGBTQ community, veterans, and people with disabilities. The greater the diversity of our people, the better we can serve our communities. The people who work at the American Cancer Society focus their diverse talents on our lifesaving mission. It is a calling. And the people who answer it are fulfilled.
MAJOR RESPONSIBILITIES
Conduct comprehensive literature reviews and analyze surveillance data from various public-use databases (including the behavioral risk factor surveillance system, youth risk behavior survey, national health interview survey, national health and nutrition examinations survey, cancer registries) as well as medical claims data to meet various cancer surveillance and screening activities including research projects for the peer-review literature., collaborate with colleagues on cancer screening, surveillance, and social determinants of health research projects to contribute to scientific literature., ensure the accuracy and consistency of data presented in facts & figures publication (e.g., proofreading text and data checking)., respond to requests for risk factors and screening data from acs staff, media, and the general public., write, test, and submit computer programs in sas, sudaan, and seer*stat to operate in a variety of computer environments (e.g. pc and local mainframe). efficient, logical, pre-tested programs are essential in large databases., prepare tables and figures for scientific presentations using excel, powerpoint and/or origin lab., document analytic programs and results in an organized, dated, and clearly labeled form for future reference., proofread reports for publication and presentation at professional meetings., co-author or author papers for publications in scientific journals., knowledge/skills, formal knowledge:, master’s degree or equivalent amount of experience and education in public health, statistics, or epidemiology., two year experience in statistical, medical, or biologic research., cancer screening, early detection, and risk factor surveillance, and survey research experience highly desirable, specialized training or knowledge:, good familiarity with sas or related statistical software (r, stata). quantiative skills and good knowledge of statistics., preferred: experience in analysis of survey data using sudaan; background in cancer epidemiology., familiarity with large database (nhis, brfss, seer, etc). , familiarity with fundamental principles of biology and health., good communication skills. attention to detail with numbers and calculations., direct supervision received:, reports to scientific director, risk factors & screening research., internal contacts: , close working relationships with staff in acs research departments, health equity, acs cancer action network, corporate communications/marketing, and acs regions., external contacts: , collaborators in universities, at the centers for disease control and prevention, the national cancer institute, the north american association of central cancer registries, and other relevant cancer surveillance organizations..
The American Cancer Society has adopted a vaccination policy that requires all staff, regardless of position or work location, to be fully vaccinated against COVID-19 (except where prohibited by state law).
ACS provides staff a generous paid time off policy; medical, dental, retirement benefits, wellness programs, and professional development programs to enhance staff skills. Further details on our benefits can be found on our careers site at: jobs.cancer.org/benefits. We are a proud equal opportunity employer.
Equal Opportunity Employer.
See our commitment to a policy of Equal Employment Opportunity to continually ensure equal opportunity to our employees and to our applicants.
Sign up for job alerts
Stay up-to-date about the latest career opportunities at American Cancer Society!
Email Address
- Discovery, Atlanta, Georgia, United States Remove
Confirm Email
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- NATURE PODCAST
- 05 April 2024
Audio long read: Why are so many young people getting cancer? What the data say
- Heidi Ledford &
- Benjamin Thompson
You can also search for this author in PubMed Google Scholar
Download the 05 April long read podcast
Around the world, rates of cancers that typically affect older adults are increasing in those under 50 years old. Models based on global data predict that the number of early-onset cancer cases like these will increase by around 30% between 2019 and 2030.
The most likely contributors — such as rising rates of obesity and early-cancer screening — do not fully account for the increase. To try and understand the reasons behind this trend, many researchers are searching for answers buried in studies that tracked the lives and health of children born half a century ago.
This is an audio version of our Feature Why are so many young people getting cancer? What the data say
Never miss an episode. Subscribe to the Nature Podcast on Apple Podcasts , Spotify or your favourite podcast app. An RSS feed for Nature Podcast is available too.
doi: https://doi.org/10.1038/d41586-024-00884-1
Related Articles

- Epidemiology
- Medical research

AI traces mysterious metastatic cancers to their source
News 17 APR 24

Biological age surges in survivors of childhood cancer
Research Highlight 11 APR 24

How to supercharge cancer-fighting cells: give them stem-cell skills
News 10 APR 24

Bird flu outbreak in US cows: why scientists are concerned
News Explainer 08 APR 24

Fungal diseases are spreading undetected
Outlook 14 MAR 24

Why are so many young people getting cancer? What the data say
News Feature 13 MAR 24

Blocking cell death limits lung damage and inflammation from influenza
News & Views 10 APR 24
Postdoctoral Research Associate position at University of Oklahoma Health Sciences Center
Postdoctoral Research Associate position at University of Oklahoma Health Sciences Center The Kamiya Mehla lab at the newly established Departmen...
Oklahoma City, Oklahoma
University of Oklahoma Health Sciences Center
Computational Postdoctoral Fellow with a Strong Background in Bioinformatics
Houston, Texas (US)
The University of Texas MD Anderson Cancer Center
Locum Associate or Senior Editor (Immunology), Nature Communications
The Editor in Immunology at Nature Communications will handle original research papers and work on all aspects of the editorial process.
London, Beijing or Shanghai - Hybrid working model
Springer Nature Ltd
Assistant Professor - Cell Physiology & Molecular Biophysics
Opportunity in the Department of Cell Physiology and Molecular Biophysics (CPMB) at Texas Tech University Health Sciences Center (TTUHSC)
Lubbock, Texas
Texas Tech University Health Sciences Center, School of Medicine
Postdoctoral Associate- Curing Brain Tumors
Baylor College of Medicine (BCM)
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
IMAGES
COMMENTS
Among children (14 years or younger) and adolescents (15 to 19 years), overall cancer death rates have declined by 70 percent and 64 percent, respectively, between 1970 and 2020, driven largely by improvements in treatment ( 2). Among the major advances made across the clinical cancer care continuum from August 1, 2022, to July 31, 2023, are 14 ...
Part 1 of the latest Annual Report to the Nation on the Status of Cancer was released on October 27, 2022. In addition to providing rates of new cases and deaths for the most common cancers in the United States, this year's report also examines trends in pancreatic cancer and its subtypes in detail.
According to the International Agency for Research on Cancer (IARC), in 2020 there were approximately 19.3 million new cases of cancer, and 10 million deaths by this disease, 6 while 23.8 million cases and 13.0 million deaths are projected to occur by 2030. 73 In this regard, it is clear the increasing role that environmental factors ...
Notably, cancer patients in the United States shouldered an economic burden of $21 billion in 2019 from out-of-pocket costs and other related expenses, which is nearly 3.5 times the amount of approximately $6 billion in NCI funding for cancer research in the same year Yabroff KR, et al. Annual Report to the Nation on the Status of Cancer, part ...
What is the objective of the report? The IARC World Cancer Report is the most comprehensive overview of relevant research yet available. This latest publication is part of a well-established series.Produced about every 5 years, World Cancer Report provides the latest evidence on cancer prevention and serves as an authoritative reference in the cancer research community.
Nature Cancer publishes research, reviews and comment across the spectrum of the cancer field, from fundamental preclinical, to translational and clinical work. ... A study reports that survivors ...
Nature Reviews Cancer publishes a dynamic and accessible mix of Reviews, Perspectives, Progress and Highlight articles on the most important primary research ...
Progress in Cancer Research. Basic, molecular, epidemiologic, and clinical research are leading to improved cancer prevention, screening, and treatment. Decreasing cancer mortality death rates and increasing numbers of cancer survivors are important indicators of the progress we have made. As the leader of the National Cancer Program, NCI has ...
World Cancer Reports are recognized as an authoritative source of global perspective and information on cancer, including cancer patterns, causes, biological processes, and prevention. The latest World Cancer Report, published in 2020, has a specific focus on cancer prevention and the recent research that underpins prevention, and includes a section on inequalities that affect the distribution ...
Targeted therapies have swiftly taken a prominent position in cancer research and clinical oncology in recent decades, thanks to the molecular insights into oncogenic processes and mechanisms ...
The new World Cancer Report will have six sections, each containing a number of chapters. An overview of each section is provided here. ... Research findings on cancer causation encompass new insights for both well-recognized carcinogens and those cancer-causing agents that have been recently described. A daunting aspect of research is the ...
The Third Expert Report builds on two previous global reports from 1997 and 2007. It offers a wealth of new overall information, provides more sophisticated analyses of cancer risk and exposure, and reflects shifts in the Expert Panel's interpretation of the gathered evidence. And even after publication, the work remains ongoing.
NCI is the nation's leader in cancer research. Learn about key research areas, initiatives, progress, and research tools, including specimens and data. ... The 2022 report includes data on new cancer cases and deaths plus a detailed examination of trends in pancreatic cancer and its subtypes.
F. Castinetti and F. Borson-ChazotN Engl J Med 2023;389:1916-1918. Although medullary thyroid cancer accounts for less than 5% of thyroid cancers, it deserves attention because of its phenotypic ...
World Cancer Report: Cancer Research for Cancer Prevention features the latest research from across multiple disciplines. It is aimed primarily at cancer researchers, academia, health professionals, and policy-makers, but this expert report remains accessible to a wider audience, including the general public, civil society, and the private sector.
Cancer, an international interdisciplinary journal of the American Cancer Society, publishes high-impact, peer-reviewed original articles and solicited content on the latest clinical research findings. Spanning the breadth of oncology disciplines, Cancer delivers something for everyone involved in cancer research, risk reduction, treatment, and ...
Cancer Reports is an international, open access oncology journal publishing basic, translational, clinical and interdisciplinary research in cancer biology, diagnosis, treatment, outcome, supportive care, epidemiology and health disparities. We encourage data-driven, scientifically valid findings, including incremental discoveries, pilot studies and more.
Organoid biology will further develop with a goal of translating the research into personalized therapy. These research areas may result in the creation of new cancer treatments in the future. Keywords: exosomes, immunotherapy, microbiome, organoid. Cancer research has made remarkable progress and new discoveries are beginning to be made.
Top 100 in Cancer - 2022. This collection highlights our most downloaded* cancer papers published in 2022. Featuring authors from aroud the world, these papers showcase valuable research from an ...
Extracellular vesicles for cancer diagnosis and therapy. EVs are classified in two categories based on their biogenesis. Specifically, exosomes are small vesicles of around 30-150 nm originated from endosomes in physiological and pathological conditions and released by a fusion of multivesicular bodies (MVBs) to the cell membrane [55, 56], while shed microvesicles (sMVs), with a typical size ...
Roussos-Torres and colleagues perform a phase Ib clinical trial of entinostat, nivolumab and ipilimumab in individuals with advanced HER2-negative breast cancer, report on safety and response and ...
Prostate cancer is the most common cancer in men in 112 countries, and accounts for 15% of cancers. In this Commission, we report projections of prostate cancer cases in 2040 on the basis of data for demographic changes worldwide and rising life expectancy. Our findings suggest that the number of new cases annually will rise from 1·4 million in 2020 to 2·9 million by 2040.
Cancer Research UK Lung Cancer screening project. This report presents the data from the 2022 Lung Cancer Screening survey, led by Cancer Research UK (CRUK), conducted by YouGov and with the costs of the project covered by ScottishPower. This piece of research aims to inform CRUK's work in the lung cancer space.
This pilot research suggests that, even in countries with a health care system free at the point of care, people with breast cancer can incur hidden costs. Building on previous work, the Commission report also discusses serious health-related suffering, an indicator of the need for palliative care, with estimates provided by a small expert group.
This report is in response to House Report 117-88, pages 329-330, accompanying H.R. 4432, the Department of Defense Appropriations Bill, 2022, which directs the Assistant Secretary of Defense for Health Affairs to provide a report to the congressional defense committees on the status of the Peer-Reviewed Cancer Research Program (PRCRP).
National Coffee Association President and CEO William Murray said banning European Method decaf coffee — the type that uses methylene chloride — "would defy science and harm American's ...
Tubulin alpha-1b chain was identified as a prognosis and immune biomarker in pan-cancer combing with experimental validation in breast cancer. Yiyang Wang. , Yongxiang Li. & Chenming Guo. Article ...
April 16, 2024. Elizabeth Scoone, Kyle Quinlan and Nathan Mader. Relay for Life returns to campus, raises $15,000 for cancer research. Watch on. Paper bags filled the Siebert Hall lawn Sunday ...
The incumbent will join the Risk Factors & Screening Research team within the Surveillance & Health Equity Science (SHES) Department of the American Cancer Society (ACS). Primary responsibilities include updating the biennial Cancer Prevention & Early Detection (CPED) Facts & Figures; provide analytical support to Scientific Director of Risk ...
Download the 05 April long read podcast. Around the world, rates of cancers that typically affect older adults are increasing in those under 50 years old. Models based on global data predict that ...