Why global health equity matters for all and what organizations can do to advance it

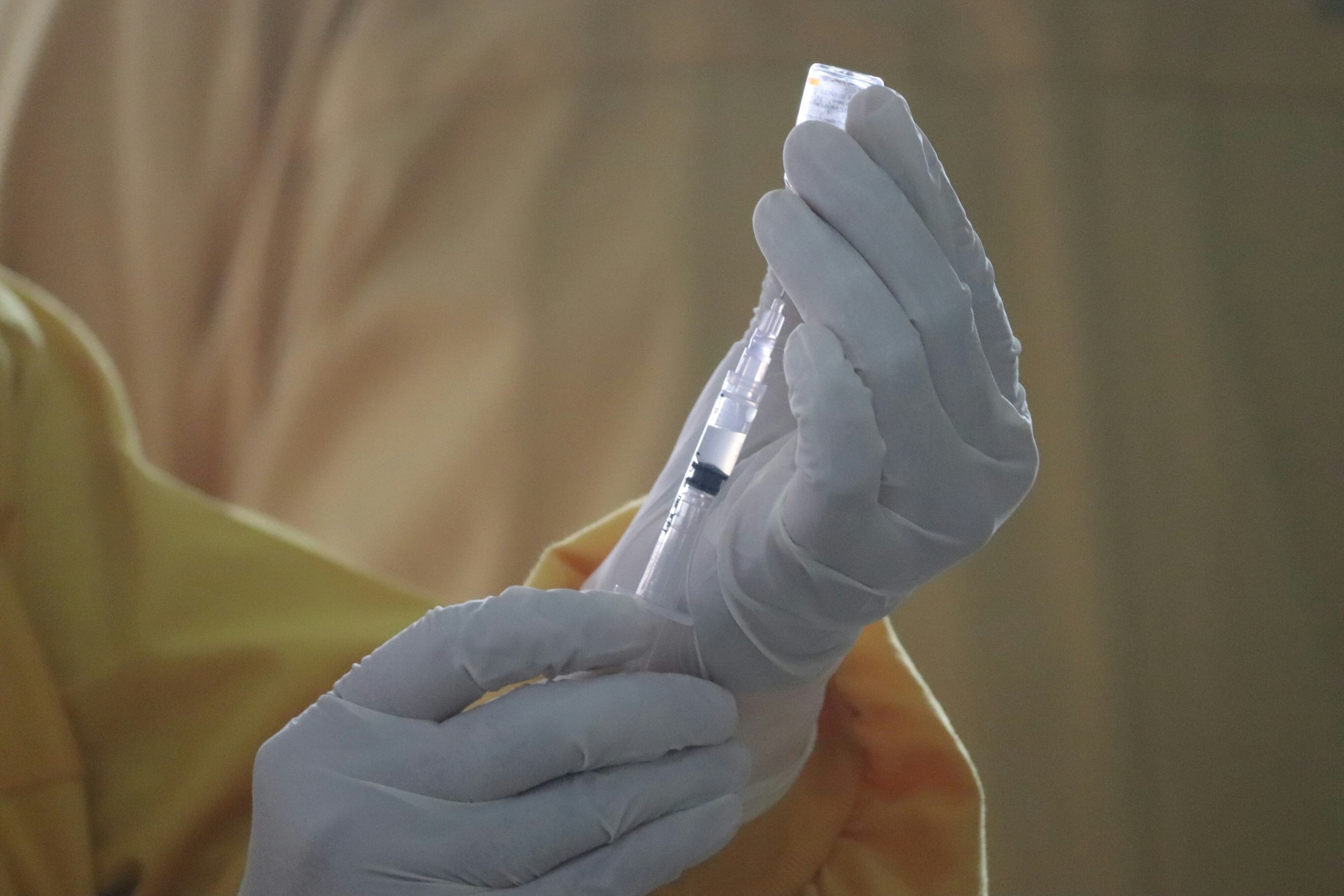
The pursuit of health equity is not just a moral obligation but also a strategic imperative. Image: Unsplash/CDC

.chakra .wef-1c7l3mo{-webkit-transition:all 0.15s ease-out;transition:all 0.15s ease-out;cursor:pointer;-webkit-text-decoration:none;text-decoration:none;outline:none;color:inherit;}.chakra .wef-1c7l3mo:hover,.chakra .wef-1c7l3mo[data-hover]{-webkit-text-decoration:underline;text-decoration:underline;}.chakra .wef-1c7l3mo:focus,.chakra .wef-1c7l3mo[data-focus]{box-shadow:0 0 0 3px rgba(168,203,251,0.5);} Burgess Harrison
.chakra .wef-9dduvl{margin-top:16px;margin-bottom:16px;line-height:1.388;font-size:1.25rem;}@media screen and (min-width:56.5rem){.chakra .wef-9dduvl{font-size:1.125rem;}} Explore and monitor how .chakra .wef-15eoq1r{margin-top:16px;margin-bottom:16px;line-height:1.388;font-size:1.25rem;color:#F7DB5E;}@media screen and (min-width:56.5rem){.chakra .wef-15eoq1r{font-size:1.125rem;}} Health and Healthcare is affecting economies, industries and global issues

.chakra .wef-1nk5u5d{margin-top:16px;margin-bottom:16px;line-height:1.388;color:#2846F8;font-size:1.25rem;}@media screen and (min-width:56.5rem){.chakra .wef-1nk5u5d{font-size:1.125rem;}} Get involved with our crowdsourced digital platform to deliver impact at scale
Stay up to date:, health and healthcare.
- The imperative for global health equity has never been more acute.
- Diseases know no boundaries, and our efforts to combat them must transcend borders, cultures and socio-economic divides.
- By championing health equity, we uplift the most vulnerable and marginalized and strengthen our global community against future health-related challenges.
In an era where the global expenditure on healthcare eclipses $8 trillion annually , a stark paradox emerges.
The World Health Organization (WHO) underscores a monumental investment in health, yet a growing wave of indifference threatens to undermine the fabric of our interconnected health ecosystem. As nations navigate the turbulence of polarization and isolationism, the imperative for global health equity has never been more acute. Here, I dive into the essence of health equity, its universal importance and the actionable steps organizations can undertake to champion this cause.
Global health equity: a collective mission
The COVID-19 pandemic served as a harrowing reminder of our shared vulnerability. It demonstrated unequivocally that the health of the individual is inextricably linked to the global health network. Diseases know no boundaries, and as such, our efforts to combat them must also transcend borders, cultures and socio-economic divides. The pandemic highlighted that indifference towards the health and well-being of communities, both domestically and internationally, can have cascading effects, underscoring the essence of health equity.
The rising tide of indifference
In the United States, resistance to initiatives aimed at fostering health equity is on the rise. Certain states have been at the forefront of opposing affirmative action, diversity, equity, inclusion (DE&I) and health equity programmes. This growing resistance is a microcosm of a larger global trend of retracting into silos, which poses a significant threat to the pursuit of global health equity.
The Global Health and Strategic Outlook 2023 highlighted that there will be an estimated shortage of 10 million healthcare workers worldwide by 2030.
The World Economic Forum’s Centre for Health and Healthcare works with governments and businesses to build more resilient, efficient and equitable healthcare systems that embrace new technologies.
Learn more about our impact:
- Global vaccine delivery: Our contribution to COVAX resulted in the delivery of over 1 billion COVID-19 vaccines and our efforts in launching Gavi, the Vaccine Alliance, has helped save more than 13 million lives over the past 20 years .
- Davos Alzheimer's Collaborative: Through this collaborative initiative, we are working to accelerate progress in the discovery, testing and delivery of interventions for Alzheimer's – building a cohort of 1 million people living with the disease who provide real-world data to researchers worldwide.
- Mental health policy: In partnership with Deloitte, we developed a comprehensive toolkit to assist lawmakers in crafting effective policies related to technology for mental health .
- Global Coalition for Value in Healthcare: We are fostering a sustainable and equitable healthcare industry by launching innovative healthcare hubs to address ineffective spending on global health . In the Netherlands, for example, it has provided care for more than 3,000 patients with type 1 diabetes and enrolled 69 healthcare providers who supported 50,000 mothers in Sub-Saharan Africa.
- UHC2030 Private Sector Constituency : This collaboration with 30 diverse stakeholders plays a crucial role in advocating for universal health coverage and emphasizing the private sector's potential to contribute to achieving this ambitious goal.
Want to know more about our centre’s impact or get involved? Contact us .
Championing health equity in challenging environments
Despite these challenges, there is a path forward. Organizations and leaders have a pivotal role in advocating for and implementing strategies promoting health equity. By embracing innovative solutions and harnessing diverse voices, businesses can contribute significantly to this global endeavour.
The pursuit of health equity is not just a moral obligation. It is also a strategic imperative that benefits both the global population and the business community.
The role of businesses in promoting health equity
Businesses wield considerable influence and resources, which can be mobilized to champion the cause of health equity. They can make a substantial impact through corporate social responsibility (CSR) initiatives, public-private partnerships and investments in health technology. And by prioritizing the health and well-being of all stakeholders, businesses contribute to a more equitable world and enhance their resilience and sustainability.
Have you read?
How investors can bolster global health equity while generating long-term value, how poor oral health impacts health equity , how cloud computing is helping close the health equity gap, introducing health — it's about you too.
To galvanize action and foster a culture of health equity, we have created the monthly feature, Health — it's about you, too . This initiative will explore various aspects of global health, sharing stories that highlight our interconnectedness and the importance of collective well-being.
Utilizing the acronym H.E.A.L.T.H— Hope, Education, Advocacy, Leadership, Technology, Humanity: it will highlight the role of hope and humanity in health, advocate for education and leadership in health initiatives and leverage technology for better health outcomes. We will delve into the critical dimensions of health equity without divisive language, inspiring individuals, communities and organizations to take meaningful action.
Each month, the feature will spotlight a different theme, providing insights, case studies and actionable steps for engagement. Through the universal language of art and storytelling, we aim to communicate the urgency of health equity in an engaging and comprehensive manner.
Public, private partnerships and nonprofit collaborative action is being taken as exemplified by:
Health is for EveryBODY™ : from the National Minority Health Association (NMHA) and Sage Growth Partners (SGP) and over 30 organizations highlighting the fact that globally, when it comes to health, we are all in it together with two days of focus: January 4 th was One for All day, and April 1 st is All for One day.
The HEART Framework : Rhia Ventures’ Health Equity Assessment and Rating Tool (HEART Framework), adapted from the Racial Equity Assessment Lab (REAL) Framework , was developed as a standardized approach to identifying where organizations (e.g., investors, nonprofits, startup companies, etc.) are positioned on their journey towards advancing health equity.
The World Economic Forum’s Zero Health Gap Pledge: All organizations have a role in advancing health equity and eliminating disparities in health and wellbeing outcomes between and within countries. The Zero Health Gaps Pledge is a commitment from CEOs across industries and regions for their organizations to play their part by embedding health equity in core strategies, operations, and investments.
Equity for All: Lupus : An NMHA health awareness campaign to address issues faced by people living with systemic lupus erythematosus (SLE ) . This effort is supported by the Global Healthy Living Foundation , HealthFirst , Lupus Research Alliance , Biogen and UCB .
CEO Action for Racial Equity : This fellowship is a first-of-its-kind, business-led initiative working to advance racial equity through public policy. It's a Path to Progress , bringing business, communities and policy together to drive change. Through corporate and community engagement, the fellowship is fighting societal systemic racism by advancing racial equity through public policy at the federal, state and local levels. Our focus is to positively impact the 47+ million Black Americans and improve societal well-being.
American Kidney Fund Health Equity Coalition : In the US, Black and Hispanic people fare worse with kidney disease than White people. Black and Hispanic people are more likely to develop kidney failure and are less likely to receive a kidney transplant . It doesn't have to be this way. The American Kidney Fund programmes put solutions into practice that help break down common barriers — so that everyone can equally prevent and get treatment for kidney disease.
American Epilepsy Society Disrupting Disparities Advisory Committee : This project aims to improve outcomes for underserved people with epilepsy by improving the epilepsy clinical knowledge of the non-specialist epilepsy care workforce and deepening understanding of social determinants of health and commitment to epilepsy self-management by the epilepsy specialist workforce.
HLTH Foundation Techquity: The HLTH Foundation launched Techquity for Health a coalition to help integrate health equity standards into healthcare technology and data practices.
Digital Medicine Society : (DiMe) brings a team together in a health equity coalition.
These are a few examples of the collaborative efforts being made to address health equity.
A call to action
The journey towards global health equity is a collective endeavour that requires the concerted effort of individuals, communities and organizations worldwide. We can build a healthier, more equitable world for future generations by fostering a culture of empathy, access and trust. It's not just about the health of the individual but about the well-being of humanity at large. Let us embrace our shared responsibility and act with the urgency and solidarity that global health equity demands.
The domino effect of global health equity can be profound. One small action or effort can often create the energy for change. It reminds us that our actions or inactions have far-reaching consequences. By championing health equity, we not only uplift the most vulnerable and marginalized among us but also strengthen our global community against future health-related challenges. Any business, government or organization can begin to work together to ensure that health equity is not just an ideal but a reality for all. As evidenced by the collaborative efforts underway and in the immortal words of Nike®, when it comes to health equity — Just do it.
Don't miss any update on this topic
Create a free account and access your personalized content collection with our latest publications and analyses.
License and Republishing
World Economic Forum articles may be republished in accordance with the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International Public License, and in accordance with our Terms of Use.
The views expressed in this article are those of the author alone and not the World Economic Forum.
The Agenda .chakra .wef-n7bacu{margin-top:16px;margin-bottom:16px;line-height:1.388;font-weight:400;} Weekly
A weekly update of the most important issues driving the global agenda
.chakra .wef-1dtnjt5{display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-align-items:center;-webkit-box-align:center;-ms-flex-align:center;align-items:center;-webkit-flex-wrap:wrap;-ms-flex-wrap:wrap;flex-wrap:wrap;} More on Health and Healthcare Systems .chakra .wef-17xejub{-webkit-flex:1;-ms-flex:1;flex:1;justify-self:stretch;-webkit-align-self:stretch;-ms-flex-item-align:stretch;align-self:stretch;} .chakra .wef-nr1rr4{display:-webkit-inline-box;display:-webkit-inline-flex;display:-ms-inline-flexbox;display:inline-flex;white-space:normal;vertical-align:middle;text-transform:uppercase;font-size:0.75rem;border-radius:0.25rem;font-weight:700;-webkit-align-items:center;-webkit-box-align:center;-ms-flex-align:center;align-items:center;line-height:1.2;-webkit-letter-spacing:1.25px;-moz-letter-spacing:1.25px;-ms-letter-spacing:1.25px;letter-spacing:1.25px;background:none;padding:0px;color:#B3B3B3;-webkit-box-decoration-break:clone;box-decoration-break:clone;-webkit-box-decoration-break:clone;}@media screen and (min-width:37.5rem){.chakra .wef-nr1rr4{font-size:0.875rem;}}@media screen and (min-width:56.5rem){.chakra .wef-nr1rr4{font-size:1rem;}} See all

This Earth Day we consider the impact of climate change on human health
Shyam Bishen and Annika Green
April 22, 2024

Scientists have invented a method to break down 'forever chemicals' in our drinking water. Here’s how
Johnny Wood
April 17, 2024

Young people are becoming unhappier, a new report finds

Promoting healthy habit formation is key to improving public health. Here's why
Adrian Gore
April 15, 2024

What's 'biophilic design' and how can it benefit neurodivergent people?
Fatemeh Aminpour, Ilan Katz and Jennifer Skattebol
Why stemming the rise of antibiotic resistance will be an historic achievement
Carel du Marchie Sarvaas
April 11, 2024
- Search Menu
- Advance Articles
- Editor's Choice
- Supplements
- Open Access Articles
- Research Collections
- Review Collections
- Author Guidelines
- Submission Site
- Open Access Options
- Self-Archiving Policy
- About Health Policy and Planning
- About the London School of Hygiene and Tropical Medicine
- HPP at a glance
- Editorial Board
- Advertising and Corporate Services
- Journals Career Network
- Journals on Oxford Academic
- Books on Oxford Academic
Article Contents
Introduction, conclusions and recommendations, acknowledgements, the effects of global health initiatives on country health systems: a review of the evidence from hiv/aids control.
- Article contents
- Figures & tables
- Supplementary Data
Regien G Biesma, Ruairí Brugha, Andrew Harmer, Aisling Walsh, Neil Spicer, Gill Walt, The effects of global health initiatives on country health systems: a review of the evidence from HIV/AIDS control, Health Policy and Planning , Volume 24, Issue 4, July 2009, Pages 239–252, https://doi.org/10.1093/heapol/czp025
- Permissions Icon Permissions
This paper reviews country-level evidence about the impact of global health initiatives (GHIs), which have had profound effects on recipient country health systems in middle and low income countries. We have selected three initiatives that account for an estimated two-thirds of external funding earmarked for HIV/AIDS control in resource-poor countries: the Global Fund to Fight AIDS, TB and Malaria, the World Bank Multi-country AIDS Program (MAP) and the US President's Emergency Plan for AIDS Relief (PEPFAR). This paper draws on 31 original country-specific and cross-country articles and reports, based on country-level fieldwork conducted between 2002 and 2007. Positive effects have included a rapid scale-up in HIV/AIDS service delivery, greater stakeholder participation, and channelling of funds to non-governmental stakeholders, mainly NGOs and faith-based bodies. Negative effects include distortion of recipient countries’ national policies, notably through distracting governments from coordinated efforts to strengthen health systems and re-verticalization of planning, management and monitoring and evaluation systems. Sub-national and district studies are needed to assess the degree to which GHIs are learning to align with and build the capacities of countries to respond to HIV/AIDS; whether marginalized populations access and benefit from GHI-funded programmes; and about the cost-effectiveness and long-term sustainability of the HIV and AIDS programmes funded by the GHIs. Three multi-country sets of evaluations, which will be reporting in 2009, will answer some of these questions.
Global health initiatives (GHIs) have enabled wider stakeholder participation in service delivery while often having early negative systems effects through establishing parallel bodies and processes that are poorly coordinated, harmonized and aligned with national systems.
Over time, GHIs have learned to better utilize country systems and support national disease control efforts, while making least progress in enabling countries to implement coordinated financial management and human resource strategies.
Independent longitudinal evaluations of GHIs are needed—especially at district, facility and community levels—to track developments and provide timely information to recipient countries, GHIs, civil society organizations and development agencies.
The past 10 years have witnessed a proliferation of what are commonly called global health initiatives (GHIs). They were put in place as an emergency response to accelerate the scale-up of control of the major communicable diseases, especially HIV/AIDS. GHIs are characterized by their ability to mobilize huge levels of financial resources, linking inputs to performance; and by the channelling of resources directly to non-governmental civil society groups (Caines 2005 ). Three GHIs—the World Bank's Multi-country HIV/AIDS Programme (MAP), the Global Fund to Fight AIDS, TB and Malaria, and The President's Emergency Plan For AIDS Relief (PEPFAR) (see Table 1 for main features)—are contributing more than two-thirds of all direct external funding to scaling up HIV/AIDS prevention, treatment and care in resource-poor countries (GFATM 2007 ; Oomman et al . 2007 ). They have leveraged high-level political support for HIV/AIDS at the global level and captured the attention of country-level stakeholders.
Main characteristics and HIV/AIDS commitments from the three GHIs (in millions of constant US$)
* Sources : OECD CRS database (last accessed 20 November 2008), Oomman et al . ( 2007 ).
Surprisingly, predictions that GHIs were likely to have profound effects on recipient country health systems (Brugha and Walt 2001 ) remain only partially explored (Brugha 2008 ; Yu et al . 2008 ), and speculation rather than systematic review of evidence characterizes current understanding of this major shift towards disease-specific funding, and its impact on health systems in recipient countries. Analysis has focused most closely on the Global Fund, and where analysis has been conducted on MAP and PEPFAR, lessons learned have not been collated and widely disseminated. The purpose of our review, therefore, is to systematically review, discuss and make recommendations for global and country policy makers around future evidence needs, based on available empirical data from countries on the specific effects on country health systems of these three GHIs.
In this review, we follow Brugha ( 2008 ) where, based on functions rather than governance structure, a GHI is defined as: ‘a blueprint for financing, resourcing, coordinating and/or implementing disease control across at least several countries in more than one region of the world’. According to this definition, GHIs may be bilateral agency—government to government—aid mechanisms, as in the case of PEPFAR; they can be established by a multilateral agency, as in the case of the World Bank's MAP; or they may be public-private partnerships, as in the case of the Global Fund. What characterizes them as GHIs is that they use uniform approaches to applying large levels of resources for HIV/AIDS control across a range of different countries and regions. 1 Our analysis of the effects of GHIs on country health systems focuses primarily on the effects that they have on those organizations, institutions and resources that produce actions whose primary purpose is to improve health (WHO 2000), which includes public, non-profit and for-profit private sectors, as well as international and bilateral donors, foundations and voluntary organizations involved in funding or implementing health activities at central, regional, district, community and/or household levels (Islam 2007 ).
Search strategy
In late 2007, we conducted a review of key documents, initially using as search terms research themes derived from a three-country study of the effects of the Global Fund (Stillman and Bennett 2005 ) and a draft of a policy review on GHIs (Brugha 2008 ). These themes and the names of the three selected GHIs were used as search terms for conducting a comprehensive search of six databases (AIDS Portal, CAB Direct, ELDIS, POPLINE, PubMed, and Web of Knowledge) for the period 2002–07. 2 We also performed internet searches for grey literature, reviewing the websites of three global health organizations (The World Bank's Independent Evaluation Group, the Global Fund Evaluation Library, and PEPFAR), and the research archives of three global health research institutes (Centre for Global Development, the UK Department for International Development Health Resource Centre, and Partnerships for Health Reform). Additional publications were obtained through reference lists of identified papers and by contacting key informants in the field.
Criteria for selection
Three authors examined the list of references generated by the search and independently assessed the retrieved studies for inclusion using the following criteria: This review does not include broad overviews of secondary material or ‘grey’ literature (for example, policy briefs, media or journal ‘comments’). We excluded studies restricted to data collection only at the global level, those based only on secondary data, and reviews and commentaries. This was sometimes a difficult judgement as some important reviews contained or cited some relevant primary data, but were excluded if these could not be directly sourced from papers or reports in the public domain.
Reports and papers must provide data about one or more of the key research themes as it relates to one or more of the three HIV/AIDS GHIs: Global Fund, PEPFAR or World Bank MAP;
Reports and papers must present primary data collected at the country level;
There must be some outline of methods, i.e. some explanation of how data were collected and analysed and how findings were derived;
The data are ‘original’. This might take the form of (i) primary qualitative or quantitative research findings; and (ii) external or internal multi-country evaluations of one or more of the GHIs.
A health systems framework for GHIs
Drawing on the conceptual framework for analysing system-wide effects of the Global Fund developed by Bennett and Fairbank ( 2003 ) and selected national-level effects reported in a policy review (Brugha 2008 ), a draft health systems framework was developed. This was composed of three health system's functions: policy development, policy implementation and service delivery. Given the lack of published evidence, 2002–07, on the effects of these GHIs on focal and non-focal services, the framework was shortened and focused on specific themes under policy development and policy implementation. Policy development reflected global concerns around country ownership, harmonization and alignment of global initiatives with national priorities and policies, as expressed in the Paris Declaration on Aid Effectiveness (OECD 2005 ). Policy implementation explored four cross-cutting health systems themes: coordination and planning, stakeholder engagement, monitoring and evaluation, and human resources (see Table 2 ). As new studies provide additional evidence, the framework can be expanded to include GHI effects on infrastructure and availability of drugs and other equipment; on coverage, equity and access to services; and the effects on non-focal, non-GHI supported services. Under each of these themes, we first present and interpret negative effects, which often correspond with the early effects of the GHIs, followed by positive effects and lessons learned by GHIs across this period.
Framework for assessing the published effects of GHIs on national health systems
Adapted from the SWEF framework by Bennett & Fairbank ( 2003 ) and Brugha ( 2008 ).
Description of studies
Thirty-one reports, where data were collected between 2002 and 2007, met the inclusion criteria (see Table 3 ). Some were disseminated both as individual and as cross-country outputs, notably the four-country Global Fund Tracking Study and the four-country SWEF (System Wide Effects of the Fund) studies. All were descriptive cross-sectional studies. A limited number of studies in this review have collected data both at the national and sub-national level, notably the SWEF study in Georgia, Benin and Ethiopia (Curatio 2004 ; Banteyerga et al . 2006 ; Gbangbadthore et al . 2006 ) and some others (GFATM 2004 ; McKinsey 2005 ; Kelly et al . 2006 ). Most of the studies included in this review used mainly or wholly qualitative methods (in-depth interviews).
Included studies with main characteristics
GF = Global Fund.
National policy development
Alignment to national policy, plans and priorities for health.
Negative effects of all three GHIs were reported by most early studies, including examples of how GHIs distracted governments from coordinated efforts to strengthen health systems through distorting national priorities and through imposing donor implementation conditions (Brugha et al . 2004 ; Grace 2004 ; World Bank 2004 ; McKinsey 2005 ; Stillman and Bennett 2005 ). The Global Fund aims to support programmes that reflect local priorities and fit within existing country structures, but in practice the extent to which this occurred varied widely (Stillman and Bennett 2005 ). The Fund rejected Uganda's 2002 Round One cross-cutting systems-strengthening proposal, requiring Uganda to break it into disease-specific components (Donoghue et al . 2005a ). In response, the Government established a discrete project management unit, which it and its donor partners viewed in 2003 as a distortion of Uganda's policy of channelling all funds to support a coordinated national health sector strategy. Pressure from World Health Organization (WHO) consultants led to Tanzania applying for Global Fund support for an anti-retroviral treatment programme, in place of the government's priority to fund a programme on orphans and children (Starling et al . 2005a ). Concerns were reported about PEPFAR-imposed policy prescriptions such as disallowing grant recipients from providing counselling on abortion and promotion of abstinence-only prevention approaches (ITPC 2005 ). An evaluation commissioned by the US Congress reported that PEPFAR's commitment to country ownership had been undermined by its rigid budget allocations to specific control measures (Sepulveda et al . 2007 ). Oomman et al . ( 2007 ) reported that PEPFAR's funding allocations were remarkably consistent despite epidemiological and health systems’ differences across Mozambique, Uganda and Zambia. This suggested that global earmarks and donor conditionalities were driving funding allocations regardless of countries’ diseases, health needs and priorities.
GHI-imposed priorities and funding decisions also reflected country systems’ weaknesses. An evaluation of the World Bank MAP reported that its approach was undermined by countries lacking national plans that prioritized the components of an HIV/AIDS programme according to their importance or anticipated effectiveness (OED 2005 ). In the early years of MAP, most Ministries of Health had been slow to respond to the HIV epidemic and some felt disempowered by MAP's support to a multisectoral response which channelled funds to other ministries in the fight against AIDS (World Bank 2004 ). The World Bank's interim review found that governments’ multisectoral response to the MAP had been disappointing. The different ministries’ sectoral plans lacked inter-sectorality and had not moved beyond their own workplace interventions to consider programmes for their beneficiaries such as students (Education) and farmers (Agriculture). Despite these early concerns, MAP was evaluated in 2007 as having succeeded in promoting a multisectoral response over the course of its 7 years (Gorgens-Albino et al . 2007 ), which corresponded with positive findings from an independent study in Uganda (Donoghue et al . 2005b ) indicating that GHI approaches had promoted lesson-learning by governments.
Global Fund and PEPFAR have also reportedly learned lessons and modified their processes over time. Studies across 2002–07 suggest that the Global Fund was beginning to adapt its early approach to fit with countries’ priorities for aligning new funds with country systems. In 2006, it was seen as more supportive of Ethiopia's decentralization policies than in 2005 (Banteyerga et al . 2005 ; Banteyerga et al . 2006 ). A follow-up study in Benin showed that the Global Fund was becoming better aligned with Benin's policies on partnership, although the planning of activities remained top-down, which conflicted with bottom-up processes supported by national health policy (Gbangbadthore et al . 2006 ). The US evaluation reported that recipient governments perceived PEPFAR's Country Operational Plans as becoming better aligned with national plans over time (Sepulveda et al . 2007 ). In Mozambique, while PEPFAR remained outside of the Sector Wide Approach (SWAp) pooled mechanism for funding the health and HIV/AIDS sectors, its representatives did participate in the annual planning activities undertaken by the Ministry of Health and National AIDS Council (Oomman et al . 2007 ). In Ethiopia, PEPFAR was working with the government to align with its priorities, although it was channelling its funds to its preferred implementing partners (Banteyerga 2006 ).
Donor harmonization and aid mechanisms
Negative effects on donor harmonization were reported in the early years of the GHIs. Those such as the Global Fund that lacked a country presence were radically new financing mechanisms in the international aid architecture; and they had not agreed with partners about their respective roles and responsibilities (McKinsey 2005 ). Although all of these GHIs had stated their willingness to harmonize their activities with other partners, the reality was often different. For example, the World Bank's review of MAP recommended that it and other donors should adopt ‘The Three Ones’ principles of harmonization: one strategic framework, one national authority and one monitoring and evaluation system for HIV/AIDS (World Bank 2004 ). However, MAP projects themselves continued to burden government officials with extensive and complex procedural and reporting requirements (Oomman et al . 2007 ).
An early synthesis of studies compiled by the Global Fund reported little harmonization between the Global Fund and pre-existing planning and funding mechanisms, such as SWAps and joint interagency committees (GFATM 2004 ). Later, Wilkinson et al . ( 2006 ) reported variable experiences of the Global Fund across different countries. While it supported donor harmonization and alignment efforts in Cambodia, Nigeria and Namibia, it was reportedly undermining these efforts in Sri Lanka and Cameroon, through requiring separate reporting systems with associated transaction costs. PEPFAR's requirement of US Federal Drugs Administration approval of antiretroviral drugs has prevented it relying on the WHO prequalification for quality assurance on which most donors and countries rely (Sepulveda et al . 2007 ). Other barriers to harmonization and collective donor action have included PEPFAR's requirement that results be attributable to its inputs, and its lack of transparency and unwillingness to involve other donors in its own annual planning processes, which have been considered procurement-sensitive (Sepulveda et al . 2007 ).
There is evidence, over time, that the GHIs—especially the Global Fund—have learned lessons and begun to harmonize their approaches and align them with governments. Follow-up studies across 2004 and 2005 in Benin and Ethiopia, where the Global Fund and PEPFAR signed a memorandum of understanding, reported significant improvements in GHI harmonization (Stillman and Bennett 2005 ; Banteyerga 2006 ). The Global Fund's agreement in 2004 to allow its funds be channelled through Mozambique's SWAp, the Common Fund, was seen as a pioneering example of how disease-specific programmes can learn to adapt to and strengthen country systems (McKinsey 2005 ). In Mozambique, the World Bank MAP followed the Global Fund's lead, but PEPFAR remained outside of the SWAp as PEPFAR does not support Ministry of Finance fund management processes (McKinsey 2005 ; Oomman et al . 2007 ). However, despite not being able to contribute funds directly to the SWAp, it had become an active participant in donor partnerships that aimed to harmonize donor and country activities (Oomman et al . 2007 ).
The integration of Global Fund support into Malawi's SWAp to fund its integrated service delivery approach was perceived as positive for its sustainability (Mtonya and Chizimbi 2006 ). The MAP mainly focused its harmonization activities through National AIDS Councils (NACs), where it contributed to pooled-funding to the NAC's Integrated Annual Work Plan for 2003–2008 (Mtonya and Chizimbi 2006 ). In other countries, MAP has contributed funds to support implementation of Global Fund plans, and several MAP projects have implemented joint supervision missions (Gorgens-Albino et al . 2007 ).
Policy implementation
Coordination and planning structures.
The three-disease focus of the Global Fund has required the establishment of a new planning structure: the Country Coordination Mechanism (CCM); and coordination has continued to be a contentious issue for national planners (Wilkinson et al . 2006 ). The result has been duplication in planning for HIV/AIDS control, between CCMs and national AIDS councils. In Uganda, this led to competition between the MoH and the Uganda AIDS Commission for control and funds (Donoghue et al . 2005b ). In Malawi, it was reported that there were parallel planning structures for the NAC Integrated National Work Plan and the SWAp Programme of Work, which Global Fund support had aggravated (Mtonya and Chizimbi 2006 ). The McKinsey study ( 2005 ) found that in Tanzania and the Democratic Republic of Congo there were at least four committees overseeing HIV/AIDS control, with little communication between them about their activities. Respondents in Angola believed there were too many coordinating bodies that did not meet the country's needs (McKinsey 2005 ).
The World Bank, which endorsed the UNAIDS ‘Three Ones’ principles, had a simpler task in that it worked with existing national AIDS councils (OED 2005 ). However, several studies reported longstanding weaknesses in NACs, which have not provided consistent leadership and oversight (Donoghue et al . 2005a ; ITPC 2005 ; Starling et al . 2005a ). Their secretariats have often become implementation agencies rather than coordinators and facilitators (World Bank 2004 ). One three-country study reported that preparation of annual country operational plans, a condition of PEPFAR support, consumed considerable time and effort of recipient organizations in Uganda, Zambia and Mozambique (Oomman et al . 2007 ). While duplication of planning structures has persisted, some positive effects of GHIs on coordination and planning have been reported. In Malawi, after a USAID policy project study in 2004 had pointed to the multiplicity of HIV/AIDS coordinating structures, the Malawi Partnership Forum was created in 2005 as a central coordination structure overarching all existing mechanisms (Mtonya and Chizimbi 2006 ).
Coordination and planning processes
Several studies have reported systemic weaknesses in CCM governance, such as suboptimal communication between its members, and a lack of trust between government and non-government sectors (Brugha et al . 2004 ; Curatio 2004 ; Doupe 2004 ; GFATM 2004 ; Grace 2004 ; Brugha et al . 2005 ; Donoghue et al . 2005a ; ITPC 2005 ; Starling et al . 2005a ; Stillman and Bennett 2005 ; Kelly et al . 2006 ; Wilkinson et al . 2006 ). Often CCMs were too large and unwieldy, which detracted from efficient functioning (Doupe 2004 ; Grace 2004 ). Concerns emerged in 2004 about the degree of participation and the capacity of Mozambique's CCM to adapt to its new role in overseeing Principal Recipient activities, in that the two principal recipients of funding were bodies represented by the Chair and Vice-Chair of the CCM (Starling et al . 2005b ). Similar concerns were also reported in Uganda with regard to the CCM Chair influencing the selection of its own constituency as the principal recipient of funds (Donoghue et al . 2005b ). However, comparable evidence of the effects of the MAP and PEPFAR on planning processes is lacking, reflecting PEPFAR's lack of transparency; and because the World Bank has traditionally negotiated directly with government behind closed doors.
GHI requirements and feed-back have also had positive effects on planning capacity (McKinsey 2005 ). In Georgia and China, feedback on the country proposals enhanced their capacity to plan and anticipate future needs (Curatio 2004 ; van Kerkhoff and Szlezak 2006 ). In Angola, which had recently emerged from conflict and where the risk of HIV/AIDS transmission was increasing, Global Fund and World Bank support was seen as critical in identifying appropriate measures for control of the epidemic (McKinsey 2005 ).
Widening stakeholder involvement: engaging and funding civil society
All three GHIs, most visibly the Global Fund through its CCMs, have boosted stakeholder engagement. However, several negative early effects were reported, which stemmed partly from government responses to these new ways of working. In 2002–04, some governments were perceived to be controlling the Global Fund processes and marginalizing civil society (Brugha et al . 2004 ; Grace 2004 ). Several studies reported problems in CCM constituencies, such as reluctance by government-dominated CCMs to include strong non-governmental partners (including the private for-profit sector), strong advocates for communities living with AIDS, geographical representation and strong technical expertise (Curatio 2004 ; Doupe 2004 ; GFATM 2004 ; Brugha et al . 2005 ; Donoghue et al . 2005a ; ITPC 2005 ; Starling et al . 2005a ; Stillman and Bennett 2005 ; Kelly et al . 2006 ). As a result, the Global Fund introduced tighter conditions, stipulating that CCMs, which prepare proposals and apply for funds, must include these sectors (Wilkinson et al . 2006 ).
Despite early problems, GHIs have been more effective than other financing mechanisms in diversifying stakeholder participation and involving NGOs and faith-based organizations (FBOs), enabling them to gain direct access to financial resources (GFATM 2004 ; OED 2004 ; McKinsey 2005 ; Wilkinson et al . 2006 ). MAP has expanded the scope and range of FBO and community responses to the HIV epidemic (Gorgens-Albino et al . 2007 ; Oomman et al . 2007 ). However, little published evidence was found on how communities’ planning capacity was strengthened. PEPFAR's focus on civil society has been at the expense of building government capacity and through heavy use of US NGOs (Oomman et al . 2007 ). A follow-up survey in Benin showed that the Global Fund CCM had become more pro-active since the baseline survey by including a broader range of stakeholders (Gbangbadthore et al . 2006 ). In Malawi, Benin and Zambia, the new opportunities provided by the Global Fund strengthened public/private collaborations, through NGOs establishing umbrella organizations that helped to channel funds through principal recipients to sub-recipients (Donoghue et al . 2005a ; Mtonya et al . 2005 ; Smith et al . 2005 ; Stillman and Bennett 2005 ). This also served to improve the capacity of local district structures, local NGOs and community groups.
Widening stakeholder involvement: multiple funding channels
Several studies report that GHIs, which focus on the same diseases, channel funds through many different routes, both within and outside the public sector. While there are clear advantages to involving a greater diversity of actors, many countries have found it difficult to cope with the complexity. For example, in Angola MAP channelled funds through the Ministry of Planning rather than the Ministry of Health, which was the usual channel, and the Global Fund did so through the United Nations Development Programme, UNDP (McKinsey 2005 ). PEPFAR, on the other hand, has chosen to channel its funds outside the public sector, mainly through international (often US-based) NGOs. These NGOs then fund country-based civil society and faith-based groups (Oomman et al . 2007 ). There were concerns in South Africa, Uganda, Benin, Ethiopia and Malawi about the rapid growth of the NGO sector, where many new NGOs were seen as having limited capacity and were only weakly accountable (Donoghue et al . 2005b ; Bennett et al . 2006 ; Kelly et al . 2006 ). These studies concluded that too little attention was paid to strengthening community-level systems and to ensuring adequate regulation or quality control in the non-public sector. There has been minimal reported involvement of the private for-profit sector in GHI processes and in receipt of funds, apart from the Global Fund in Malawi where private clinics were allocated free antiretroviral drugs (Stillman and Bennett 2005 ).
Despite concerns about capacity, it has been accepted almost universally as a positive feature of the GHIs that they all have disbursed significant funds to civil society. The Global Fund mandated that 30% of all grants should be allocated to civil society groups (Wilkinson et al . 2006 ); and the SWEF and Tracking Studies reported early evidence that the Global Fund was achieving this objective (Banteyerga et al . 2005 ; Donohoe et al . 2005a ; Mtonya et al . 2005 ; Smith et al . 2005 ).
Disbursement, absorption and management of GHI funds: disbursement and absorptive capacity
From 2002 to 2007, countries reported that the combination of different fiscal years, the different disbursement mechanisms of the three GHIs and unpredictable disbursement had made it difficult for countries to draw down funds and integrate these resources into coordinated national plans (Brugha et al . 2004 ; Grace 2004 ; Stillman and Bennett 2005 ; McKinsey 2005 ; Wilkinson et al . 2006 ; Oomman et al . 2007 ). Tanzania experienced quite similar problems in drawing down MAP and later Global Fund money; and respondents commented on the lack of lesson-learning across GHIs (Starling et al . 2005a ). In the Global Fund Tracking Studies (2003–04) and baseline SWEF studies (2004–05), countries reported immense pressure due to the Global Fund's performance-based disbursement conditions (Brugha et al . 2004 ; Stillman and Bennett 2005 ). Such conditions were not seen as inherently wrong, but as compounding problems of low absorptive capacity due to weak country budgetary systems and incompatible donor systems (ITPC 2005 ; McKinsey 2005 ). In Ethiopia, weak government plans were seen as not providing a solid base for guiding Global Fund-supported activities (Banteyerga et al . 2005 ). In Laos, the Global Fund delayed disbursements until the country resolved its financial, monitoring and evaluation systems’ weaknesses (McKinsey 2005 ). Lack of a country presence (a key feature of the Global Fund), and the slowness of it and its global multilateral and bilateral partners to respond to the need for stronger technical support to countries, often delayed and impaired grant implementation (Wilkinson et al . 2006 ).
On the positive side, evidence has shown that over the years 2002–07, the three GHIs have significantly increased total aid flows in the areas of the focal diseases (Gorgens-Albino et al . 2007 ; Oomman et al . 2007 ; Sepulveda et al . 2007 ). GHIs have been achieving their objective of prioritizing and funding the control of major diseases that were previously under-resourced (McKinsey 2005 ). In Benin, the Global Fund raised the overall budget for health spending by about 15% (Gbangbadthore et al . 2006 ). In the early 2000s, MAP made large commitments to HIV and AIDS control in advance of other donors with US$1 billion being fully committed by 2004 (Gorgens-Albino et al . 2007 ). Since 2004, MAP funding has been more moderate, while the Global Fund and in particular PEPFAR have increased their funding dramatically, as reported for Mozambique, Uganda and Malawi (Oomman et al . 2007 ). PEPFAR has disbursed more quickly than the Global Fund and MAP, partly by working outside of and making little effort to build government systems, which have been slower to draw down funds than non-government recipients (Stillman and Bennett 2005 ; Oomman et al . 2007 ). However, PEPFAR has provided countries with the least flexibility in how funds could be used, whereas the Global Fund has been seen as willing to fund gaps (Oomman et al . 2007 ).
Disbursement, absorption and management of GHI funds: financial management
Several studies have reported GHI-imposed duplication and parallelism in financial and programmatic management systems and cycles, which have created fragmentation and increased the administrative burden for already overloaded staff (Brugha et al . 2004 ; Grace 2004 ; Brugha et al . 2005 ; McKinsey 2005 ; Stillman and Bennett 2005 ; Oomman et al . 2007 ). Although separate systems for financing were sometimes justified, GHIs differed in efforts to use existing systems and/or to improve the capacity of recipient organizations.
The stringent World Bank MAP requirements have often led to the establishment of new financial management systems rather than using standard government systems. However, the World Bank MAP projects have made progress in building reliable country systems for financial management. Specific project staff, who sit within government ministries, were hired to oversee grant implementation and to train government staff in MAP-specific procedures (Oomman et al . 2007 ). PEPFAR, in their function as an emergency response, required recipient organizations that were able to manage funding efficiently and implement fast. Often they have channelled funding outside of the government system, following PEPFAR-specific accounting and reporting procedures, while they relied on their recipient organizations to build the capacity of the government and other local organizations (Oomman et al . 2007 ). The Global Fund has continued to utilize an independent Local Fund Agent (LFA) financial management and audit model. However, evaluations of the LFA system reported that, in practice, LFAs have often not been well aligned with government systems. Frequently they have lacked programmatic skills and have been unable to mobilize and work in partnership with other country partners (Kruse and Claussen 2004 ; Euro Health Group 2007 ). Recently, the Global Fund has been aiming to strengthen its LFA system through providing more comprehensive tools and guidelines for recipient (and sub-recipient) organizations (Euro Health Group 2007 ). However, evaluations of GHIs across 2002–07 have reported little progress in reducing GHI systems’ duplications.
Monitoring and evaluation (M&E)
Parallel systems and processes established by new GHIs contravene the Paris Principles of Aid Effectiveness, often bypassing countries’ own systems, and result in avoidable transaction costs (McKinsey 2005 ). However, M&E requirements of GHIs have often not been streamlined and, as a result, it is generally reported in national studies that managers, at the national and district levels, have to prepare multiple M&E reports, in different formats and with different deadlines for the different donors of their programmes. In some cases, additional indicators have been required that were not part of countries’ own systems (McKinsey 2005 ).
PEPFAR, which operates outside government systems, has continued to use project approaches and expects reporting to be carried out according its formats (Oomman et al . 2007 ). Several studies reported contrasting perceptions of Global Fund alignment with existing country M&E systems (Brugha et al . 2005 ; Wilkinson et al . 2006 ). In Cambodia, Uganda and Cameroon, the use of Global Fund project-related monitoring tools undermined national programmes and the ‘Three Ones’ principle of a single M&E system.
The M&E emphasis of the first generation of the World Bank supported AIDS projects was on monitoring as opposed to evaluation, but was often poorly designed, under-implemented and under-supervised (OED 2005 ). Informants in Tanzania, Malawi, Uganda and Mozambique also expressed concern about weak local M&E capacity or weak systems for monitoring GHI funds and were sceptical of their countries’ ability to demonstrate that they had met agreed targets (Brugha et al . 2005 ). Consequently, GHIs were encountering weak M&E systems and putting in place GHI-specific measures to address these weaknesses.
Improvements over time have been reported in that GHIs have started to work with countries on developing and strengthening their M&E systems (McKinsey 2005 ). In Sri Lanka and Nigeria, Global Fund indicators fitted with the national programme indicators and national M&E activities (Wilkinson et al . 2006 ). The follow-up SWEF studies in Ethiopia and Malawi in 2005–06 reported some improvements in integration, alignment and performance assessment since the baseline studies, one year earlier (Stillman and Bennett 2005 ). Recently, the World Bank developed an operational guide for programme M&E and put in place M&E country assistance capacity in the form of the Global Monitoring and Evaluation Support Team (GAMET), based at the World Bank (Gorgens-Albino et al . 2007 ). Recent findings show that PEPFAR has been supporting building local capacity for collecting, synthesizing and reporting on HIV/AIDS data through skills training, development of health information systems, and technical assistance, although neglecting or avoiding the strengthening of national systems (Sepulveda et al . 2007 ).
Human resources for health: availability of health workers
Shortage of trained staff was reported in early country studies as a major barrier to health systems, and GHI efforts to scale-up antiretroviral treatment services in particular (Grace 2004 ; Brugha et al . 2005 ; Mtonya et al . 2005 ). In 2002–04 in Zambia, it was reported that sufficient numbers of health workers were not being trained to compensate for losses due to illness, death from AIDS, and emigration (Donoghue et al . 2005a ). Both Malawi and Kenya reported public sector health worker shortages, which key informants believed would be aggravated by selectively investing in health workers to work in GHI-funded programmes for control of focal diseases such as HIV/AIDS (World Bank 2004 ; Mtonya et al . 2005 ). Migration of personnel from reproductive health and family planning through re-allocation to ‘follow the money of the Global Fund’ was reported in 2005–06 (Schott et al . 2005 ; Gbangbadthore et al . 2006 ; Wilkinson et al . 2006 ). In Ethiopia, Global Fund supported activities were inducing health workers to move away from the public to the private sector, NGOs and bilateral agencies (Banteyerga et al . 2005 ). The follow-up component of the study suggested this had worsened (Banteyerga et al . 2006 ). The nature of human resource problems varied, with shifts of health workers from public to donor supported projects/programmes as well as to other countries, causing both internal and external ‘brain drain’ (Sepulveda et al . 2007 ). However, national key informants perceived that the broader donor community and GHIs acted similarly in initiating projects that poached qualified staff from routine government programmes and employment, by offering them incentives or higher salaries (Donoghue et al . 2005a ; Drew and Purvis 2006 ).
Over time, positive responses to (partly GHI-induced) health worker shortages were reported. The follow-up study in Ethiopia found that the government had put in place a human resource strategy, which included increases in salaries and incentives to keep health workers in the public sector (Banteyerga et al . 2006 ). PEPFAR has supported a number of activities focused on retention of health workers, providing physicians working in rural areas with better working and living conditions such as housing, transportation, hardship allowances and educational stipends for their children (Sepulveda et al . 2007 ). Malawi's Global Fund Round 5 proposal addressed health worker distribution through aiming to increase community-based services by recruiting, training and retaining Health Surveillance Assistants (HSAs) to assist in scaling up antiretrovirals (Mtonya et al . 2005 ). In Benin, the Global Fund was reported to have strengthened infrastructure and provided equipment that health workers needed to better perform their tasks (Gbangbadthore et al . 2006 ).
Human resources for health: workload, motivation and incentives
The combination of the additional workload, which GHI funding has facilitated, and restrictions on public health staffing levels and remuneration have increased the strain on public sector health workers. This has been further exacerbated when GHI-funded activities accelerated staff leakage to the private sector. In Benin, it was reported that workers already working in the public sector earned no additional pay despite the extra work due to the Global Fund. However, programmes that hired health workers directly with Global Fund money were receiving higher salaries (Smith et al . 2005 ). The 2003–04 studies in Zambia and Mozambique reported that the inability to use Global Fund support to supplement the salaries of government staff running HIV programmes—most funds were going to support programme activities and purchase commodities—was de-motivating staff (Donoghue et al . 2005a ; Starling et al . 2005b ). The early focus of PEPFAR was to strengthen the skills of existing health workers to provide HIV care and treatment services and, similar to the Global Fund, funding could not be used to top-up the salaries of existing public sector staff or to hire additional staff (Sepulveda et al . 2007 ). However, in Uganda, the salaries of staff hired by NGOs were supported by PEPAR funds, which enabled them to attract the best health workers from the public sector (Oomman et al . 2007 ). MAP funding could be used for salary top-ups but only at the district government level (Oomman et al . 2007 ).
The studies reviewed here (2002–07) showed little evidence that the early GHI-funded programmes had addressed issues of workload and motivation. Where there were pre-existing shortages of health workers, GHI-supported activities were overburdening already limited capacity. The evidence suggests that the Global Fund has changed its conditions over time. Mozambique's 2002 Round 2 request for salary support for scaling up the numbers of health workers to deliver its TB control programme was rejected by the Fund (Starling et al . 2005b ). In contrast, in Malawi a Round 1 Global Fund grant was re-allocated 3 years later in 2005 to increase all health worker salaries, at the request of the government and other donors (Stillman and Bennett 2005 ).
Human resources for health: training
Early studies of the Global Fund anticipated adverse effects as ministries of health were under pressure to spend large amounts of money quickly, for example on training workshops, and health workers were relying on per diem allowances to supplement salaries (GFATM 2004 ; Brugha et al . 2005 ; Stillman and Bennett 2005 ). Most training focused largely on improving clinical skills, while planning and managerial skills, critical to successful implementation, were often neglected (McKinsey 2005 ; Stillman and Bennett 2005 ; Drew and Purvis 2006 ). In Benin, there were early missed opportunities to use Global Fund money to develop generic and transferable skills, such as management, monitoring and evaluation (Smith 2005 ).
In general, the increase in funding for training has been reported as a positive effect of GHIs. The Global Fund has allowed recipients to determine their own needs in capacity building (Oomman et al . 2007 ). In Ethiopia, the Global Fund supported the scale up training of multiple cadres, such as nurses, health officers, laboratory technicians and health extension workers (Banteyerga et al . 2005 ). In Benin, some Global Fund training provided skills transferable to disease programmes beyond the three focal diseases (Smith et al . 2005 ). PEPFAR typically supported capacity-building activities focused on training of existing personnel as an approach to addressing the shortage in human resources (Sepulveda et al . 2007 ). For example, in Uganda it funded the training of teachers to implement revised school curricula on HIV/AIDS and technical assistance for the district AIDS committees to generate HIV/AIDS strategic plans for the districts (Oomman et al . 2007 ). Oomman et al . ( 2007 ) reports that PEPFAR plans for 2008 would focus on building local capacity and a substantial amount of targets are focused on training new health workers.
The capacity-building activities of the World Bank's MAP have focused on national government, civil society organizations, district government and in particular on the community level; and have generally been seen as positive (Oomman et al . 2007 ). They have concentrated on management, administration, finance and implementation skills, although most involved short-term training. MAP was the first donor to channel a substantial amount of funding to the community level and build local capacity. In Zambia, key informants were positive about the community-response component of the MAP project (Oomman et al . 2007 ). More research is needed to determine the effect of these GHI-funded activities on human resource capacity and retention at the service delivery level in recipient countries.
Interpreting the evidence
This study has reviewed the literature on the effects of three GHIs on country health systems with respect to: 1) national policy; 2) coordination and planning; 3) stakeholder involvement; 4) disbursement, absorptive capacity and management; 5) monitoring & evaluation; and 6) human resources. This section discusses the major strengths and limitations of the quality of available evidence which is of importance when interpreting the results.
The major strength and rationale for this paper is that it has taken a systematic approach to selecting and reviewing the evidence of the health systems effects of specific GHIs in what has become a politically-charged arena. A recent review by Yu et al . ( 2008 ), on the effects on health systems of HIV/AIDS funding more generally, has cited press releases and GHI assertions, as well as commissioned evaluations, when attributing effects to GHI funding. Studies that look more broadly at the effects of increased funding to HIV/AIDS control are also less likely to shed light on the specific health systems effects and the particular strengths and weaknesses of different GHIs. The chapter by Brugha ( 2008 ) was not a systematic review and aimed to draw out the policy processes involved and policy lessons learned since the emergence of GHIs, rather than to review their effects on health systems. The framework that has been applied here is derived from early country experiences in managing GHIs, experiences that are not adequately captured in WHO's health systems building blocks frameworks (WHO 2007 ). The review provides an historical backdrop to forthcoming district-level studies; but also points to some chronic, refractory problems at the national level, which are inherent in the incentive systems underlying disease-specific initiatives.
Despite our systematic approach, the available evidence in this review has several limitations. First, most studies have focused on the national level, where GHI effects are initially felt. There was little empirical evidence (and much conjecture) regarding their effects at the district, facility and community levels. It is here that the strengths, weaknesses and added value (or not) of these still new, disease-specific initiatives will play out and will need to be assessed.
Secondly, with a few exceptions, most were descriptive studies with a cross-sectional design, which limits their capacity to demonstrate changes over time. GHIs have evolved and have sometimes been quite adept in learning and applying lessons, which has been more evident with the Global Fund than with PEPFAR. Rapid lesson-learning has meant that some study findings quickly become outdated or new problems supersede old ones.
Thirdly, not all GHIs and regions of the world have been studied equally. The Global Fund, because of its visibility and transparency, has been evaluated most often, whereas PEPFAR has remained the most opaque of these GHIs. Moreover, the limited empirical evidence on MAP, Global Fund and PEPFAR country-level effects relied heavily on evaluations conducted or commissioned by—or on behalf of—these initiatives, which may affect their validity. Most evidence is also based on studies conducted in sub-Saharan Africa, which is naturally the priority region for three HIV/AIDS-focused GHIs.
Lastly, mainly because this review relied heavily on unpublished reports (‘grey literature’), appraisal of the quality of data collection and interpretation was hampered by limited information on methods, quality control and analysis. Furthermore, the lack of consensus on appropriate criteria for assessing qualitative research (Dixon-Woods et al . 2004 ; Goldsmith et al . 2007 ) precluded us from making formal judgements on the quality of the studies.
This review has contributed to the surprisingly thin body of evidence regarding the health systems effects of three major GHIs. The systematic approach adopted has produced a series of findings that are of relevance to the current international debate on this issue. Based on the findings presented above, conclusions and recommendations are proposed that are relevant to national and international policy makers, donors, researchers and indeed civil society organizations.
Overall, the findings of this review of studies published between 2002 and 2007 suggest that the three GHIs initially often had negative effects, and later—as they learned lessons—more often positive effects on health systems. They also had different effects. From its outset, MAP was viewed positively for its capacity-building activities at national and district public-sector levels, and particularly at the community level. The Global Fund's particular strength has been in boosting the engagement of NGOs and faith-based bodies, bringing them into planning structures with government and enabling them to access significant funds. PEPFAR is well regarded for its fast and predictable disbursement of funding to civil society implementers.
At the level of national policy development , GHIs have generally made most progress in aligning with national joint strategic planning processes, while harmonization of activities with other partners has remained a challenge. Effects on other national health priorities, such as family planning and maternal care, were not reported and will require district and facility studies to assess effects at the service delivery level. While the Global Fund supported, with variable success, programmes that reflected local priorities and country ownership, PEPFAR's rigid budget allocations were more difficult to fit to a country's own priorities for health.
MAP's support to a multisectoral response has been most hindered by the weak capacity and lack of intersectorality of recipient country ministries, which supports the hypothesis that GHIs reveal rather than cause country systems weaknesses. Indeed, GHIs did not initially consider health systems strengthening to be part of their mandate but are now more willing to address systems weaknesses (Brugha et al . 2005 ; McKinsey 2005 ). This is all the more important now because, due to the rapid GHI-supported scaling up of HIV care and treatment in low income countries, HIV and AIDS are being transformed from an epidemic emergency to an endemic manageable chronic disease . As such, HIV control will require health systems that support continuity of care and the retention and follow up of patients with multiple and multi-systems diseases (El-Sadr and Abrams 2007 ).
Despite some positive developments, such as the integration of Global Fund support into some countries’ SWAps, donor harmonization activities have continued to fall short. While the vertical funding, planning and performance monitoring approaches that have characterized the GHIs could be seen as more efficient responses to tackling disease emergencies, these approaches created substantial barriers to harmonizing donor activities. They also reflected GHIs’ inherent need to demonstrate value for money through donor-specific measurements of performance. More recently, the GHIs have retreated from making claims of initiative-specific attributable successes (Brugha 2007 ; Gorgens-Albino et al . 2007 ), acknowledging the interplay of the many inputs and factors affecting programme implementation and service delivery. This was probably in response to the inherent difficulties of attribution in the complex multi-funded terrain of African health systems (Bennett et al . 2006 ). It also reflected a change in the global development assistance climate in the light of the Paris Declaration on Aid Effectiveness (OECD 2005 ).
However, it is at the national policy implementation level where the main early effects of GHIs—often negative at first and subsequently positive—have been encountered and documented. GHIs have led to multiple and parallel coordinating bodies , such as Global Fund CCMs, that have conflicted and sometimes contested with pre-existing bodies such as National AIDS Councils. Often, neither was providing the necessary leadership and oversight. Others, such as PEPFAR, established and continued to use parallel planning processes, inevitably pulling governments and other implementers away from other important activities because of the volume of funds at stake. However, positive effects have followed negative ones in that CCMs have enabled substantial improvements in stakeholder participation in the health sector. Through all three GHIs, NGOs and faith-based organizations have become direct recipients of significant levels of funding and thereby additional programme implementers. While there are great advantages to involving a greater diversity of actors, these new sources of funds have provoked real tensions in resource-starved settings between governments, as the traditional recipients of donor aid, and new civil society implementing organizations. Emerging evidence suggests that GHIs, which have been either geographically or ideologically detached from these concerns, have not done enough to help manage these tensions.
Where GHIs have been most retrograde has been in maintaining their own fiscal cycles, systems for auditing expenditure and GHI-specific reporting requirements. There have been gradual efforts to reduce transaction costs for countries. For example, the Global Fund has shown a willingness (in principle, at least) to adapt and align with country systems and directly fund countries’ national disease control plans, for example through ‘rolling continuation channels’ (GFATM 2007 ). However, it has continued to utilize a non-aligned Local Fund Agent model for financial management and audit (GFATM 2008b ). More recently, GHIs have started to work with countries in strengthening monitoring and evaluation systems and increasing local capacity, although this has mainly been for HIV/AIDS programmes and strengthening of the wider national health system has been neglected.
Finally, the effective implementation of GHI-supported programmes depends on human resources , which are recognized as the main bottleneck to scaling-up service delivery, especially in sub-Saharan Africa. There were credible, if anecdotal, early reports that different funding sources were competing for a limited pool of health workers by offering them incentives or higher salaries, which accelerated public sector staff leakage to non-government sectors. The combination of additional workload and remuneration constraints led to de-motivated and overburdened health workers in the public sector. One of the reasons was that GHI requirements in the early years, except to some extent MAP, precluded the funding of salaries for additional public sector health workers. Countries have also invested heavily in writing funding applications, whereas capacity for implementation of GHI-funded programmes has often been lacking. The early studies reviewed here suggest that the Global Fund and PEPFAR limited their human capacity-building activities to training existing health care workers, while MAP undertook a wider approach to capacity building at national and community levels. However, again, emerging evidence suggests that GHIs have been increasingly recognizing the importance of focusing attention on (and funding for) training and improving work and living conditions of health workers in rural areas as retention strategies.
The principal recommendation to GHIs, recipient donor countries, civil society organizations and technical agencies alike is to engage more fully with the Paris Principles for Aid Effectiveness as an important step in maximizing positive and minimizing negative effects of their programmes: Secondly, country and global policy makers and donors should demand and fund the acquisition of better evidence on what is a complex and rapidly evolving arena. What is now needed are coordinated evaluations using multiple methods in order to assess and understand the combined effects of GHIs and how they work alongside longer-standing disease-control financing mechanisms. Given the rapid learning of GHIs, which is often but not always applied, continuous monitoring and independent evaluations are needed to track changes and identify refractory problems. Early evaluations have been generally descriptive, necessary because of the rapid evolution in the GHI arena. Now, more analytical health policy and health systems evaluations are needed.
GHIs, which have signed up to these principles, could do much more to promote country ownership through aligning their objectives with comprehensive national health (rather than only HIV/AIDS) priorities.
Coordinated GHI investment to strengthen the capacity of national systems for financial management, M&E and reporting could thereby give GHIs the confidence to harmonize, align and use these systems.
There is an obvious need for stronger coordination of donor investments to support countries’ national strategic health plans, which can include flexibility to allow GHIs and other donors to support specific components of such plans.
GHIs should give recipient countries sufficient flexibility to address systems’ weaknesses and strengthen implementation capacity, especially in human resources at all levels.
Public sector health worker shortages, recognized as the key determinant for wide-ranging efforts to scale-up health-related priority interventions, should be addressed by GHIs through providing long-term funding for additional human resources for the health sector.
GHIs should continue to encourage the participation of non-government as well as government stakeholders, while reducing tensions created by funding new implementers in service delivery by requiring them, as far as possible, to utilize and contribute data to national information systems.
We believe this review of evidence on the early national effects of GHIs is timely, in advance of dissemination of findings in 2009 from the Global Fund Five Year Evaluation ( http://www.theglobalfund.org/en/about/terg/five_year_evaluation/ ), the Global HIV/AIDS Initiatives Network (GHIN – http://www.ghinet.org ) 3 and the recent WHO-launched initiative ‘Maximising Positive Synergies between health systems and GHIs’ (WHO 2008 ). Syntheses and interpretation of findings from these different evaluations—on a country-by-country basis—could provide invaluable lessons on how a much more complex mix of funding for disease control and health systems strengthening can work together in a complementary way to support country-led efforts to roll back the HIV and AIDS epidemic. They could also provide lessons for the establishment of effective long-term, comprehensive monitoring and evaluation systems.
Regien Biesma was funded under a 4-year research project grant, ‘GHIs in Africa’ (INCO-CT-2006-032371), funded by the EU 6th framework INCO-DEV programme. The INCO partners are based in three southern African countries (Angola, Mozambique and South Africa) and three European countries (Belgium, Ireland and Portugal). The authors would like to thank all partners who provided helpful comments on an earlier review of global health initiatives. Neil Spicer is funded under a grant from the Open Society Institute (OSI). Aisling Walsh is funded under the Global HIV/AIDS Initiatives Network (GHIN) grant, funded by Irish Aid and DANIDA. Ruairí Brugha and Gill Walt are co-coordinators of the GHIN network. Andrew Harmer was funded under a UK Department for International Development (DFID) grant to design a database on global health initiatives.
The authors acknowledge with appreciation financial support from the Open Society Institute to undertake research on global HIV/AIDS initiatives and their effects on health systems.
MAP was small relative to the total annual amounts provided by the Global Fund and PEPFAR, which had become the major external funder of HIV/AIDS control in sub-Saharan Africa by 2007 (Oomman et al . 2007 ). However, MAP was the first of these new GHIs for funding HIV/AIDS control, whose impact on countries’ health systems was experienced and reported across 2002–07.
Our initial review used the following Boolean string: (global health initiatives OR global health partnership OR public-private partnership OR Global Fund OR PEPFAR OR World Bank MAP) AND (HIV/AIDS) AND (effects OR national policy OR financial flow OR public-private partnerships OR planning and coordination OR implementation and monitoring and evaluation OR human resources).
The Global HIV/AIDS Initiatives Network (GHIN) is examining the effects and the inter-relationships of the three global health initiatives. GHIN has its origins in the Global Fund Tracking Study (2003–04), and in the SWEF studies (2005–06), which together provided several of the studies and papers reviewed.
Google Scholar
Google Preview
- acquired immunodeficiency syndrome
- delivery of health care
- world health
- human resource management
- president's emergency plan for aids relief
- nongovernmental organizations
Email alerts
Citing articles via.
- Recommend to Your Librarian
Affiliations
- Online ISSN 1460-2237
- Copyright © 2024 The London School of Hygiene and Tropical Medicine and Oxford University Press
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Institutional account management
- Rights and permissions
- Get help with access
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
- Chronicle Conversations
- Article archives
- Issue archives

Advancing the Global Health Agenda
About the author, ilona kickbusch.
December 2011, No. 4 Vol. XLVIII, 7 Billion People, 1 United Nations, Hand in Hands
I n just over two decades, global health has gained a political visibility and status that some authors have called a political revolution. As health related issues have become a centre piece of the global agenda, significant resources in development aid have been made available to address major health problems. Global health has gained this political prominence because three agendas have reinforced one another in a variety of ways:
a security agenda driven by the fear of global pandemics or the intentional spread of disease, in an era where viruses have the potential to spread from one part of the world to another in a matter of hours;
an economic agenda, which is concerned not only with the economic impact of poor health on development or of pandemic outbreaks in the global marketplace, but increasingly considers the economic relevance of the health sector, in particular of certain industries, such as tobacco, food, and pharmaceuticals, and the growing global market of goods and services in relation to health;
a social justice agenda advocating health as a social value and human right, which includes action on the social determinants of health, access to medicines, support for the Millennium Development Goals (MDGs) relating to health, and the active engagement of philanthropies and civil society in a broad range of global health initiatives.
The global health agenda brings together two critical action spheres of our time: managing interdependence and globalization, and addressing the growing inequalities within and between nations through development strategies. It also lies at the intersection of many policy arenas and is subject to a special dynamic. On the one hand, poor health is frequently a consequence of other global crises such as finance, food insecurity, or climate change, while on the other hand, the whole of society bears the impact if health challenges are not well managed. Indeed, the economic consequences of governance failures in health, be they national or global, are significant; epidemics such as HIV/AIDS or disease outbreaks such as severe acute respiratory syndrome (SARS) or H1N1 influenza have proven this. Poor health will hinder development or destroy any development gains which were achieved through great effort. At present, this is best illustrated through The Global Economic Burden of Non-communicable Diseases (NCDs), a study prepared in 2011 by the World Economic Forum and the Harvard School of Public Health, which calculated that over the next 20 years, NCDs will cost more than $30 trillion, representing 48 per cent of the global GDP in 2010, thus pushing millions of people below the poverty line. This will result in a dramatic negative impact on the productivity and quality of life in many countries and regions of the world.
THE UNITED NATIONS AND HEALTH
A series of commitments, a wide range of international health policy instruments, new organizations and initiatives, as well as a broadening of the scope of health debates have marked efforts to improve health throughout the world over the past two decades. Many of these have emerged as a response to the increasingly complex global challenges defined by rising inequalities, epidemiological and demographic transitions, double disease burdens for many countries, unexpected natural disasters, such as the tsunami that occurred in Japan and the earthquake in Haiti, or the persistence of other threats, like the far-reaching consequences of the financial crisis.
In this context, the United Nations and its specialized agency for health, the World Health Organization (WHO), have played a crucial role by exercising its constitutional functions, in particular its convening power and its normative and standard-setting work. It has been fundamental to refer major global health issues to the United Nations General Assembly in order to underline that:
health must be considered an investment in both human and economic development;
health is a central building block in fighting poverty and in ensuring sustainable development;
health security and protection is the cornerstone of human security.
With the establishment of the Millennium Development Goals, following the Millennium Summit in 2000, came the first breakthrough -- the recognition of women's and children's health, as well as infectious diseases. In 2001, the UN General Assembly Special Session on HIV/AIDS stated in its Declaration of Commitment that "the global HIV/AIDS epidemic is a global emergency and one of the most formidable challenges to human life and dignity, as well as to the effective enjoyment of human rights". More recently, in 2011, the United Nations held the High-Level Meeting on Non- Communicable Diseases, which resulted in a political declaration and launched the Global Strategy for Women's and Children's Health.
HEALTH AT WHO
Despite significant funding problems, in recent decades WHO has worked towards the attainment of the highest possible standards of health in many ways, ranging from disease- specific programmes to overall efforts to strengthen health care systems based on primary health care. Many observers fail to realize that some of the most critical breakthroughs for global health have occurred as a result of the treaty-making power of the Organization, and through the strengthening of its normative role. Key examples include:
The WHO Framework Convention on Tobacco Control, the first international treaty negotiated under the auspices of WHO, was adopted in 2003 and entered into force in 2005. It has become one of the most rapidly and widely embraced treaties in United Nations history.
Since June 2007, states have been implementing the International Health Regulations adopted by the World Health Assembly in 2005. This legally-binding agreement provides a new framework for the coordination of the management of public health emergencies of international concern.
In 2011, WHO member States adopted the Pandemic Influenza Preparedness Framework, which brings together member States, industry, other key stakeholders, and WHO to implement a global approach to pandemic influenza preparedness and response, improve in the sharing of knowledge concerning influenza viruses with pandemic potential, and achieve more equitable access to life-saving vaccines and medicines.
In May 2010, WHO member States adopted the Global Code of Practice on the International Recruitment of Health Personnel to address the challenge of health worker migration, especially from low-income countries with already fragile health systems. It marked the first time in 30 years that WHO member States used the constitutional authority of the Organization to develop a code, following the adoption of the International Code of Marketing of Breast-milk Substitutes in 1981.
MONEY IS NOT ENOUGH
Global health is far more multifaceted than is often perceived, and requires more than development aid to achieve. In a global world, we need an integrated approach which includes action on social determinants, social protection, the support for major health care programmes at the local and country level, and the global agreements and commitments necessary to address the responsibilities and approaches of the many actors involved. One of the key challenges that global health faces at this point in time is the need to integrate the many laudable health initiatives which often run parallel to the health systems of the countries concerned. We still have a long way to go from the country ownership that was agreed upon in the 2005 Paris Declaration on Aid Effectiveness and the 2008 Accra Agenda for Action.
Too frequently, the global health debate is dominated by concentrating on the funding gap. For example, one calculation indicates that an extra $250 billion would be needed to reach the health MDGs over the next 5 to 10 years, of which $70 billion would come from donors. A much needed shift in perspective requires:
donors and countries to put more effort into developing domestic financing structures for health that are fair and sustainable;
national development strategies that counteract fragmented, short-term, and unpredictable aid for health;
social protection to be addressed with new urgency, as out-of-pocket payment for health care pushes people under the poverty line;
better use of the resources provided;
different sectors of government to work together to promote health nationally and internationally.
However, these remain difficult without the commitment and political will of the ruling elites. A case in point is the glob- al NCD challenge, which requires whole-of-government and whole-of-society approaches. Mounting evidence highlights how millions of deaths can be averted and economic losses reduced by billions; but progress requires action in many policy arenas, such as social policy, urban development, taxation, and education. Population-based measures for reducing tobacco and harmful alcohol use, as well as unhealthy diets and physical inactivity, are estimated to cost $2 billion per year for all low- and middle-income countries which, in fact, translates to less than $0.40 per person.
MORE VOICES FOR HEALTH -- MORE SKILLS TO NEGOTIATE
More actors want to have their voices heard on global health matters at the national and international level. The number of organizations active in health at the global level has increased considerably, and many of them are exploring innovative financing and governance models. Such new actors include the Global Fund to Fight AIDS, Tuberculosis and Malaria; the Joint United Nations Programme on HIV/ AIDS; and the GAVI Alliance. The Bill and Melinda Gates Foundation, and others like it, have changed the face of global health through significant financial contributions and a new approach to venture philanthropy, looking for innovation that supports the poorest. The private sector, first challenged by the UN Global Compact, has become active in new ways and is now involved in a myriad of health initiatives, including the United Nations debate on NCDs. A growing number of countries and regional organizations, such as the European Union, are developing an active stance in matters pertaining to global health. These new voices are heard during the debates on the reform of WHO, which is currently under way. They raise questions such as how can more stakeholders be involved? How can the voices of civil society be heard? How should the United Nations Organization deal with the private sector?
At the national level, the diversity of global health issues has gradually brought ministries of health, foreign affairs, security, economics, and development into a new dialogue. Global health today requires a skill mix of technical health knowledge, negotiating expertise, as well as awareness about geopolitical constellations, overlapping alliances, and trade and economic implications, to mention just a few. Some countries have begun to train negotiators in global health diplomacy and have introduced formal global health strategies to guide their actions in the global arena. This now includes not only WHO, but other international venues, such as the World Trade Organization, the Human Rights Council, and the Group of Twenty (G20) Finance Ministers and Central Bank Governors. The proposal of a financial transaction tax, for example, has long been on the agenda of health advocates in order to secure sustainable financing for health programmes.
Since 2008, the relationship between health and foreign policy is changing, as highlighted in the UN General Assembly resolution on Global Health and Foreign Policy. A group of foreign ministers have proposed that foreign policy apply a health lens, and that the protection of health interests should not necessarily be mutually exclusive with other core interests of countries. There are increasing opportunities where foreign policy interests can support health, and the initiatives by many emerging economies in South-South programmes are a good example of this. Finding mutually beneficial synergies between countries is critical in order to move the global health agenda forward.
THE INDISPENSABLE ROLE OF THE UNITED NATIONS
Global health deals with a wide range of concerns and tensions, not only between countries but between sectors, and between many different actors and interests. The growing complexity calls for better global health governance, including better coherence among multiple initiatives, clear distribution of responsibilities, and more transparency and accountability. The resulting debate revolves around key questions regarding where the leadership and authority on global health should lie, who should be involved, and what legitimate roles different actors could have, so that the potential of each of the diverse players can be utilized for the benefit of all. Who better to take on this challenge than the United Nations?
The UN Chronicle is not an official record. It is privileged to host senior United Nations officials as well as distinguished contributors from outside the United Nations system whose views are not necessarily those of the United Nations. Similarly, the boundaries and names shown, and the designations used, in maps or articles do not necessarily imply endorsement or acceptance by the United Nations.

The LDC Future Forum: Accelerating the Attainment of the Sustainable Development Goals in the Least Developed Countries
The desired outcome of the LDC Future Forums is the dissemination of practical and evidence-based case studies, solutions and policy recommendations for achieving sustainable development.

From Local Moments to Global Movement: Reparation Mechanisms and a Development Framework
For two centuries, emancipated Black people have been calling for reparations for the crimes committed against them.

World Down Syndrome Day: A Chance to End the Stereotypes
The international community, led by the United Nations, can continue to improve the lives of people with Down syndrome by addressing stereotypes and misconceptions.
Documents and publications
- Yearbook of the United Nations
- Basic Facts About the United Nations
- Journal of the United Nations
- Meetings Coverage and Press Releases
- United Nations Official Document System (ODS)
- Africa Renewal
Libraries and Archives
- Dag Hammarskjöld Library
- UN Audiovisual Library
- UN Archives and Records Management
- Audiovisual Library of International Law
- UN iLibrary
News and media
- UN News Centre
- UN Chronicle on Twitter
- UN Chronicle on Facebook
The UN at Work
- 17 Goals to Transform Our World
- Official observances
- United Nations Academic Impact (UNAI)
- Protecting Human Rights
- Maintaining International Peace and Security
- The Office of the Secretary-General’s Envoy on Youth
- United Nations Careers
")
- Health topics
- Data and statistics
- Media centre
- Information resources
Section menu
You are here, global health initiatives.

The Global Fund and Gavi, the Vaccine Alliance are the main institutions that provide substantial funding to eligible countries in the Region. Seven countries – Afghanistan, Djibouti, Pakistan, Somalia, Sudan, Syrian Arab Republic and Yemen – are eligible for Gavi support on immunization and health system strengthening, and 12 are eligible for Global Fund grants, including the seven supported by Gavi.
Protracted social and political unrest in most grant-recipient countries continues to be a major challenge. Insecurity in many places hampers access to social services with the health sector being the worst affected, and the loss of human capital has severely weakened health services and systems in affected countries. Furthermore, global health initiatives have created parallel systems that undermine the holistic approach for health system development, and the principles of external aid, such as ownership and harmonization, are not adequately applied.

Gavi, The Vaccine Alliance
Gavi support to:
Afghanistan
The Global Fund

The Global Fund to Fight AIDS, Tuberculosis and Malaria

Policy on WHO Engagement with Global Health Partnerships and Hosting Arrangements
Partnerships and Collaborative Arrangements with WHO involvement
WHO: Key player in global immunization and founding member of the Vaccine Alliance
Help and services
- Cyber security
WHO Offices
- WHO headquarters
- WHO African Region
- WHO Region of the Americas
- WHO South-East Asia Region
- WHO European Region
- WHO Western Pacific Region
Connect with us
Why is global health important?
- Post author: Global Health Core
- Post published: April 25, 2019
- Post category: Uncategorized
The Importance of Global Health in The Modern World
The global health field addresses the quality of healthcare around the world, from developing nations to world powers. For residents of countries with strong healthcare systems, it can be tempting to wonder, why is global health important? When everything in your community is taken care of, it is easy to dismiss concerns in other parts of the world as other people’s problems. This is a short-sighted approach to healthcare, however. The world grows more and more connected every day, and that’s why global health should also be considered an important part of local health. Here are a few of the best reasons why global health matters to everyone, no matter where they are from.
Healthier Communities Around the Globe
The first benefit of improving global health is a humanitarian one. By investing in healthcare around the world, including in areas not capable of building the required healthcare systems on their own, the world becomes a healthier and happier place. Improving healthcare in developing nations offers the most opportunity to have a massive impact in terms of lives improved and lives saved. Developing nations are also not the only ones helped by global health groups. While much of their work is done in nations with the most need, global really means global, and even well-developed nations can benefit directly from global health work.
Reduced Risk of Spreading Diseases
There are more reasons to help nations in need than just kindness. Global health initiatives can help to reduce the risk of diseases spreading around the world. International travel means no country is truly isolated from another, and outbreaks in any nation have the potential to spread to areas on the entire other side of the planet when individuals are infected abroad then return home.
Increased Understanding of International Patients
Spreading global health awareness also makes doctors more capable of treating the patients they see on a daily basis. Customs and traditions vary around the world, so a doctor who is well taught in global health issues is in a better position to treat their foreign patients with caring and understanding, providing the care they need while also respecting the patient’s cultural norms.
Healthcare Talent Can Come From Anywhere
There is no way to know where the next great medical mind will be born, and if someone with a talent for healthcare is born somewhere that the healthcare and educational systems are not in place to nurture that talent, the world as a whole loses out. By increasing medical access around the world, global health workers make it easier for someone interested in healthcare to flourish, no matter where they are born, which in turn increases the chance that important breakthroughs for the entire world are achieved.
You Might Also Like
What are the 10 most common diseases, what are the biggest health problems in the world, what are the global health issues.
Reimagining the Future of Global Health Initiatives: Final Report Release

30/08/23 News
We are thrilled to announce the release of the final report from our research project, “ Reimagining the Future of Global Health Initiatives .” This report delves deep into the intricate world of Global Health Initiatives (GHIs), offering invaluable insights into their trends, challenges, and positive contributions that are shaping the global health landscape.
Uncover the Global Health Landscape
In an ever-evolving world, the realm of global health is marked by both opportunities and complexities. Our report takes a closer look at the dynamic trends that are shaping the future of global health initiatives. From innovative financing strategies that are revolutionizing healthcare funding to unforeseen outcomes that have sparked new discussions, this report is a treasure trove of knowledge for those invested in the world of health.
We invite you to dive into the rich insights presented in this report. Whether you’re a healthcare professional, researcher, policymaker, or simply someone passionate about global health, there’s something for everyone in this comprehensive study. You can read it online or dowload the Final Report , the Research Brief, and the Summary Notes .
Privacy Overview
- Undergraduate
- High School
- Architecture
- American History
- Asian History
- Antique Literature
- American Literature
- Asian Literature
- Classic English Literature
- World Literature
- Creative Writing
- Linguistics
- Criminal Justice
- Legal Issues
- Anthropology
- Archaeology
- Political Science
- World Affairs
- African-American Studies
- East European Studies
- Latin-American Studies
- Native-American Studies
- West European Studies
- Family and Consumer Science
- Social Issues
- Women and Gender Studies
- Social Work
- Natural Sciences
- Pharmacology
- Earth science
- Agriculture
- Agricultural Studies
- Computer Science
- IT Management
- Mathematics
- Investments
- Engineering and Technology
- Engineering
- Aeronautics
- Medicine and Health
- Alternative Medicine
- Communications and Media
- Advertising
- Communication Strategies
- Public Relations
- Educational Theories
- Teacher's Career
- Chicago/Turabian
- Company Analysis
- Education Theories
- Shakespeare
- Canadian Studies
- Food Safety
- Relation of Global Warming and Extreme Weather Condition
- Movie Review
- Admission Essay
- Annotated Bibliography
- Application Essay
- Article Critique
- Article Review
- Article Writing
- Book Review
- Business Plan
- Business Proposal
- Capstone Project
- Cover Letter
- Creative Essay
- Dissertation
- Dissertation - Abstract
- Dissertation - Conclusion
- Dissertation - Discussion
- Dissertation - Hypothesis
- Dissertation - Introduction
- Dissertation - Literature
- Dissertation - Methodology
- Dissertation - Results
- GCSE Coursework
- Grant Proposal
- Marketing Plan
- Multiple Choice Quiz
- Personal Statement
- Power Point Presentation
- Power Point Presentation With Speaker Notes
- Questionnaire
- Reaction Paper
Research Paper
- Research Proposal
- SWOT analysis
- Thesis Paper
- Online Quiz
- Literature Review
- Movie Analysis
- Statistics problem
- Math Problem
- All papers examples
- How It Works
- Money Back Policy
- Terms of Use
- Privacy Policy
- We Are Hiring
Global Health Care, Essay Example
Pages: 3
Words: 917
Hire a Writer for Custom Essay
Use 10% Off Discount: "custom10" in 1 Click 👇
You are free to use it as an inspiration or a source for your own work.
Introduction
Global health care is a challenging phenomenon that supports the development of new perspectives and approaches to solving global health concerns, including nutrition, infectious disease, cancer, and chronic illness. It is important to address global health as a driving force in international healthcare expenditures because it represents an opportunity for clinicians throughout the world to collaborate and to address global health concerns to achieve favorable outcomes. Global healthcare in the modern era includes the utilization of technology to support different population groups and to address different challenges as related to global health problems that impact millions of people in different ways. These challenges demonstrate the importance of large-scale efforts to eradicate disease, to prevent illness, and to manage disease effectively through comprehensive strategies that encourage communication and collaboration across boundaries.
Global health care incorporates a number of critical factors into play so that people throughout the world are given a chance to live and to lead a higher quality of life. The World Health Organization (WHO) is of particular relevance because this organization supports global health initiatives and large-scale impact projects throughout the world (Sundewall et.al, 2009). The WHO recognizes the importance of developing strategies to address global health concerns by pooling resources in order to ensure that many population groups are positively impacted by these initiatives (Sundewall et.al, 2009). The WHO also collaborates with government bodies throughout the world to address specific concerns that are relevant to different population groups, such as infectious diseases, many of which ravage populations in a significant manner (Fineberg and Hunter, 2013). In this context, it is observed that global health has a significant impact on populations and their ability to thrive, given the high mortality rates of some diseases in less developed nations (Fineberg and Hunter, 2013). Therefore, it is expected that there will be additional frameworks in place to accommodate the needs of populations and the resources that are required to achieve favorable outcomes (Fineberg and Hunter, 2013).
In addition to the WHO, there are many other international organizations that support global health and disease in different ways. For example, The United Nations Children’s Fund (UNICEF) supports large-scale global health efforts to support the world’s children (imva.org, 2013). UNICEF works in conjunction with many governments and other sources of funding in order to accomplish its objectives related to child health and wellbeing (imva.org, 2013). UNICEF spends significant funds on many focus areas, including the preservation of child health, nutrition, emergency support, and sanitation in conjunction with local water supplies (imva.org, 2013). In addition, the United States Agency for International Development (USAID) provides support in many areas, including a primary focus on healthcare in developing nations (imva.org, 2013).
Leininger’s Culture Care Theory is essential in satisfying the objectives of global health because it supports an understanding of the issues related to cultural diversity and how they impact healthcare practices throughout the world (Current Nursing, 2012). This theory embodies many of the differences that exist in modern healthcare practices and supports a greater understanding of the issues that are most relevant on a global scale (Current Nursing, 2012). This theory is applicable because it represents a call to action to consider cultural differences when providing care and treatment to different population groups, but not at the expense of the quality of care that is provided (Current Nursing, 2012). In many countries, the provision of care is largely dependent on cultural diversity and customs, which is essential to a thriving healthcare system; however, diversity must also incorporate the concept of providing maximum care for an individual in need of treatment (Current Nursing, 2012).
Professional nursing is highly relevant to global health because nurses address some of the most critical challenges in providing care and expanding access to treatment for millions of people throughout the world. However, it is also important for nurses working with global health initiatives to recognize the importance of these directives and to consider ways to improve quality of care without compromising principles or other factors in the process. These efforts will ensure that nurses maximize their knowledge and understanding of global health and its scope in order to achieve positive outcomes for people in desperate need of healthcare services throughout the world. Nurses must collaborate with small and large-scale organizations regarding global health issues so that population needs are targeted and are specific. These efforts will ensure that patients are treated in areas where healthcare access is severely limited.
Global health represents a significant set of challenges for clinicians throughout the world. It is important to recognize these concerns and to take the steps that are necessary to provide patients with the best possible outcomes to achieve optimal health. The scope of global health concerns is significant; therefore, it is important to address these concerns and to take the steps that are necessary to collaborate and promote initiatives to fight global health problems. When these objectives are achieved using the knowledge and expertise of nurses, it is likely that there will be many opportunities to treat patients and to educate them regarding positive health. With the assistance of large global organizations, nurses play an important role in shaping outcomes for women throughout the world.
Current Nursing (2012). Transcultural nursing. Retrieved from http://currentnursing.com/nursing_theory/transcultural_nursing.html
Fineberg, H.V., and Hunter, D. J. (2013). A global view of health – an unfolding series. T he New England Journal of Medicine, 368(1), 78-79.
Imva.org (2013). Bilateral agencies. Retrieved from http://www.imva.org/Pages/orgfrm.htm
Sundewall, J., Chansa, C., Tomson, G., Forsberg, B.C., and Mudenda, D. (2009). Global health initiatives and country health systems. The Lancet, 374, 1237.
Stuck with your Essay?
Get in touch with one of our experts for instant help!
Helping People: Compassion, Essay Example
Why Is There a Need to Breastfeed, Research Paper Example
Time is precious
don’t waste it!
Plagiarism-free guarantee
Privacy guarantee
Secure checkout
Money back guarantee

Related Essay Samples & Examples
Voting as a civic responsibility, essay example.
Pages: 1
Words: 287
Utilitarianism and Its Applications, Essay Example
Words: 356
The Age-Related Changes of the Older Person, Essay Example
Pages: 2
Words: 448
The Problems ESOL Teachers Face, Essay Example
Pages: 8
Words: 2293
Should English Be the Primary Language? Essay Example
Pages: 4
Words: 999
The Term “Social Construction of Reality”, Essay Example
Words: 371
- Open access
- Published: 07 April 2020
What is global health? Key concepts and clarification of misperceptions
Report of the 2019 GHRP editorial meeting
- Xinguang Chen 1 , 2 ,
- Hao Li 1 , 3 ,
- Don Eliseo Lucero-Prisno III 4 ,
- Abu S. Abdullah 5 , 6 ,
- Jiayan Huang 7 ,
- Charlotte Laurence 8 ,
- Xiaohui Liang 1 , 3 ,
- Zhenyu Ma 9 ,
- Zongfu Mao 1 , 3 ,
- Ran Ren 10 ,
- Shaolong Wu 11 ,
- Nan Wang 1 , 3 ,
- Peigang Wang 1 , 3 ,
- Tingting Wang 1 , 3 ,
- Hong Yan 3 &
- Yuliang Zou 3
Global Health Research and Policy volume 5 , Article number: 14 ( 2020 ) Cite this article
53k Accesses
27 Citations
8 Altmetric
Metrics details
The call for “W orking Together to Build a Community of Shared Future for Mankind” requires us to improve people’s health across the globe, while global health development entails a satisfactory answer to a fundamental question: “What is global health?” To promote research, teaching, policymaking, and practice in global health, we summarize the main points on the definition of global health from the Editorial Board Meeting of Global Health Research and Policy, convened in July 2019 in Wuhan, China. The meeting functioned as a platform for free brainstorming, in-depth discussion, and post-meeting synthesizing. Through the meeting, we have reached a consensus that global health can be considered as a general guiding principle, an organizing framework for thinking and action, a new branch of sciences and specialized discipline in the large family of public health and medicine. The word “global” in global health can be subjective or objective, depending on the context and setting. In addition to dual-, multi-country and global, a project or a study conducted at a local area can be global if it (1) is framed with a global perspective, (2) intends to address an issue with global impact, and/or (3) seeks global solutions to an issue, such as frameworks, strategies, policies, laws, and regulations. In this regard, global health is eventually an extension of “international health” by borrowing related knowledge, theories, technologies and methodologies from public health and medicine. Although global health is a concept that will continue to evolve, our conceptualization through group effort provides, to date, a comprehensive understanding. This report helps to inform individuals in the global health community to advance global health science and practice, and recommend to take advantage of the Belt and Road Initiative proposed by China.
“Promoting Health For All” can be considered as the mission of global health for collective efforts to build “a Community of Shared Future for Mankind” first proposed by President Xi Jinping of China in 2013. The concept of global health continues to evolve along with the rapid development in global health research, education, policymaking, and practice. It has been promoted on various platforms for exchange, including conferences, workshops and academic journals. Within the Editorial Board of Global Health Research and Policy (GHRP), many members expressed their own points of view and often disagreed with each other with regard to the concept of global health. Substantial discrepancies in the definition of global health will not only affect the daily work of the Editorial Board of GHRP, but also impede the development of global health sciences.
To promote a better understanding of the term “ global health” , we convened a special session in the 2019 GHRP Editorial Board Meeting on the 7th of July at Wuhan University, China. The session started with a review of previous work on the concept of global health by researchers from different institutions across the globe, followed by free brainstorms, questions-answers and open discussion. Individual participants raised many questions and generously shared their thoughts and understanding of the term global health. The session was ended with a summary co-led by Dr. Xinguang Chen and Dr. Hao Li. Post-meeting efforts were thus organized to further synthesize the opinions and comments gathered during the meeting and post-meeting development through emails, telephone calls and in-person communications. With all these efforts together, concensus have been met on several key concepts and a number of confusions have been clarified regarding global health. In this editorial, we report the main results and conclusions.
A brief history
Our current understanding of the concept of global health is based on information in the literature in the past seven to eight decades. Global health as a scientific term first appeared in the literature in the 1940s [ 1 ]. It was subsequently used by the World Health Organization (WHO) as guidance and theoretical foundation [ 2 , 3 , 4 ]. Few scholars discussed the concept of global health until the 1990s, and the number of papers on this topic has risen rapidly in the subsequent decade [ 5 ] when global health was promoted under the Global Health Initiative - a global health plan signed by the U.S. President Barack Obama [ 6 ]. As a key part of the national strategy in economic globalization, security and international policies, global health in the United States has promoted collaborations across countries to deal with challenging medical and health issues through federal funding, development aids, capacity building, education, scientific research, policymaking and implementation.
Based on his experience working with Professor Zongfu Mao, the lead Editors-in-Chief, who established the Global Health Institute at Wuhan University in 2011 and launched the GHRP in 2016, Dr. Chen presented his own thoughts surrounding the definition of global health to the 2019 GHRP Editorial Board Meeting. Briefly, Dr. Chen defined global health with a three-dimensional perspective.
First, global health can be considered as a guiding principle, a branch of health sciences, and a specialized discipline within the broader arena of public health and medicine [ 5 ]. As many researchers posit, global health first serves as a guiding principle for people who would like to contribute to the health of all people across the globe [ 5 , 7 , 8 ].
Second, Dr. Chen’s conceptualization of global health is consistent with the opinions of many other scholars. Global health as a branch of sciences focuses primarily on the medical and health issues with global impact or can be effectively addressed through global solutions [ 9 , 10 , 11 , 12 , 13 , 14 , 15 , 16 ]. Therefore, the goal of global health science is to understand global medical and health issues and develop global solutions and implications [ 7 , 9 , 15 , 17 , 18 , 19 ].
Third, according to Dr. Chen, to develop global health as a branch of science in the fields of public health and medicine, a specialized discipline must be established, including educational institutions, research entities, and academic societies. Only with such infrastructure, can the professionals and students in the global health field receive academic training, conduct global health research, exchange and disseminate research findings, and promote global health practices [ 5 , 15 , 20 , 21 , 22 , 23 ].
Developmentally and historically, we have learned and will continue to learn global health from the WHO [ 1 , 4 , 24 , 25 ]. WHO’s projects are often ambitious, involving multiple countries, or even global in scope. Through research and action projects, the WHO has established a solid knowledge base, relevant theories, models, methodologies, valuable data, and lots of experiences that can be directly used in developing global health [ 26 , 27 , 28 , 29 ]. Typical examples include WHO’s efforts for global HIV/AIDS control [ 13 , 30 , 31 , 32 ], and the Primary Healthcare Programs to promote Health For All [ 33 , 34 ].
The definition of Global Health
From published studies in the international literature and our experiences in research, training, teaching and practice, our meeting reached a consensus-global health is a newly established branch of health sciences, growing out from medicine, public health and international health, with much input from the WHO. What makes global health different from them is that (1) global health deals with only medical and health issues with global impact [ 35 , 5 , 36 , 10 , 14 , 2 ] the main task of global health is to seek for global solutions to the issues with global health impact [ 7 , 18 , 37 ]; and (3) the ultimate goal is to use the power of academic research and science to promote health for all, and to improve health equity and reduce health disparities [ 7 , 14 , 15 , 18 , 38 ]. Therefore, global health targets populations in all countries and involves all sectors beyond medical and health systems, although global health research and practice can be conducted locally [ 39 ].
As a branch of medical and health sciences, global health has three fundamental tasks: (1) to master the spatio-temporal patterns of a medical and/or health issue across the globe to gain a better understanding of the issue and to assess its global impact [ 40 , 41 , 42 , 43 ]; (2) to investigate the determinants and influential factors associated with medical and health issues that are known to have global impact [ 15 , 40 , 41 , 42 , 43 ]; and (3) to establish evidence-based global solutions, including strategies, frameworks, governances, policies, regulations and laws [ 14 , 15 , 28 , 38 , 44 , 45 , 46 , 47 ].
Like public health, medicine, and other branches of sciences, global health should have three basic functions : The first function is to generate new knowledge and theories about global health issues, influential factors, and develop global solutions. The second function is to distribute the knowledge through education, training, publication and other forms of knowledge sharing. The last function is to apply the global health knowledge, theories, and intervention strategies in practice to solve global health problems.
Understanding the word “global”
Confusion in understanding the term ‘global health’ has largely resulted from our understanding of the word “global”. There are few discrepancies when the word ‘global’ is used in other settings such as in geography. In there, the world global physically pertains to the Earth we live on, including all people and all countries in the world. However, discrepancies appear when the word “global” is combined with the word “health” to form the term “global health”. Following the word “global” literately, an institution, a research project, or an article can be considered as global only if it encompasses all people and all countries in the world. If we follow this understanding, few of the work we are doing now belong to global health; even the work by WHO are for member countries only, not for all people and all countries in the world. But most studies published in various global health journals, including those in our GHRP, are conducted at a local or international level. How could this global health happen?
The argument presented above leads to another conceptualization: Global health means health for a very large group of people in a very large geographic area such as the Western Pacific, Africa, Asia, Europe, and Latin America. Along with this line of understanding, an institution, a research project or an article involving multi-countries and places can be considered as global, including those conducted in countries involved in China’s Belt and Road Initiative (BRI) [ 26 , 48 , 49 , 50 , 51 ]. They are considered as global because they meet our definitions of global health which focus on medical and health issues with global impact or look for global solutions to a medical or health issue [ 5 , 7 , 22 ].
One step further, the word ‘global’ can be considered as a concept of goal-setting in global health. Typical examples of this understanding are the goals established for a global health institution, for faculty specialized in global health, and for students who major or minor in global health. Although few of the global health institutions, scholars and students have conducted or are going to conduct research studies with a global sample or delivered interventions to all people in all countries, all of them share a common goal: Preventing diseases and promoting health for all people in the world. For example, preventing HIV transmission within Wuhan would not necessarily be a global health project; but the same project can be considered as global if it is guided by a global perspective, analyzed with methods with global link such as phylogenetic analysis [ 52 , 53 ], and the goal is to contribute to global implications to end HIV/AIDS epidemic.
The concept of global impact
Global impact is a key concept for global health. Different from other public health and medical disciplines, global health can address any issue that has a global impact on the health of human kind, including health system problems that have already affected or will affect a large number of people or countries across the globe. Three illustrative examples are (1) the SARS epidemic that occurred in several areas in Hong Kong could spread globally in a short period [ 11 ] to cause many medical and public health challenges [ 54 , 55 ]; (2) the global epidemic of HIV/AIDS [ 13 ]; and the novel coronavirus epidemic first broke out in December 2019 in Wuhan and quickly spread to many countries in the world [ 56 ].
Along with rapid and unevenly paced globalization, economic growth, and technological development, more and more medical and health issues with global impact emerge. Typical examples include growing health disparities, migration-related medical and health issues, issues related to internet abuse, the spread of sedentary lifestyles and lack of physical activity, obesity, increasing rates of substance abuse, depression, suicide and many other emerging mental health issues, and so on [ 10 , 23 , 36 , 42 , 57 , 58 , 59 , 60 ]. GHRP is expecting to receive and publish more studies targeting these issues guided by a global health perspective and supports more researchers to look for global solutions to these issues.
The concept of global solution
Another concept parallel to global impact is global solution . What do we mean by global solutions? Different from the conventional understanding in public health and medicine, global health selectively targets issues with global impact. Such issues often can only be effectively solved at the macro level through cross-cultural, international, and/or even global collaboration and cooperation among different entities and stakeholders. Furthermore, as long as the problem is solved, it will benefit a large number of population. We term this type of interventions as a global solution. For example, the 90–90-90 strategy promoted by the WHO is a global solution to end the HIV/AIDS epidemic [ 61 , 62 ]; the measures used to end the SARS epidemic is a global solution [ 11 ]; and the ongoing measures to control influenza [ 63 , 64 ] and malaria [ 45 , 65 ], and the measures taken by China, WHO and many countries in the world to control the new coronaviral epidemic started in China are also great examples of global solutions [ 66 ].
Global solutions are also needed for many emerging health problems, including cardiovascular diseases, sedentary lifestyle, obesity, internet abuse, drug abuse, tobacco smoking, suicide, and other problems [ 29 , 44 ]. As described earlier, global solutions are not often a medical intervention or a procedure for individual patients but frameworks, policies, strategies, laws and regulations. Using social media to deliver interventions represents a promising approach in establishment of global solutions, given its power to penetrate physical barriers and can reach a large body of audience quickly.
Types of Global Health researches
One challenge to GHRP editors (and authors alike) is how to judge whether a research study is global? Based on the new definition of global health we proposed as described above, two types of studies are considered as global and will receive further reviews for publication consideration. Type I includes projects or studies that involve multiple countries with diverse backgrounds or cover a large diverse populations residing in a broad geographical area. Type II includes projects or studies guided by a global perspective, although they may use data from a local population or a local territory. Relative to Type I, we anticipate more Type II project and studies in the field of global health. Type I study is easy to assess, but caution is needed to assess if a project or a study is Type II. Therefore, we propose the following three points for consideration: (1) if the targeted issues are of global health impact, (2) if the research is attempted to understand an issue with a global perspective, and (3) if the research purpose is to seek for a global solution.
An illustrative example of Type I studies is the epidemic and control of SARS in Hong Kong [ 11 , 67 ]. Although started locally, SARS presents a global threat; while controlling the epidemic requires international and global collaboration, including measures to confine the infected and measures to block the transmission paths and measures to protect vulnerable populations, not simply the provisions of vaccines and medicines. HIV/AIDS presents another example of Type I project. The impact of HIV/AIDS is global. Any HIV/AIDS studies regardless of their scope will be global as long as it contributes to the global efforts to end the HIV/AIDS epidemic by 2030 [ 61 , 62 ]. Lastly, an investigation of cardiovascular diseases (CVD) in a country, in Nepal for example, can be considered as global if the study is framed from a global perspective [ 44 ].
The discussion presented above suggests that in addition to scope, the purpose of a project or study can determine if it is global. A pharmaceutical company can target all people in the world to develop a new drug. The research would be considered as global if the purpose is to improve the medical and health conditions of the global population. However, it would not be considered as global if the purpose is purely to pursue profit. A research study on a medical or health problem among rural-to-urban migrants in China [ 57 , 58 , 60 ] can be considered as global if the researchers frame the study with a global perspective and include an objective to inform other countries in the world to deal with the same or similar issues.
Think globally and act locally
The catchphrase “think globally and act locally” presents another guiding principle for global health and can be used to help determine whether a medical or public health research project or a study is global. First, thinking globally and acting locally means to learn from each other in understanding and solving local health problems with the broadest perspective possible. Taking traffic accidents as an example, traffic accidents increase rapidly in many countries undergoing rapid economic growth [ 68 , 69 ]. There are two approaches to the problem: (1) locally focused approach: conducting research studies locally to identify influential factors and to seek for solutions based on local research findings; or (2) a globally focused approach: conducting the same research with a global perspective by learning from other countries with successful solutions to issues related traffic accidents [ 70 ].
Second, thinking globally and acting locally means adopting solutions that haven been proven effective in other comparable settings. It may greatly increase the efficiency to solve many global health issues if we approach these issues with a globally focused perspective. For example, vector-borne diseases are very prevalent among people living in many countries in Africa and Latin America, such as malaria, dengue, and chikungunya [ 45 , 71 , 72 ]. We would be able to control these epidemics by directly adopting the successful strategy of massive use of bed nets that has been proven to be effective and cost-saving [ 73 ]. Unfortunately, this strategy is included only as “simple alternative measures” in the so-called global vector-borne disease control in these countries, while most resources are channeled towards more advanced technologies and vaccinations [ 16 , 19 , 74 ].
Third, thinking globally and acting locally means learning from each other at different levels. At the individual level, people in high income countries can learn from those in low- and mid-income countries (LMICs) to be physically more active, such as playing Taiji, Yoga, etc.; while people in LMICs can learn from those in high income countries to improve their hygiene, life styles, personal health management, etc. At the population level, communities, organizations, governments, and countries can learn from each other in understanding their own medical and health problems and healthcare systems, and to seek solutions for these problems. For example, China can learn from the United States to deal with health issues of rural to urban migrants [ 75 ]; and the United States can learn from China to build three-tier health care systems to deliver primary care and prevention measures to improve health equality.
Lastly, thinking globally and acting locally means opportunities to conduct global health research and to be able to exchange research findings and experiences across the globe; even without traveling to another country. For example, international immigrants and international students present a unique opportunity for global health research in a local city [ 5 , 76 ]. To be global, literature search and review remains the most important approach for us to learn from each other besides conducting collaborative work with the like-minded researchers across countries; rapid development in big data and machine learning provide another powerful approach for global health research. Institutions and programs for global health provides a formal venue for such learning and exchange opportunities.
Reframing a local research study as global
The purpose of this article is to promote global health through research and publication. Anyone who reads this paper up to this point might already be able to have a clear idea on how to reframe his/her own research project or article to be of global nature. There is no doubt that a research project is global if it involves multiple countries with investigators of diverse backgrounds from different countries. However, if a research project targets a local population with investigators from only one or two local institutions, can such project be considered as global?
Our answer to this question is “yes” even if a research study is conducted locally, if the researcher (1) can demonstrate that the issue to be studied or being studied has a global impact, or (2) eventually looks for a global solution although supported with local data. For example, the study of increased traffic accidents in a city in Pakistan can be considered as global if the researchers frame the problem from a global perspective and/or adopt global solutions by learning from other countries. On the other hand, a statistical report of traffic accidents or an epidemiological investigation of factors related to the traffic accidents at the local level will not be considered as global. Studies conducted in a local hospital on drug resistance to antibiotics and associated cost are global if expected findings can inform other countries to prevent abuse of antibiotics [ 77 ]. Lastly, studies supported by international health programs can be packaged as global simply by broadening the vision from international to global.
Is Global Health a new bottle with old wine?
Another challenge question many scholars often ask is: “What new things can global health bring to public health and medicine?” The essence of this question is whether global health is simply a collection of existing medical and health problems packaged with a new title? From our previous discussion, many readers may already have their own answer to this question that this is not true. However, we would like to emphasize a few points. First, global health is not equal to public health, medicine or both, but a newly emerged sub-discipline within the public health-medicine arena. Global health is not for all medical and health problems but for the problems with global impact and with the purpose of seeking global solutions. In other words, global health focuses primarily on mega medical and health problems that transcend geographical, cultural, and national boundaries and seeks broad solutions, including frameworks, partnerships and cooperation, policies, laws and regulations that can be implemented through governments, social media, communities, and other large and broad reaching mechanisms.
Second, global health needs many visions, methods, strategies, approaches, and frameworks that are not conventionally used in public health and medicine [ 5 , 18 , 22 , 34 ]. They will enable global health researchers to locate and investigate those medical and health issues with global impact, gain new knowledge about them, develop new strategies to solve them, and train health workers to deliver the developed strategies. Consequently, geography, history, culture, sociology, governance, and laws that are optional for medicine and public health are essential for global health. Lastly, it is fundamental to have a global perspective for anyone in global health, but this could be optional for other medical and health scientists [ 40 , 41 ].
Global Health, international health, and public health
As previously discussed, global health has been linked to several other related disciplines, particularly public health, international health, and medicine [ 3 , 5 , 7 , 18 , 22 ]. To our understanding, global health can be considered as an application of medical and public health sciences together with other disciplines (1) in tackling those issues with global impact and (2) in the effort to seek global solutions. Thus, global health treats public health sciences and medicine as their foundations, and will selectively use theories, knowledge, techniques, therapeutics and prevention measures from public health, medicine, and other disciplines to understand and solve global health problems.
There are also clear boundaries between global health, public health and medicine with regard to the target population. Medicine targets patient populations, public health targets health populations in general, while global health targets the global population. We have to admit that there are obvious overlaps between global health, public health and medicine, particularly between global health and international health. It is worth noting that global health can be considered as an extension of international health with regard to the scope and purposes. International health focuses on the health of participating countries with intention to affect non-participating countries, while global health directly states that its goal is to promote health and prevent and treat diseases for all people in all countries across the globe. Thus, global health can be considered as developed from, and eventually replace international health.
Challenges and opportunities for China to contribute to Global Health
To pursue A Community with a Shared Future for Mankind , China’s BRI , currently involving more than 150 countries across the globe, creates a great opportunity for Chinese scholars to contribute to global health. China has a lot to learn from other countries in advancing its medical and health technologies and to optimize its own healthcare system, and to reduce health disparities among the 56 ethnic groups of its people. China can also gain knowledge from other countries to construct healthy lifestyles and avoid unhealthy behaviors as Chinese people become more affluent. Adequate materials and money may be able to promote physical health in China; but it will be challenging for Chinese people to avoid mental health problems currently highly prevalent in many rich and developed countries.
To develop global health, we cannot ignore the opportunities along with the BRI for Chinese scholars to share China’s lessons and successful experience with other countries. China has made a lot of achievements in public health and medicine before and after the Open Door Policy [ 49 , 78 ]. Typical examples include the ups and downs of the 3-Tier Healthcare Systems, the Policy of Prevention First, and the Policy of Putting Rural Health as the Priority, the Massive Patriotic Hygiene Movement with emphasis on simple technology and broad community participation, the Free Healthcare System for urban and the Cooperative Healthcare System for rural residents. There are many aspects of these initiatives that other countries can emulate including the implementation of public health programs covering a huge population base unprecedented in many other countries.
There are challenges for Chinese scholars to share China’s experiences with others as encountered in practice. First of all, China is politically very stable while many other countries have to change their national leadership periodically. Changes in leadership may result in changes in the delivery of evidence- based intervention programs/projects, although the changes may not be evidence-based but politically oriented. For example, the 3-Tier Healthcare System that worked in China [ 79 , 80 ] may not work in other countries and places without modifications to suit for the settings where there is a lack of local organizational systems. Culturally, promotion of common values among the public is unique in China, thus interventions that are effective among Chinese population may not work in countries and places where individualism dominates. For example, vaccination program as a global solution against infectious diseases showed great success in China, but not in the United States as indicated by the 2019 measles outbreak [ 81 ].
China can also learn from countries and international agencies such as the United Kingdom, the United States, the World Health Organization, and the United Nations to successfully and effectively provide assistance to LMICs. As China develops, it will increasingly take on the role of a donor country. Therefore, it is important for Chinese scholars to learn from all countries in the world and to work together for a Community of Shared Future for Mankind during the great course to develop global health.
Promotion of global health is an essential part of the Working Together to Build a Community of Shared Future for Mankind. In this editorial, we summarized our discussions in the 2019 GHRP Editorial Board Meeting regarding the concept of global health. The goal is to enhance consensus among the board members as well as researchers, practitioners, educators and students in the global health community. We welcome comments, suggestions and critiques that may help further our understanding of the concept. We would like to keep the concept of global health open and let it evolve along with our research, teaching, policy and practice in global health.
Dunham GC. Today's global Frontiers in public health: I. a pattern for cooperative public health. Am J Public Health Nations Health. 1945;35(2):89–95.
Article CAS PubMed PubMed Central Google Scholar
Kickbusch I. Health promotion: a global perspective. Can J Public Health. 1986;77(5):321–6.
CAS PubMed Google Scholar
Kickbusch I. Global + local = glocal public health. J Epidemiol Community Health. 1999;53(8):451–2.
Kickbusch I. Mapping the future of public health: action on global health. Can J Public Health. 2006;97(1):6–8.
Article PubMed PubMed Central Google Scholar
Chen X. Understanding the development and perception of global health for more effective student education. Yale J Biol Med. 2014;87(3):231–40.
PubMed PubMed Central Google Scholar
Bristol N. Obama's plans for US and global health. Lancet. 2008;372(9652):1797–8.
Article PubMed Google Scholar
Koplan JP, Bond TC, Merson MH, Reddy KS, Rodriguez MH, Sewankambo NK, et al. Towards a common definition of global health. Lancet. 2009;373(9679):1993–5.
Peluso MJ, Encandela J, Hafler JP, Margolis CZ. Guiding principles for the development of global health education curricula in undergraduate medical education. Med Teach. 2012;34(8):653–8.
Brown TM, Cueto M, Fee E. The World Health Organization and the transition from international to global public health. Am J Public Health. 2006;96(1):62–72.
Friedrich MJ. Global obesity epidemic worsening. Jama-Journal of the American Medical Association. 2017;318(7):603.
Google Scholar
Hung LS. The SARS epidemic in Hong Kong: what lessons have we learned? J R Soc Med. 2003;96(8):374–8.
Institute of Medicine (US), Board on International Health. America's vital interest in global health: protecting our people, enhancing our economy, and advancing our international interests. Washington, D.C.: National Academies Press; 1997.
Katz IT, Ehrenkranz P, El-Sadr W. The global HIV epidemic what will it take to get to the finish line? Jama-Journal of the American Medical Association. 2018;319(11):1094–5.
Article Google Scholar
Kickbusch I. Global health diplomacy: how foreign policy can influence health. BMJ. 2011;342:d3154.
Ren R. The definition and characteristics of global health. Medicine & Philosophy. 2015;36(8A):1–3.
CAS Google Scholar
Strategies, The malERA Consultative Group on Integration. malERA: An updated research agenda for basic science and enabling technologies in malaria elimination and eradication. PLoS Med. 2017;14(11):e1002451.
Kickbusch I, Hein W, Silberschmidt G. Addressing global health governance challenges through a new mechanism: the proposal for a committee C of the world health assembly. J Law Med Ethics. 2010;38(3):550–63.
Merson MH, Black RE, Mills AJ. Global health: diseases, programs, systems and policies. Jones & Bartlett Learning, L.L.C: New York/Ontario/London; 2012.
The malERA Consultative Group on Integration Strategies. A research agenda for malaria eradication: cross-cutting issues for eradication. PLoS Med. 2011;8(1):e1000404.
Mao Z, Liu P, Xiang H. Reformation and renewal of the undergraduate education based on a global health perspective - an example of the College of Health at Wuhan University. Wuhan, China: Wuhan University Press; 2018.
Rowson M, Smith A, Hughes R, Johnson O, Maini A, Martin S, Yudkin JS, et al. The evolution of global health teaching in undergraduate medical curricula. Glob Health. 2012;8(1):35.
Rowson M, Willott C, Hughes R, Maini A, Martin S, Miranda JJ, Yudkin JS, et al. Conceptualising global health: theoretical issues and their relevance for teaching. Glob Health. 2012;8(1):36.
White SK. Public health at a crossroads: assessing teaching on economic globalization as a social determinant of health. Crit Public Health. 2012;22(3):281–95.
Khubchandani J, Simmons R. Going global: building a foundation for global health promotion research to practice. Health Promot Pract. 2012;13(3):293–7.
Kickbusch I, Silberschmidt G, Buss P. Global health diplomacy: the need for new perspectives, strategic approaches and skills in global health. Bull World Health Organ. 2007;85(3):230–2.
Agaku IT, Ayo-Yusuf OA, Vardavas CI, Connolly G. Predictors and patterns of cigarette and smokeless tobacco use among adolescents in 32 countries, 2007-2011. J Adolesc Health. 2014;54(1):47–53.
Nikaj S, Chaloupka FJ. The effect of prices on cigarette use among youths in the global youth tobacco survey. Nicotine Tob Res. 2014;16(S1):S16–23.
World Health Organization. WHO Framework Convention on Tobacco Control. Geneva, Switzerland World Health Organization; 2003.
Rao S, Aslam SK, Zaheer S, Shafique K. Anti-smoking initiatives and current smoking among 19643 adolescents in South Asia: findings from the global youth tobacco survey. Harm Reduct J. 2014;11(1):8.
Harman S. 15 years of 'War on AIDS': what impact has the global HIV/AIDS response had on the political economy of Africa? Rev Afr Polit Econ. 2015;42(145):467–76.
Raguin G, Girard PM. Toward a global health approach: lessons from the HIV and Ebola epidemics. Glob Health. 2018;14(1):1–4.
Stover J, Bertozzi S, Gutierrez JP, Walker N, Stanecki KA, Greener R, Ghys PD, et al. The global impact of scaling up HIV/AIDS prevention programs in low- and middle-income countries. Science. 2006;311(5766):1474–6.
Article CAS PubMed Google Scholar
Amofah GK. Ghana. Selective versus comprehensive primary health care. Trop Dr. 1994;24(2):76–8.
Article CAS Google Scholar
Magnussen L, Ehiri J, Jolly P. Comprehensive versus selective primary health care: lessons for global health policy. Health Aff (Millwood). 2004;23(3):167–76.
Brown H. WHO puts cancer on global health agenda. Lancet Oncol. 2004;5(11):644.
Degenhardt L, Stockings E, Patton G, Hall WD, Lynskey M. The increasing global health priority of substance use in young people. Lancet Psychiatry. 2016;3(3):251–64.
Alonso PL, Brown G, Tanner M, Integratio, maIERA Consultative Grp. A Research Agenda for Malaria Eradication: Cross-Cutting Issues for Eradication. Plos Medicine. 2011;8(1):e1000399.
Stuckler D, McKee M. Five metaphors about global-health policy. Lancet. 2008;372(9633):95–7.
Beaglehole R, Bonita R. What is global health. Glob Health Action. 2010;3:5142.
Chen X, Chen DG. Statistical methods for global health and epidemiology. Basel, Switzerland: Springer; 2019.
Hao YT, Chen X. Research methods in global health (textbook). Beijing, China: People' Health Publication House; 2018.
Labonte R, Schrecker T. Globalization and social determinants of health: introduction and methodological background (part 1 of 3). Glob Health. 2007;3(1):5.
Labonte R, Schrecker T. Globalization and social determinants of health: the role of the global marketplace (part 2 of 3). Glob Health. 2007;3(1):6.
Aifah A, Iwelunmor J, Akwanalo C, Allison J, Amberbir A, Asante KP, Weber MB, et al. The Kathmandu declaration on global CVD/hypertension research and implementation science: a framework to advance implementation research for cardiovascular and other noncommunicable diseases in low- and middle-income countries. Glob Heart. 2019;14(2):103–7.
Feachem R, Sabot O. A new global malaria eradication strategy. Lancet. 2008;371(9624):1633–5.
Petersen PE. World health organization global policy for improvement of oral health--world health assembly 2007. Int Dent J. 2008;58(3):115–21.
Singh N. A new global malaria eradication strategy: implications for malaria research from an Indian perspective. Trans R Soc Trop Med Hyg. 2009;103(12):1202–3.
Grimm S. China-Africa cooperation: promises, pratice and prospects. Journal of Contemporary China. 2014;23(90):993–1011.
Tang K, Li ZH, Li WK, Chen L. China's silk road and global health. Lancet. 2017;390(10112):2595–601.
Witvliet MI, Arah OA, Stronks K, Kunst AE. A global study on lone mothers: exploring the associations of self-assessed general health with motherhood types and gender inequality in 32 countries. Womens Health Issues. 2014;24(2):e177–85.
Zhu S, Zhu W, Qian W, He Y, Huang J. A China - Vietnam collaboration for public health care: a preliminary study. Glob Health Res Policy. 2019;4(1):23.
Rife BD, Mavian C, Chen X, Ciccozzi M, Salemi M, Min J, Prosperi MC. Phylodynamic applications in 21(st) century global infectious disease research. Glob Health Res Policy. 2017;2(1):13.
Zhou S, Cella E, Zhou W, Kong WH, Liu MQ, Liu PL, Chen X, et al. Population dynamics of hepatitis C virus subtypes in injecting drug users on methadone maintenance treatment in China associated with economic and health reform. J Viral Hepat. 2017;24(7):551–60.
Lee A, Abdullah AS. Severe acute respiratory syndrome: a challenge for public health practice in Hong Kong. J Epidemiol Community Health. 2003;57(9):655–8.
Abdullah AS, Thomas GN, McGhee SM, Morisky DE. Impact of severe acute respiratory syndrome (SARS) on travel and population mobility: implications for travel medicine practitioners. J Travel Med. 2004;11(2):107–11.
Li Q, Guan XH, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N Engl J Med. 2020.
Chen XG, Yu B, Gong J, Wang PG, Elliott AL. Social capital associated with quality of life mediated by employment experiences: evidence from a random sample of rural-to-urban migrants in China. Soc Indic Res. 2018;139(1):327–46.
Guo Y, Chen XG, Gong J, Li F, Zhu CY, Yan YQ, Wang L. Association between spouse/child separation and migration-related stress among a random sample of rural-to-urban migrants in Wuhan China. Plos One. 2016;11(4):e0154252.
Article PubMed PubMed Central CAS Google Scholar
Sinyor M, Tse R, Pirkis J. Global trends in suicide epidemiology. Current Opinion in Psychiatry. 2017;30(1):1–6.
Yu B, Chen XG, Elliott AL, Wang Y, Li F, Gong J. Social capital, migration stress, depression and sexual risk behaviors among rural-to-urban migrants in China: a moderated mediation modeling analysis. Anxiety Stress and Coping. 2019;32(4):362–75.
Jamieson D, Kellerman SE. The 90 90 90 strategy to end the HIV pandemic by 2030: can the supply chain handle it? J Int AIDS Soc. 2016;19(1):20917.
Lima VD, St-Jean M, Rozada I, Shoveller JA, Nosyk B, Hogg RS, Montaner JSG, et al. Progress towards the United Nations 90-90-90 and 95-95-95 targets: the experience in British Columbia. Canada J Int AIDS Soc. 2017;20(3):e25011.
Friede M, Palkonyay L, Alfonso C, Pervikov Y, Torelli G, Wood D, Kieny MP. WHO initiative to increase global and equitable access to influenza vaccine in the event of a pandemic: supporting developing country production capacity through technology transfer. Vaccine. 2011;29(S1):A2–7.
Palkonyay L, Fatima H. A decade of adaptation: regulatory contributions of the World Health Organization to the global action plan for influenza vaccines (2006-2016). Vaccine. 2016;34(45):5414–9.
McCoy D, Kembhavi G, Patel J, Luintel A. The Bill & Melinda Gates Foundation's grant-making programme for global health. Lancet. 2009;373(9675):1645–53.
World Health Organization. Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). Geneva, Switzerland; 2020.
Abdullah AS, Tomlinson B, Cockram CS, Thomas GN. Lessons from the severe acute respiratory syndrome outbreak in Hong Kong. Emerg Infect Dis. 2003;9(9):1042–5.
Ameratunga S, Hijar M, Norton R. Road-traffic injuries: confronting disparities to address a global-health problem. Lancet. 2006;367(9521):1533–40.
Naci H, Chisholm D, Baker TD. Distribution of road traffic deaths by road user group: a global comparison. Injury Prevention. 2009;15(1):55–9.
Kareem A. Review of global menace of road accidents with special reference to Malaysia- a social perspective. Malays J Med Sci. 2003;10(2):31–9.
Gubler DJ. The economic burden of dengue. Am J Trop Med Hyg. 2012;86(5):743–4.
Wettstein ZS, Fleming M, Chang AY, Copenhaver DJ, Wateska AR, Bartsch SM, Kulkarni RP, et al. Total economic cost and burden of dengue in Nicaragua: 1996-2010. Am J Trop Med Hyg. 2012;87(4):616–22.
Cheng H, Yang W, Kang W, Liu C. Large-scale spraying of bednets to control mosquito vectors and malaria in Sichuan. China Bull World Health Organ. 1995;73(3):321–8.
The malERA Consultative Group on Integration Strategies. A research agenda for malaria eradication: vector control. PLoS Med. 2011;8(1):e1000401.
Menzies NA, Hill AN, Cohen T, Salomon JA. The impact of migration on tuberculosis in the United States. Int J Tuberc Lung Dis. 2018;22(12):1392–403.
Liu Y, Chen XG, Li SY, Bin Y, Wang Y, Yan H. Path analysis of acculturative stress components and their relationship with depression among international students in China. Stress Health. 2016;32(5):524–32.
Li H, Liu XL, Cui D, Wang Q, Mao Z, Gang L, Sun J, et al. Estimating the direct medical economic disease burden of healthcare associated infections in Chinese public tertiary hospitals. 2017;29(5):440-450. Asia Pac J Public Health. 2017;29(5):440–50.
Blumenthal D, Hsiao W. Lessons from the East - China's rapidly evolving health care system. N Engl J Med. 2015;372(14):1281–5.
Chen Z. Launch of the health-care reform plan in China. Lancet. 2009;373(9672):1322–4.
Liu XZ, Wang JL. An introduction to China’s health care system. J Public Health Policy. 1991;12(1):104–16.
Patel M, Lee AD, Redd SB, Clemmons NS, McNall RJ, Cohn AC, Gastanaduy PA. Increase in measles cases - United States, January 1-April 26, 2019. Am J Transplant. 2019;19(7):2127–30.
Download references
Acknowledgements
We would like to thank those who had provided their comments for the improvement of the manuscript.
The work is funded by the journal development funds of Wuhan University.
Author information
Authors and affiliations.
Global Health Institute, Wuhan University, Wuhan, China
Xinguang Chen, Hao Li, Xiaohui Liang, Zongfu Mao, Nan Wang, Peigang Wang & Tingting Wang
Department of Epidemiology, University of Florida, Florida, USA
Xinguang Chen
School of Health Sciences, Wuhan University, Wuhan, China
Hao Li, Xiaohui Liang, Zongfu Mao, Nan Wang, Peigang Wang, Tingting Wang, Hong Yan & Yuliang Zou
Department of Global Health and Development, London School of Hygiene and Tropical Medicine, London, UK
Don Eliseo Lucero-Prisno III
Global Health Research Center, Duke Kunshan University, Kunshan, China
Abu S. Abdullah
Duke Global Health Institute, Duke University, Durham, North Carolina, USA
School of Public Health, Fudan University, Shanghai, China
Jiayan Huang
Consultant in Global Health, London, UK
Charlotte Laurence
School of Public Health, Guangxi Medical University, Guangxi, China
Global Health Research Center, Dalian Medical University, Dalian, China
School of Public Health, Sun Yat-sen University, Guangzhou, China
Shaolong Wu
You can also search for this author in PubMed Google Scholar
Contributions
Chen XG wrote the manuscript. LI H organized the meeting, collecting the comments and editing the manuscript. Lucero-Prisno DE integrated all the comments together. Abdullah AS, Huang JY, Laurence C, Liang XH, Ma ZY, Ren R, Wu SL, Wang N, Wang PG and Wang Tt all participated in the discussion and comments of this manuscript. Laurence C and Liang XH both provided language editing. The author(s) read and approved the final manuscript
Corresponding author
Correspondence to Hao Li .
Ethics declarations
Ethics approval and consent to participate.
Not applicable.
Consent for publication
The manuscript was sent to all the authors and they all agreed to submit it for publication.
Competing interests
The authors declare that they have no competing interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Chen, X., Li, H., Lucero-Prisno, D.E. et al. What is global health? Key concepts and clarification of misperceptions. glob health res policy 5 , 14 (2020). https://doi.org/10.1186/s41256-020-00142-7
Download citation
Received : 15 February 2020
Accepted : 09 March 2020
Published : 07 April 2020
DOI : https://doi.org/10.1186/s41256-020-00142-7
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Global health
- Global impact
- Global solution
- Global health sciences
- Global health theory
- global health education
- Global health development
Global Health Research and Policy
ISSN: 2397-0642
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Am J Trop Med Hyg
- v.87(3); 2012 Sep 5
The Importance of the Global Health Strategy from the U.S. Department of Health and Human Services
The world in which we live is more interconnected today than ever before. In an era when we can get anywhere on the planet in less than a day, and when the flow of persons and goods stretches worldwide, we must ensure that the systems for preventing, detecting, and containing disease stretch equally far. Likewise, we need to remain just as vigilant when it comes to safeguarding the food and drug products that go into our bodies.
For an illustration, let us look at Dulles Airport, a port of entry to the Washington, DC metropolitan region. In 2010, more than 6.4 million international passengers came through Dulles, and that is just one of three major airports in the area. Each day upward of one million persons drive across our borders, arrive at U.S. airports, or dock in our ports. What is more, we import half of the fruit and more than three-fourths of the seafood we consume, often from countries with far fewer safety controls than we enjoy here at home.
The notion that diseases or contamination somehow recognize geographic or political borders is a dangerous illusion. As my boss, Health and Human Services Secretary Kathleen Sebelius, often remarks, “We can no longer separate global health from America's health.”
Fortunately, the United States has a broad, diverse, and world-class range of experience and expertise in dealing with all manner of global health issues. Much of this work is performed within federal agencies throughout the government, through non-governmental organizations, and within research institutions. Although most work at my agency, the United States Department of Health and Human Services (HHS), is geared toward protecting and promoting the health of Americans domestically, we are no strangers to the global health environment. Each of our 11 agencies and 18 staff offices engages in global health activities, and we have placed more than 300 of our department's officials in more than 75 countries, providing on-the-ground guidance and input. Nor is global health a new area for HHS; we have been actively engaged in global health efforts for decades. As far back as 1948, HHS joined with the health ministries of other countries to create the World Health Organization (WHO), the health arm of the United Nations. Our scientists and epidemiologists have been at the forefront in the effort to eradicate smallpox; we invested heavily in tuberculosis, malaria, and human immunodeficiency virus/acquired immunodeficiency syndrome research, treatment, and prevention; and we have supported the development of new vaccines and treatments for neglected diseases of the world's poorest people. And our global health portfolio continues to grow.
With such a wide array of professionals and departments within HHS working on global efforts to prevent disease, promote health, and strengthen partnerships, we needed to find a way to pull together our work and bring it into a coherent whole. That is why Secretary Sebelius called for the creation of a unified department strategy for dealing with global health issues. In response, the Office of Global Affairs recently unveiled the HHS Global Health Strategy (GHS) at the beginning of 2012.
The GHS is the product of many months spent exploring the range of global health work being done within all of HHS; examining the rationale behind that work; identifying top priorities; and synchronizing the role of HHS in a comprehensive, cohesive strategy to guide us in developing programs that will have real impact and be mutually reinforcing. The strategy is based on several underlying principles, including using evidence-based knowledge to inform decisions; responding to local needs and building local capacity; and emphasizing prevention.
The strategy identifies 10 objectives into which we now have categorized the efforts within HHS on global health matters: the first three focus on surveying, preventing, and responding to outbreaks and disaster; the next two emphasize improving the safety of international supply chains and strengthening standards for food and drug and feed production; and two more encourage increased research and sharing best practices worldwide. The final three objectives look forward to the emerging challenges of the 21st century by encouraging global action to address the major current and emerging contributors to global death, illness, and disability; supporting President Obama's Global Health Initiative (GHI); and advancing health diplomacy.
By increasing our effectiveness in these 10 key areas, we aim to achieve, through global health action, three overall goals: protecting and promoting the health and well-being of Americans; providing leadership and technical expertise in science, policy, programs, and practice; and advancing United States interests in international diplomacy, development, and security.
So what exactly does HHS do in each of these objectives? In each instance, we are harnessing the power of what we already do very well throughout the agency while using the strategy as a roadmap to make sure we are maximizing dollars, impact, and results.
When thinking about the first cluster of three objectives, prevention, detection, and response, it is important to note that HHS is recognized globally for its unsurpassed technical expertise and experience in disease surveillance, notably through the Centers for Disease Control and Prevention. In concert with critical partners such as the U.S. Agency for International Development and the Department of Defense, we will continue to support countries and organizations to strengthen surveillance systems and make sure we are plugging gaps. We assist with improving workforce and laboratory capacity to support diagnosis for disease surveillance. And we ensure those surveillance efforts are timely, evidence-based, data-driven, and internationally shared and actionable to inform public health policies and decision-making.
When it comes to prevention, HHS agencies provide direct prevention-focused and preparedness-oriented support and technical support throughout the world. We support the development of sustainable capacities for addressing both public health emergencies and day-to-day public health needs. We facilitate the development, use, and evaluation of vaccines and other prevention strategies, such as vector control and safe drinking water. We support database and information technology infrastructure with global access for monitoring purposes, including early warning systems and monitoring holdings of dangerous pathogens. And we coordinate with global partners to disseminate public information and emergency notification when necessary.
In the event of public health emergencies, HHS is prepared and able to respond internationally as well as at home. We maintain a wealth of domestic and international scientific, technical, and operational expertise that is frequently called upon during and after international emergencies. We coordinate with others, including the U.S. Agency for International Development and WHO to investigate outbreaks, to treat the sick and injured, and to mitigate impact on people's lives. We support the development of sustainable response capacities and provide technical expertise in investigating disease outbreaks and identifying their cause. We collaborate with international partners to develop best practices for responding to natural and man-made disasters. And as laid out by the GHS, we will continue to develop policy frameworks, agreements, and operational plans to facilitate HHS decision-making in response to requests for emergency assistance.
With the second cluster of objectives, global supply chains and standards, the road forward is clear. Principally through the Food and Drug Administration, HHS works to enhance regulatory systems and global manufacturing and supply chains to ensure the safety of medical products, food, and feed. Our efforts help to identify key risks in the supply chain and we implement strategies to mitigate those risks in cooperation with other governments and international agencies. And we work to strengthen strategic regulatory partnerships that promote a safer, higher quality global supply of medical products, food, and feed.
Through our active membership in WHO and a range of specialized international agencies, HHS also continues to provide leadership to establish, strengthen, and implement science-based international health and safety standards. The agency supports multilateral efforts to improve global health policies, programs, and practices. To those ends, we work to ensure an appropriate leadership role for the United States in the development of science-based norms and standards. And we work to strengthen existing multilateral relationships while developing new strategic alliances to maximize the achievement of our global health goals.
Innovating biomedical and public health research and exchanging best practices globally are key to improving health and well-being across national borders. HHS places a strong emphasis on both of those areas and strives to accelerate scientific discovery to improve patient care. The National Institutes of Health serves as the global gold standard in biomedical research. Priorities identified within the GHS include addressing research linked to scientific opportunity, public health needs, and the evolving burden of disease. We support the rapid translation of research results into new or improved preventive, diagnostic, and treatment products and processes. And we encourage research that identifies causative pathways of the spread of infectious disease and other health threats.
HHS brings to the global health arena technical expertise in the areas of human resources for health, service delivery, and regulatory science and systems. We support collaborative health system strengthening activities, including workforce development. We promote global exchange of best practices and lessons learned to ensure that evidence supports decisions and program implementation. And we strive to address the underproduction and retention of health professionals in developing countries.
The final three objectives in the GHS position us for the future. As we move deeper into the 21st century, the global health challenges we face are changing. Shifting global disease burdens include cardiovascular disease, cancer, chronic respiratory illnesses, diabetes, environmental risk factors, and an aging population. In this area, HHS promotes the development, implementation, evaluation, and dissemination of cost-effective prevention, policies, and strategies for non-communicable diseases, just as we have done for decades for communicable diseases. We advance the integration of effective public health policies and trade policies. And we work to strengthen health system capacities to address the changing global patterns of death, illness, and disability by fostering evidence-based interdisciplinary practice and promoting integrated community approaches.
HHS and many of its agencies have participated actively in the development and implementation of the President's Global Health Initiative. The initiative is designed to improve health outcomes related to control of HIV/AIDS, TB, malaria, and neglected tropical diseases in low-income countries. GHI recently entered a second phase of the initiative, shifting the leadership of in country coordination from Washington D.C. to Ambassadors in the field. However the principles and design of the GHI remain the same, and countries continue to focus on the health of women, newborns, and children through programs for nutrition, safe water, and reproductive, maternal, and child health. HHS contributes to the achievement of GHI goals, focusing our efforts on county ownership and integration and coordination, health system engineering and the integration of public health services for prevention and control.
Finally, HHS currently works within the broader context of U.S. foreign policy to engage on health issues with diplomatic partners and to strengthen peer-to-peer technical, public health, and scientific relationships. The GHS outlines top priorities, including assigning health attaches to key U.S. embassies for international cooperation. We are working to establish a global health career track within HHS to formalize career opportunities and training for our staff working in global health, both domestically and internationally. We already partner with the Department of State to bolster knowledge about global health among the diplomatic corps. And we work to strengthen diplomatic knowledge, negotiation skills, and understanding of development principles for HHS field staff and technical health experts.
Although the GHS provides crucial coordination and guidance for HHS global health work, it also makes clear there is much to be done. Under each of the 10 objectives outlined above, there are a plethora of steps to be taken and critical work to do. My team, the Office of Global Affairs, is working on incorporating the GHS and its underlying principles into workplans throughout HHS, and we are prioritizing activities and partnerships while working with the entire U.S. government to improve coordination and communication.
To be certain, the Global Health Strategy is not an attempt to create an entirely new direction for HHS; rather it is meant to provide a clearer focus for our efforts in the coming years. We have ample evidence that no country can protect the health of its citizens alone. Our global health work is therefore not an addition to our efforts to improve health here in America, but rather a necessary extension of those efforts. Through robust cooperation with other nations and international organizations, we will continue to work to reduce the risks of disease, disability, and premature death for all our citizens, and in turn, all persons worldwide.
Author's address: Nils Daulaire, Office of Global Affairs, U.S. Department of Health and Human Services, 200 Independence Avenue, SW, Washington, DC 20201, E-mail: [email protected] .
Volume 16 Supplement 4
Health policy dialogue: lessons from Africa
- Open access
- Published: 18 July 2016
Global health initiatives in Africa – governance, priorities, harmonisation and alignment
- Aziza Mwisongo 1 &
- Juliet Nabyonga-Orem 1
BMC Health Services Research volume 16 , Article number: 212 ( 2016 ) Cite this article
23k Accesses
38 Citations
7 Altmetric
Metrics details
The advent of global health initiatives (GHIs) has changed the landscape and architecture of health financing in low and middle income countries, particularly in Africa. Over the last decade, the African Region has realised improvements in health outcomes as a result of interventions implemented by both governments and development partners. However, alignment and harmonisation of partnerships and GHIs are still difficult in the African countries with inadequate capacity for their effective coordination.
Both published and grey literature was reviewed to understand the governance, priorities, harmonisation and alignment of GHIs in the African Region; to synthesise the knowledge and highlight the persistent challenges; and to identify gaps for future research.
GHI governance structures are often separate from those of the countries in which they operate. Their divergent funding channels and modalities may have contributed to the failure of governments to track their resources. There is also evidence that basically, earmarking and donor conditions drive funding allocations regardless of countries’ priorities. Although studies cite the lack of harmonisation of GHI priorities with national strategies, evidence shows improvements in that area over time. GHIs have used several strategies and mechanisms to involve the private sector. These have widened the pool of health service policy-makers and providers to include groups such as civil society organisations (CSOs), with both positive and negative implications. GHI strategies such as co-financing by countries as a condition for support have been positive in achieving sustainability of interventions.
Conclusions
GHI approaches have not changed substantially over the years but there has been evolution in terms of donor funding and conditions. GHIs still largely operate in a vertical manner, bypassing country systems; they compete for the limited human resources; they influence country policies; and they are not always harmonised with other donors. To maximise returns on GHI support, there is need to ensure that their approaches are more comprehensive as opposed to being selective; to improve GHI country level governance and alignment with countries’ changing epidemiologic profiles; and to strengthen their involvement of CSOs.
The advent of global health initiatives (GHIs) has changed the landscape and architecture of health financing in low and middle income countries, particularly in Africa [ 1 ]. GHIs arose as a funding mechanism out of the need to advocate, mobilise and hasten funding, for some key health problems facing the globe [ 2 ]. More than 100 GHIs have been created over the last 20 years with the aim of assisting countries to achieve their health outcomes [ 2 ]. GHIs have mainly targeted disease conditions that affect poor countries, saving many lives [ 2 ].
In the last decade the African Region has seen improvements in health outcomes resulting from the substantial efforts of both governments and development partners [ 1 , 3 – 6 ]. Besides multilateral and bilateral assistance, which are important sources of funding for health development, the African Region continues to register an increasing number of health partnerships and initiatives. This has made the aid architecture complex [ 7 , 8 ].
Although partnerships and health initiatives provide an opportunity for health sector development, the variety of their funding levels, instruments for engagement with countries, focus, and scope of support creates challenges for the recipient countries [ 9 – 16 ]. The large number of health partnerships and initiatives also generates a wide range of issues and concerns in ensuring that they are aligned to sector priorities, and in preventing overburdening of government officials with extra demands [ 17 – 23 ]. GHIs are renowned for their large funding to countries. For example, three prominent GHIs, the World Bank’s Multi-country HIV/AIDS Program (MAP), the Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM) and the US President’s Emergency Plan for AIDS Relief (PEPFAR) have provided more than two-thirds of all direct external funding for scaling up HIV/AIDS prevention, treatment and care in resource-poor countries [ 15 ].
The term global health initiative has been a subject of debate [ 24 ]. Nervi [ 25 ] claims that several initiatives that have identified themselves as global are in fact bilateral and involve only one recipient country. There are contentions regarding GHI management approaches, particularly in regard to the fact that though several GHIs have their distinct governance structures, they require the services of the same human resources that support the health sector in the countries, which is viewed as burdensome [ 20 , 26 ]. There have also been concerns about the nature of support rendered by GHIs, particularly regarding its focus, level, scheduling and timing, conditions and restrictions, all of which are thought to water down the positive synergism of GHIs [ 13 , 22 ].
Alignment and harmonisation of partnerships and global health initiatives with national priorities are still challenges for the African countries with inadequate capacity for effective coordination of such undertakings [ 20 , 21 , 27 ]. In their stewardship efforts to strengthen health systems, governments are sometimes overwhelmed by partnerships and initiatives that have parallel approaches, which cause fragmentation of resources and hamper the holistic implementation of national health strategic plans [ 13 , 21 , 22 , 28 ]. Partnerships and their members have peculiar priorities and ways of working and, consequently, consensus is not always achieved at the country level [ 28 ]. The partners’ unique reporting frameworks, funding cycles, focus and scope make aligning interventions for health systems strengthening difficult [ 15 , 29 , 30 ]. In addition, there are concerns that an increasing number of initiatives focus on issues, themes or diseases rather than on comprehensive approaches to health development and health systems strengthening [ 13 , 22 , 26 , 31 ]. In this regard, there is a need to foster coherence of partnerships and health initiatives in the African Region in order to improve their complementarity and alignment. In addition, it is important to streamline partners’ efforts for harmonised action and greater mutual accountability and, to minimise duplications [ 22 ]. With Africa now embarking on the Sustainable Development Goals (SDGs) and aiming for universal health coverage, better understanding of GHI governance, priorities, harmonisation, and alignment is crucial. This will help develop strategies to improve GHI usefulness and impact on health. This paper mainly aims to help familiarise African governments with the peculiarities of the governance, priorities, harmonisation and alignment of GHIs for better implementation of their activities.
This was a rapid literature review. A formal definition or methodology does not exist for a rapid literature review [ 32 ], but authors such as Khangura et al. [ 33 ] believe that it is becoming important as a tool to inform policy-makers and decision-makers on specific topics. The term “evidence summaries” is preferred to literature review. Characteristically, a rapid review is a short overview of available literature for a research question or set of research questions related to a single topic. For this study, the operational definition of GHIs was based on their possession of the following characteristics:
Addresses a major health issue of international concern
Is an organised effort linking people, partners and organisations
Targets several countries
Focuses on specific diseases or selected interventions, commodities or services
Has the ability to generate resources for a country
Is time limited
The main objectives of this review were to (1) explore and understand GHI governance processes, priorities, and harmonisation and alignment with country priorities in the African Region, (2) summarise and document these findings, and (3) identify gaps in the literature for future research and systematic reviews. The first two objectives were relevant for improved functioning of GHIs in Africa.
Two researchers conducted the rapid review. They first agreed on the research question, including the typology, and then on the databases to search and the search terms. They searched all the relevant literature related to GHIs and/or global health partnership (GHP) and low income countries (LMICs). The databases used were PubMed, Web of Knowledge, Web of Science, Google Scholar as well as websites of English language publications. Both peer-reviewed and grey literature was included in the search, with preference and emphasis given to literature focusing on the implementation and operations of GHIs in developing countries and Africa. Twenty three papers were initially identified, thereafter the researchers made use of their reference lists to obtain an additional 27 papers. All types of studies in Africa on the subject of interest were included in the review. Both researchers extracted the data from the literature and collated and summarised them according to the themes of interest.
GHI governance structures
GHIs use various aid modalities in the countries they support and are generally criticised for their vertical governance structures [ 29 ]. They have a tendency to create their own country-level coordination groups or committees and programmes [ 34 ]. The four main GHIs, the GAVI Alliance, GFTAM, MAP and PEPFAR, for example, all have their distinct governance structures at the country level. The GAVI Alliance has a secretariat and a board at the global level but no staff in the countries. Decisions on vaccines are usually made by the Inter-agency Coordination Committee formed specifically for GAVI Alliance. In the case of the Global Fund, a secretariat and a board oversee GFATM’s functioning while a country coordinating mechanism and local fund agents operate at the country level [ 35 ]. United States’ GHIs have global AIDS coordinators and country teams coordinated through United States embassies. MAP is coordinated by the Global HIV/AIDS Programme and regional teams such as the AIDS Campaign Team for Africa and the South Asia Regional AIDS Team; the World Bank country director and national governments.
The persistent use of separate structures by GHIs is prompted by the weak state of the governance systems in Africa and other developing countries [ 1 ], the need to ensure effective use of funds, wider involvement of stakeholders, and to affect performance and outcomes. Evidence, however, shows that the separate and different structures have several negative consequences [ 8 , 13 , 29 ], including that (1) the countries are overburdened with the parallel and duplicative processes from the many GHIs [ 1 ]; (2) GHIs often bypass the existing donor coordination processes in the countries such as the Sector-wide Approach (SWAp) and the general budget support (GBS) mechanisms [ 29 ]; and (3) GHI operations generate the risk of competition for the limited skilled workforce [ 29 , 36 ]. It is clear that GHIs are preferred to governments as employers owing to their lucrative enumeration and incentives [ 13 , 36 ].
From the literature, GHIs are viewed as operating in a top-down manner with many of their restrictions being imposed from the global level. A vast majority of them are governed by boards consisting of a variety of partners with different backgrounds, aims and perspectives [ 25 ].
One of the main thrusts of GHIs is to foster involvement of civil society organisations (CSOs) in their activities, and they have several modalities for this [ 15 ]. Two common strategies are through CSO membership in GHI national committees and as recipients of GHI funds. Despite their good intentions, these approaches have been viewed as challenging, owing to the difficulties in ensuring CSO representativeness, capacity and accountability [ 13 ].
Funding modalities
Most GHI funding support is earmarked for specific areas, with HIV being more commonly supported. Earmarked support is off budget support with multiple reporting systems. GHIs are concerned about good governance, and in their quest to ensure that funds are allocated and reach the intended beneficiaries, they have created many fragmented channels [ 29 ]. For example, in Angola the resource flows for funds from GFTAM and the President’s Malaria Initiative are completely distinct from those of the Ministry of Finance [ 37 ]. This poses difficulties in tracking resource flows, as illustrated in Fig. 1 .
Fragmented financial flows for MOF, Global Fund and PMI in Angola. Source: Global Health Partnerships, Assessing Country Consequences, 2005
Examples from Burkina Faso and Mozambique illustrate how GHIs circumvent local financial systems in favour of their discrete systems. In Burkina Faso, the GAVI Alliance and GFTAM used a demand-driven approach to funding rather than the government’s SWAp system, which integrates single reports for all donors and provides decentralised funding to districts [ 38 ]. This was also observed in Mozambique, where the GAVI Alliance and PEPFAR support was not handled through the Ministry of Finance’s management process but by representatives or officials designated by the Ministry of Health [ 38 ]. However, there have been efforts by GHIs to reduce transaction costs, for example by providing resources commensurate with the challenge of absorbing aid, complementing existing country processes or systems, and improving communication.
Areas of support
GHIs mainly focus on communicable diseases [ 13 , 34 , 39 ]. A study by the World Health Organization Maximizing Positive Synergies Collaborative Group found out that HIV/AIDS had disproportionately the greatest GHI support compared with other diseases [ 13 ]. In fact, 60 % of the GHIs in that study targeted the big three diseases of HIV/AIDS, tuberculosis and malaria, with HIV/AIDS attracting the most GHIs [ 34 , 36 ]. It is reasonable to justify the concentration on HIV/AIDS, since it was responsible for high levels of mortality and morbidity before the introduction of antiretroviral drugs. By 2007, GFTAM, PEPFAR and MAP were contributing more than two-thirds of all external funding for HIV/AIDS and malaria in low resource countries [ 40 ]. This funding was committed to several areas that target HIV and related conditions such as tuberculosis [ 4 ]. Table 1 summarises the main characteristics and HIV/AIDS commitments of the three GHIs.
GHIs are also renowned for the part they play in raising the profile of most neglected diseases such as onchocerciasis, dengue, trachoma, tetanus and schistosomiasis. Evidence shows that GHIs have programmes for these diseases, which in the past have had a low political profile and prioritisation [ 41 ]. GHIs have three broad strategies for supporting neglected diseases: raising the profile of the diseases, improving the delivery of interventions, and donating drugs. But support for neglected diseases in developing countries is viewed as unsustainable, and the consequences can be dire where support programmes are terminated. For example, Uganda faced major problems with drug shortages for neglected diseases after the drug donation period ended [ 34 ].
GHIs do not address all the gaps in health provision. For example, very few GHIs focus on non-communicable diseases [ 13 ]. There have also been concerns that most GHIs do not deal with certain areas that have a significant contribution to disability-adjusted life year (DALYs) losses such as maternal and reproductive health, depressive disorders, alcohol dependence and road traffic accidents, or the rising cancer incidences [ 13 ]. Some of the literature argues that although technical support to countries is crucial, GHI support has not been very successful [ 29 ]. Some reasons for this include the unclear and lack of a structured approach to identifying the gaps, and coordinating demand and supply to the identified technical assistance needs. Technical assistance has been ad-hoc and driven by urgent and immediate needs at the country level, an approach that often is unsustainable [ 42 ]. According to Biesma et al. [ 18 ], there were also unmet needs in the technical support provided by GHIs, such as in linking planning and disease prevalence, training on management and planning, cost-benefit analyses, monitoring and evaluation, and across-country application of lessons. GHIs have been blamed for selectively supporting certain groups that are easy to reach, contributing to the widening of the inequity gap [ 12 , 29 ]. Much of the literature shows that GHIs are not completely aligned with the countries’ national strategic plans and often impose preconceived ideas [ 12 , 29 , 37 ].
Funding levels
Despite the structural adjustment programmes and the worldwide recession, developing countries have seen a rise in development assistance for health since the early 2000s [ 3 ]. From studies mapping GHIs and GHPs, it is evident that Africa has the most GHPs per country followed by Asia. Eastern and central Europe have the lowest numbers of GHPs [ 28 ]. There are indications that a correlation exists between the number of GHPs operating in a country and its per capita GDP [ 34 ]. In general, the lower the per capita GDP, the greater the number of GHPs in the country, although there are inconsistencies [ 34 ]. The development assistance for health per DALY for HIV/AIDS, tuberculosis and malaria has increased in particular. Between 2002 and 2006, 32 % of the official development assistance for health was for HIV/AIDS and mostly went through the main GHIs for HIV/AIDS, tuberculosis, malaria and childhood immunisation, including polio. In 2007, investment through these GHIs accounted for two-thirds of all external funding for HIV/AIDS, 57 % for tuberculosis and 60 % for malaria [ 13 ].
Substantial differences exist in the countries that have received GHI funding [ 43 ]. There is considerable variation in development assistance for health per DALY across regions and within regions as shown in Fig. 2 . This variability is highly influenced by income, burden of disease, political stability, and historical and political relations between specific donors and recipient countries [ 43 ].
Map showing cumulative 2002–07 development assistance for health (DAH) per all-cause disability-adjusted life-year (DALY). Source: Ravishankar N. et al. Financing for global health: tracking developmental assistance for health from 1990 to 2007: Lancet 2009; 373: 2113-24
GHIs include NGOs and CSOs in their support. Although the channelling of funds through NGOs by GHIs has been riddled with controversy, a substantial portion of GHI funding is earmarked for NGOs and CSOs [ 44 ]. For example, GFTAM had allocated 30 % of all its grants to civil society groups in the countries of its support [ 44 ]. GHIs contribute directly to raising the overall health budgets of countries through their funding, but in a few cases they have done so through other processes [ 18 ]. For example, in Benin GFTAM contributions raised the overall budget for health spending by about 15 % [ 18 ].
The conditions relating to funding disbursement and performance have put immeasurable pressure on some weak economies [ 22 , 29 , 45 ]. In some cases the countries have failed to withdraw the funds allocated to them by GHIs owing to the strictness of the associated conditions, such as the requirement for performance-based reporting and to follow strict quality assurance guidelines [ 46 ]. Tanzania is a good example of a country where the conditions imposed by the GFTAM and MAP posed challenges in accessing their funds [ 46 ].
At the implementation level, delays in disbursement of funds and bureaucratic processes affect the use and absorptive capacity of funds, sometimes necessitating their return to the GHIs [ 46 ]. There are concerns also that in future GHI support might have adverse implications on sustainability and macroeconomic stability at the country level owing to the selective nature funding [ 47 , 48 ]. This is in reference to activities or programmes initiated by GHIs that the countries are eventually forced to sustain, which might distort their funding architecture. Recently, however, some GHIs have introduced co-financing as a means to influence governments to contribute to activities, in a way ensuring some form of sustainability [ 31 ]. For example, the GAVI Alliance requires that the countries contribute to the procurement of some of their required vaccine doses. This policy encourages them to plan for financially sustainable immunisation programmes once GAVI Alliance support for new vaccines is phased out [ 31 ].
Alignment of GHIs with national strategic plans and priorities
There has been growing concern in various African countries over the alignment of GHI objectives with those of the national strategic plans [ 2 , 17 , 19 , 21 ]. One school of thought is that by nature, GHIs with their specific earmarked funding, inevitably will influence the countries that are highly donor dependent. GHIs’ disease focus has resulted in their shift from general health systems support [ 14 , 21 , 37 , 49 ].
Examples exist on how GHIs have imposed restrictions on countries, such as the rejection of Ugandan’s 2002 Round One crosscutting, systems-strengthening proposal by GFTAM in favour of a more disease-specific proposal [ 16 ]. Also, the requirement by GFTAM for Tanzania to drop its proposal for a programme for orphans and children and instead undertake one on an antiretroviral treatment programme [ 46 ]. The failure to contain the spread of the recent Ebola outbreak in West Africa has been associated with the global health governance mechanisms implemented through GHIs that have predetermined focuses to the detriment of health promotion and health systems strengthening in countries [ 7 ]. The tide is changing, however. Lesotho’s approach to the implementation of the new strategy for HIV prevention through voluntary medical male circumcision stands out as a good example of how countries can challenge the traditional structures of global health politics controlled by experts and funders from high income countries [ 50 ]. To make an informed, local decision, Lesotho’s policy-makers consulted national statistics to determine if male circumcision was an effective approach to addressing the spread of HIV [ 50 ].
PEPFAR has been criticised for failing to link its objectives with those of the national strategic plans of the countries it supports [ 36 , 40 ]. There is also evidence that it is global earmarks and donor conditionality that drive funding allocations regardless of countries’ diseases, health needs or priorities [ 1 , 40 ]. A study conducted across Mozambique, Uganda and Zambia found that PEPFAR provided consistent and same level of funding allocations in the three countries regardless of their epidemiological and health systems’ differences [ 18 ]. According to Mckinsey and Company, BMGF 2005 [ 37 ], the countries with strong integrated health plans, established funding mechanisms with donor participation, and clearly defined roles of central and district governments interact the best with GHIs. This was also seen in an evaluation of MAP that attributed the failure of its approach to countries’ lack of national plans prioritising the components of their HIV/AIDS programme [ 51 ].
The multisectoral approach to HIV/AIDS is recognised for its success and cited as an example to follow for other disease conditions. However, how that approach is implemented has been the subject of extreme argument among health departments that feel disempowered or are bypassed by some of the GHIs such as MAP that favour that approach [ 51 ]. The failure to understand that the HIV response was multisectoral led many countries to ignore World Bank efforts to alleviate HIV/AIDS [ 51 ]. GHIs such as GFTAM also are faced with challenges for their insistence on planning processes that involve the country coordinating mechanism, a mutisectoral, private–public committee. There was lack of trust between government agencies and NGOs, and in some instances governments did not want to recognise the coordinating mechanism [ 18 ]. There were concerns that some of the country coordinating mechanisms lacked the capacity to function satisfactorily and were influenced by a few powerful members. The use of these mechanisms and the existence of several of them for HIV made it difficult to achieve alignment [ 36 ]. The presence of separate planning structures for the GHIs and the countries has led to duplication of effort [ 36 ]. Some GHIs have attempted to improve the harmonisation of their approaches with the country planning processes. This has been done through several strategies, as outlined in Table 2 .
Donor harmonisation and coordination
For aid to be effective there needs to be harmonisation of the processes between donors and other partners at the country level [ 52 ]. Harmonisation of donor policies and practices and their alignment with national policies have occurred at various levels across the countries. The negative effects of poor donor harmonisation were reported in the early years of the GHIs [ 18 ]. Despite the efforts of the countries to improve coordination and harmonisation of all donors, partners and GHIs, in the real sense GHIs are rarely part of these initiatives, as they tend to operate through separate systems and cycles or schedules [ 45 ]. This is further compounded by the lack of in country presence and as such, not able to participate in country dialogues in a consistent manner. To date little harmonisation has occurred of GFTAM processes and pre-existing planning and funding mechanisms such as SWAp and joint interagency committees [ 26 , 53 ]. Evidence shows that GFATM’s requirement of separate reporting systems is associated with higher transaction costs [ 17 , 22 ]. PEPFAR’s conditions, lack of transparency and unwillingness to involve other donors in its planning processes are cited as hindrances to harmonisation and collective donor action [ 18 , 40 ].
The literature shows that over time improvements in harmonisation have occurred, with studies from 2004 to 2005 from across the countries indicating that GHIs are harmonising their approaches [ 49 ]. GFTAM’s agreement of 2004 to allow its funds to be channelled through Mozambique’s SWAp, the common fund, was seen as a pioneering example of how disease-specific programmes could learn and adapt [ 40 ]. A review of the Mozambican approach highlighted the fact that pooling of funds and participation in SWAp structures had given GFTAM a unique perspective on the Mozambican health sector, whilst enabling it to become a more harmonised and highly influential development partner [ 40 ]. Another example is the support of harmonisation in Nigeria and Namibia by GFTAM [ 18 ]. MAP projects through the World Bank have made several attempts to harmonise efforts in the countries, for example in Malawi, where they supported the country’s integrated service delivery approaches for pooling of resources and the national AIDS councils (NACs) [ 54 ]. Despite the improvement in the collaboration between PEPFAR and national systems in information sharing, there is still reluctance among GHIs to use national systems such as those of the Ministry of Finance or the reporting systems. PEPFAR has been reported as not being transparent with other GHIs working in the areas it deals with [ 40 ].
Monitoring and evaluation (M&E) of GHIs still is not merged with the national systems, which means that multiple M&E reports are being prepared at the national and district levels [ 11 ] with different requirements for the various programmes [ 37 ]. All the GHIs conduct their separate assessments, but often involve the same constrained health human resources available at the national and sub-national levels.
The literature shows contrasting perceptions of GFATM’s alignment with existing country M&E systems. In Cambodia, Uganda and Cameroon the use of GFATM project monitoring tools undermined national programmes and the Three Ones principle that requires countries use a single M&E system [ 14 ]. PEPFAR implementers collect large amounts of data that they do not generally share with government coordinating bodies or other donor agencies [ 18 ]. The World Bank, in its case, overburdens governments with extensive and complex procedural and reporting requirements for its MAP projects instead of using one strategic framework, one national authority and one M&E system [ 40 ].
The increasing funding for some specific health problems such as HIV/AIDS has forced many countries to make efforts for greater coordination of programmes and services at the national level. Several countries in Africa like Malawi, Zambia and Tanzania have benefited from the push by GFATM to institute mechanisms for coordination of actors at the national level. However, the incentives to ensure the functioning of the coordination efforts are weak and practice falls far short of the intent of the policy, especially at the sub-national level [ 40 ]. Further, involving all the relevant stakeholders, particularly NGOs, in coordination bodies is a challenge in many countries. The McKinsey study (2005) reported in Biesma et al. [ 18 ] found that Tanzania and the Democratic Republic of the Congo had at least four committees overseeing HIV/AIDS control, with little communication or commonalities among them.
Some positive effects of GHIs on coordination and planning have been reported. In Malawi for example, after the study of the policy project by the United States Agency for International Development in 2004 raised concern about the multiplicity of HIV/AIDS coordinating structures, the Malawi Partnership Forum was created in 2005 as the central coordination structure for development partners, overriding all other mechanisms [ 54 ].
GHI contribution to stakeholder involvement
By actively involving NGOs and CSOs in their programmes, GHIs have changed the mind-set and perception that health delivery is the responsibility of governments [ 55 ]. Almost all GHIs tend to involve the private sector in their work, using several strategies and mechanisms. PEPFAR, for example, avoids the public sector in channelling its funds, choosing to use mainly international NGOs that fund CSOs [ 40 , 56 ]. The Stop TB Partnership emphasises inclusive governance that incorporates the private sector, while GFATM’s country coordinating mechanisms have private sector representation on their committees. GHIs have been more effective than other financing mechanisms in diversifying stakeholder participation and involving NGOs and faith based organisations, enabling them to gain direct access to financial resources [ 45 , 57 ]. Studies conducted in Malawi, Benin and Zambia showed that opportunities provided by GFATM strengthened public–private collaboration through allowing NGOs to establish umbrella organisations that helped to channel funds through principal recipients to sub-recipients [ 57 ]. There are still gaps, however, in the involvement of the private sector, and perceptions about how well GHIs are working with other stakeholders are contradictory [ 19 ]. There is evidence that some of the NGOs and CSOs do not have the capacity to implement GHI activities or absorb their funds [ 55 ]. Also, some indigenous NGOs have not been targeted nor reached with GHI funding, meaning that a few NGOs and CSOs dominate and benefit from GHI funding [ 15 ].
GHI commitments have been timely in providing the support necessary to handle diseases affecting LMICs [ 2 , 41 ]. It is indisputable that without their support, coverage and access to disease-specific services such as those for HIV, tuberculosis and malaria would not have been possible for the LMICs [ 1 , 41 ]. GHI support in LMICs has been varied in nature, involving financial support, technical assistance and HSS [ 17 , 20 , 24 ].
The positive outcomes of GHI support have been accompanied with negative effects that have generated controversy about its value [ 18 , 19 , 45 ]. GHIs have been criticised for their influence on national health priorities, decreased domestic spending on health, misalignment between their priorities and country health needs, distraction of government officials from their general responsibilities for health, creation of parallel systems, internal migration of health workers, increased burdening of HRH, lowered quality of services owing to pressure to meet targets, and weak accountability of the nongovernmental sector they fund [ 2 , 20 , 21 , 24 , 27 , 56 ]. Despite being pro-poor, GHIs have not been able to directly address equity through poverty-reduction strategies, which has contributed to the growing inequalities in access to health services [ 12 , 15 , 22 ].
The African Region is continually striving to improve harmonisation and coordination of support from donors and partners [ 58 ]. The initiatives focusing on this include the Paris Declaration on Aid Effectiveness, the Accra Agenda for Action, International Health Partnership and HHA. All these have the common objective of ensuring that there is effective investment in low and middle income countries through financing of sustainable development initiatives. Such an objective can only be achieved by ensuring that aid goals are aligned with countries’ needs and priorities. It also requires that the countries have the upper hand in the decision and implementation of programmes, and that capacity is built and systems are strengthened for GHIs to work without affecting government functioning [ 59 , 60 ].
Study limitations
Rapid reviews are generally criticised for not being thorough in their searches. In order to mitigate this we conducted a thorough search using several sources of information including reference list so as not to miss any relevant study. Inherent in all literature reviews is the fact that, rigorous analysis is sometimes hampered by the content of existing studies. This was one of the main limitations of this study, since many of the recent studies had a similar study focus as previous ones. Despite this challenge, the review is an adequate reflection of the state of governance, priorities, harmonisation and alignment of GHIs in this setting.
This rapid review of literature, which includes studies from GHIs’ early and recent times, reveals that little has changed in their approaches. GHIs still operate in a vertical manner, bypass countries’ systems, compete for the limited human resources, influence countries’ policies and favour unsustainable interventions [ 10 , 13 , 45 ]. The following recommendations will help to maximise the benefits and reduce the unintended challenges posed by the current GHI approaches:
Future GHI support should be more comprehensive and less selective. It should include aspects for successful disease control such as provision of the necessary drugs through funding, donation or discounted pricing; funding for some operational costs; and technical assistance in line with identified systems gaps.
There should be emphasis on strengthening of the wider systems that include social, community and health systems. GTZ’s BACKUP Initiative, which allocates specific funding for health systems support which is not disease specific [ 38 ], could serve as an example for this.
GHIs should strive to improve country level governance by using existing structures such as SWAp or iHP+ mechanisms. This ideally should extend to the use of joint planning schedules, meetings and M&E systems in order to avoid duplication of effort and overburdening of the countries with parallel procedures.
Modernisation is changing the disease profile in Africa. Africa is facing an alarming level of non-communicable diseases. GHI support should align with such changes with time. Also GHIs should evaluate their performance on epidemiologic effectiveness.
GHIs should play an important role in promoting better governance in Africa through advocating for and stimulating generation and application of appropriate policies and approaches, and giving a special focus to transparency, accountability and performance.
To improve the involvement of NGOs and CSOs, GHIs should support and promote standardisation of processes and accountability by CSOs at the country level and foster the empowerment of indigenous NGOs and CSOs.
Abbreviations
CSOs, civil society organisations; DALY, disability-adjusted life year; GFATM, Global Fund to Fight AIDS, Tuberculosis and Malaria; GHIs, global health initiatives; GHP, global health partnership; HSS, health systems strengthening; MAP, World Bank’s Multi-country HIV/AIDS Program; NAC, national AIDS council; NGO, nongovernmental organisation; PEPFAR, US President’s Emergency Plan for AIDS Relief; WHO, World Health Organization.
WHO. Maximizing positive synergies between health systems and global health initiatives. Report on the Expert Consultation on Positive Synergies between Health Systems and Global Health Initiatives. Geneva: WHO; 2008.
Google Scholar
Cahill K, Flemming D, Conway M, Gupta S. Global health partnerships: assessing country consequences. In: High level Forum: Bill and Melinda Gates Foundation, Seattle USA; 2003; 92–103.
Shaw RP, Wang H, Kress D, Hovig D. Donor and domestic financing of primary health care in low income countries. Health Systems Reform. 2015;1(1):72–88.
Article Google Scholar
Komatsu R, Korenromp EL, Low-Beer D, Watt C, Dye C, Steketee RW, Nahlen BL, Lyerla R, Garcia-Calleja JM, Cutler J. Lives saved by Global Fund-supported HIV/AIDS, tuberculosis and malaria programs: estimation approach and results between 2003 and end-2007. BMC Infect Dis. 2010;10(1):109.
Article PubMed PubMed Central Google Scholar
WHO Regional Office for Africa. Atlas of Africa health statistics. WHO Regional Office for Africa; Brazaville Congo. 2014.
WHO. Global Health Observatory (GHO) data. http://www.who.int/gho/child_health/mortality/mortality/en/ . Accessed 10 Nov 2015. Geneva; 2015
Dentico. [Ebola and the global governance of health]. Recenti Progressi in Medicina. 2014;105(11):405–6.
PubMed Google Scholar
Lancet T. Who runs global health? Lancet. 2009;373(9681):2083.
Chkhatarashvili K, Gotsadze G, Rukhadze N. Effects of GFATM on Georgia's Health Ssystem Development. Tbilisi: Curatio International Foundation; 2008.
Harmonisation for Health in Africa. Mapping global health initiatives in the WHO African Region. Brazzaville: WHO Regional Office for Africa; 2015.
Hanefeld J. The impact of global health initiatives at national and sub-national level – a policy analysis of their role in implementation processes of antiretroviral treatment (ART) roll-out in Zambia and South Africa. AIDS Care. 2010;22(S1):93–102.
Article PubMed Google Scholar
Hanefeld J. How have global health initiatives impacted on health equity? Promot Educ. 2008;15(1):19–23.
Group WHOMPSC. An assessment of interactions between global health initiatives and country health systems. Lancet. 2009;373(9681):2137–69.
Grace C. Global Fund country case studies report. London: Department for International Development; 2004.
Cohn J, Russell A, Baker B, Kayongo A, Wanjiku E, Davis P. Using global health initiatives to strengthen health systems: a civil society perspective. Global Public Health. 2011;6(7):687–702.
Donoghue M, Brugha R, Walt G, Pariyo G, Ssengooba F. Global Fund tracking study – Uganda country report. Uganda: London School of Hygiene & Tropical Medicine, UK, and Institute of Public Health, Makerere University; 2005.
Ashley W, Wyss K, Shakarishvili G, Atun R, Don de Savigny D. Global health initiative investments and health systems strengthening: a content analysis of global fund investments. Globalisation Health. 2013;9(1):30.
Biesma RG, Brugha R, Harmer A, Walsh A, Spicer N, Walt G. The effects of global health initiatives on country health systems: a review of the evidence from HIV/AIDS control. Health Policy Plan. 2009;24(4):239–52.
Bornemisza O, Bridge J, Olszak-Olszewski M, Sakvarelidze G, Lazarus J. Health aid governance in fragile states: the Global Fund experience. Global Health Gov 2010;4(1)1-18.
Bowser D, Sparkes SP, Mitchell A, Bossert TJ, Bӓrnighausen T, Gedik G, Atun R. Global Fund investments in human resources for health: innovation and missed opportunities for health systems strengthening. Health Policy Plan. 2014;29:986–97.
Brugha R, Donoghue M, Starling M, Ndubani P, Ssengooba F, Fernandes B, Walt G. The Global Fund: managing great expectations. Lancet. 2004;364(9428):95–100.
Chima CC, Homedes N. Impact of global health governance on country health systems: the case of HIV initiatives in Nigeria. J Global Health 2015;5(1):010407.
Starling M, Brugha R, Fernandes B, Cliff J, Walt G. Global Fund Tracking study: Mozambique country report. Global Fund; London, London School of Hygiene and Tropical Medicine, 2005.
Atun R, Pothapregada SK, Kwansah J, Degbotse D, Lazarus JV. Critical interactions between the Global Fund-supported HIV programs and the health system in Ghana. J Acquir Immune Defic Syndr. 2011;57:S72–6.
Nervi L. Mapping a sample of global health partnerships: a recount of significant findings. Paper prepared at request of HSS Area/PAHO. Wahington: PAHO; 2007.
Warren AE, Wyss K, Shakarishvili G, Atun R, de Savigny D. Global health initiative investments and health systems strengthening: a content analysis of global fund investments. Global Health. 2013;9(1):30.
Brugha R, Kadzandira J, Simbaya J, Dicker P, Mwapasa V, Walsh A. Health workforce responses to global health initiatives funding: a comparison of Malawi and Zambia. Hum Resour Health. 2010;8(1):19.
Carlson C. Mapping global health partnerships: What they are, what they do and where they operate. DFID Health Resource Center; London, 2009.
Cruz VO, McPake B. Global health initiatives and aid effectiveness: insights from a Ugandan case study. Global Health. 2011;7(1):20.
Drew R, Purvis G. Strengthening health systems to improve HIV/AIDS programs in the Europe and Eurasia region using Global Fund resources. Washington, DC: USAID; 2006.
Zuber PL, El-Ziq I, Kaddar M, Ottosen AE, Rosenbaum K, Shirey M, Kamara L Duclos P. Sustaining GAVI-supported vaccine introductions in resource-poor countries. Vaccine. 2011;29(17):3149–54.
Tricco AC, Antony J, Zarin W, Strifler L, Ghassemi M, Ivory J, Perrier L, Hutton B, Moher D, Straus SE. A scoping review of rapid review methods. BMC Med. 2015;13(1):1.
Khangura S, Konnyu K, Cushman R, Grimshaw J, Moher D. Evidence summaries: the evolution of a rapid review approach. Syst Rev. 2012;1(1):1–9.
Buse K, Harmer AM. Seven habits of highly effective global public–private health partnerships: practice and potential. Soc Sci Med. 2007;64(2):259–71.
Sridhar D, Tamashiro T. Vertical funds in the health sector: Lessons for education from the Global Fund and GAVI. United Nations Educational, Scientific and Cultural Organization (UNESCO); Paris-France, 2009.
Lohman N. District health officer perceptions of PEPFAR’s influence on the health system in Uganda, 2005–2011. University of Washington; USA, 2014.
Bill and Melinda Gates Foundation. Global health partnerships: Assessing country consequences. Seattle: McKinsey & Company, Global Public Health Practice; 2005.
Caines K, Buse K, Carlson C, de Loor R, Druce N, Grace C, Pearson M, Sancho J. Assessing the impact of global health partnerships. DFID Health Resource Centre, London; 2004.
McCoy D, Kinyua K. Allocating scarce resources strategically - an evaluation and discussion of the Global Fund's pattern of disbursements. PLoS one; 2012;7(5):e 34749.
Oomman N, Bernstein M, Rosenzweig S. Following the funding for HIV/AIDS: A comparative analysis of the funding practices of PEPFAR the Global Fund and World Bank MAP in Mozambique, Uganda and Zambia; Center for Global Health; Washington; 2007.
Caines K. Key Evidence from major studies of selected global health partnerships, High Level Forum on the Health MDGs background paper. London: Centre DHR, UK; 2005.
Storeng KT. The GAVI Alliance and the ‘Gates approach’ to health system strengthening. Global Public Health. 2014;9(8):865–79.
Ravishankar N, Gubbins P, Cooley RJ, Leach-Kemon K, Michaud CM, Jamison DT, Murray CJ. Financing of global health: tracking development assistance for health from 1990 to 2007. Lancet. 2009;373(9681):2113–24.
Wilkinson D, Brugha R, Hewitt S, Trap B, Eriksen J, Nielsen L, Weber W. Assessment of proposal development and review process of the Global Fund to Fight AIDS, Tuberculosis and Malaria- Assessment Report. Euro Health Group; 2006.
Banteyerga H, Kidanu A, Bennett S, Stillman K. The system-wide effects of the Global Fund in Ethiopia. Baseline study report; Bethesda MD. Partners for HealthReform Plus , Abt Associates Inc. 2005.
Starling M, Brugha R, Walt G. Global Fund Tracking Study: Tanzania country report. Lond Sch Hyg Trop Med; 2005
Le Gargasson J-B, Breugelmans JG, Mibulumukini B, Da Silva A, Colombini A. Sustainability of national immunization programme (NIP) performance and financing following Global Alliance for Vaccines and Immunization (GAVI) support to the Democratic Republic of the Congo (DRC). Vaccine. 2013;31(15):1886–91.
Ferrinho P, Dramé M, Tumusiime P. Perceptions of the usefulness of external support to immunization coverage in Chad: an analysis of the GAVI-Alliance cash-based support. Pan Afr Med J 2013;15:44.
Stillman K, Bennett S. Systemwide effects of the Global Fund: interim findings from three country studies. Bethesda MD. Partners for Health ReformPlus (PHRplus), Abt Associates, Inc, accessed from http://pdf.usaid.gov/pdf_docs/PNADF196.pdf . Accessed on the 15th April 2016 2005.
Bulled NL. Hesitance towards voluntary medical male circumcision in Lesotho: Reconfiguring global health governance. Global Public Health. 2015;10:757–72.
Ainsworth M, Vaillancourt D, Gaubatz JH. Committing to results: improving the effectiveness of HIV/AIDS assistance. An OED evaluation of the World Bank’s assistance for HIV/AIDS control. World Bank Publications; Washington DC. 2005.
African Forum and Network on Debt and development (AFRODAD); A crtitical asessment of AID management and donor harmonisation in Liberia: a case study. African Forum and Network on Debt and Development.Harare Zimbabwe; 2007.
Vujicic M, Weber SE, Nikolic IA, Atun R, Kumar R. GAVI: The Global Fund and World Bank support for human resources for health in developing countries. World Bank, Washington DC; 2011.
Mtonya B, Chizimbi S. Systemwide effects of the Global Fund in Malawi: final report. The Partners for Health ReformPlus project. Inc, Bethesda MD. 2006.
Doyle C, Patel P. Civil society organisations and global health initiatives: problems of legitimacy. Soc Sci Med. 2008;66(9):1928–38.
Cailhol J, Craveiro I, Madede T, Makoa E, Mathole T, Parsons AN, Van Leemput L, Biesma R, Brugha R, Chilundo B. Analysis of human resources for health strategies and policies in 5 countries in sub-Saharan Africa, in response to GFATM and PEPFAR-funded HIV activities. Global Health. 2013;9(1):52.
Smith O, Gbangbade S, Hounsa A, Miller-Franco L. Benin: system-wide effects of the Global Fund. Interim findings. 2005
Africa Union. Africa health strategy: 2007–2015. Third Session of the African Union Conference of Ministers of Health; African Union, Addiss Ababa - Ethiopia; 2007. 9–13.
Foresti M, Booth D, O’Neil T. Aid effectiveness and human rights: strengthening the implementation of the Paris Declaration. Overseas Development Institute report to the DAC; London, 2006.
Booth D. Aid effectiveness: bringing country ownership (and politics) back in. Confl Secur Dev. 2012;12(5):537–58.
Download references
Acknowledgements
We owe profound gratitude to Jehovah Jireh for sustenance during the entire process of writing this paper. The content of the article represent the analysis, perceptions and views of the authors only and does not represent the decisions or stated policies of the World Health Organization.
Declarations
This article has been published as part of BMC Health Services Research Volume 16 Supplement 4, 2016: Health policy dialogue: lessons from Africa. The full contents of the supplement are available online at http://bmchealthservres.biomedcentral.com/articles/supplements/volume-16-supplement-4 .
Availability of data and materials
Not applicable.
Authors’ contributions
Both authors contributed to the review of literature and drafting of the manuscript. AM led the drafting of the manuscript. All the authors read and approved the final manuscript.
Competing interests
Authors declare that they have no competing interests.
Consent for publication
Not applicable
Ethics approval and consent to participate
This study involved only the review of published literature and documents in the public domain and as such did not require ethical clearance.
Author information
Authors and affiliations.
Health Systems and Services Cluster, World Health Organization Regional Office for Africa, B.P. 06, Brazzaville, Congo
Aziza Mwisongo & Juliet Nabyonga-Orem
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Aziza Mwisongo .
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License ( http://creativecommons.org/licenses/by/4.0/ ), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated.
Reprints and permissions
About this article
Cite this article.
Mwisongo, A., Nabyonga-Orem, J. Global health initiatives in Africa – governance, priorities, harmonisation and alignment. BMC Health Serv Res 16 (Suppl 4), 212 (2016). https://doi.org/10.1186/s12913-016-1448-9
Download citation
Published : 18 July 2016
DOI : https://doi.org/10.1186/s12913-016-1448-9
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Global health initiatives
- GAVI Alliance
BMC Health Services Research
ISSN: 1472-6963
- General enquiries: [email protected]
Language selection
- Français fr
Budget 2024 Fairness for every generation
The 2024 federal budget is the government’s plan to build more homes, faster, help make life cost less, and grow the economy in a way that helps every generation get ahead.

How our economic plan can help you
Buy or rent a home.
We’re turbocharging the construction of homes across the country, and protecting the rights of renters, first-time buyers, and homeowners.
Tax-free First Home Savings Account
Over 750,000 Canadians have opened an account to save for their first down payment, and save faster with the help of tax relief.
Protecting Renters’ Rights
Our new Canadian Renters’ Bill of Rights will protect renters from unfair practices, make leases simpler, and increase price transparency.
Enhancing the Canadian Mortgage Charter
The Canadian Mortgage Charter is helping to protect homeowners who are struggling with rising mortgage payments. We are enhancing it to make it easier for younger Canadians to buy their first home, by making sure renters get credit for their rent payments and allowing up to 30-year mortgage amortizations on new builds for first-time home buyers.
Raise your family
Transforming Canada’s social safety net to help young parents with the cost of raising a family.
National School Food Program
A new National School Food Program will ensure that children have the nutritious meals they need to succeed and get a fair start in life.
More $10-a-day Child Care Spaces
We’re on track to securing Canada-wide $10-a-day child care in every province and territory by 2026, and fees have already been cut by 50 per cent everywhere, saving families thousands of dollars. We’re building more spaces and training more early childhood educators to ensure every family can access affordable child care.
Dental Care for Canadians Who Need It
The Canadian Dental Care Plan is already rolling out for uninsured Canadians with a family income of less than $90,000, to ensure everyone can afford the dental care they deserve. By 2025, nine million Canadians will be covered.
Get a good-paying job
Creating new opportunities for younger Canadians to get the education and skills they need for good-paying jobs.
Increasing Interest-Free Student Loans
Increasing Canada Student and Apprentice Loans and Grants, because everyone who wants to go to school should have the support they need to cover the costs.
More Work Experience and Skills Training for Youth
Helping young Canadians develop the skills and gain the work experience they need to achieve their dreams and get a good-paying job.
Canadian Apprenticeship Strategy
Supporting skilled trades workers by tooling up training programs and creating more apprenticeship positions to ensure young apprentices succeed.
Afford everyday essentials
Helping Canadians keep more of their money and build a better life by stabilizing the cost of everyday essentials.
Stabilizing the Cost of Groceries
Enhancing competition and monitoring grocers’ work to help stabilize prices, and lowering costs for the farmers who grow our food.
National Pharmacare Program
New programs to help with the cost of going to the dentist and pharmacy, including the cost of contraceptives and insulin, will further ease the financial burden on Canadians.
Cheaper Internet, Home Phone, and Cell Phone Plans
Lowering costs of plans, reducing junk fees, and giving Canadians more choice to switch providers and find better deals.
Retire safely and securely
After a lifetime of working hard—Canadians deserve to know they will be secure and comfortable in retirement.
A Stronger Canada Pension Plan
Enhancing the CPP to increase pension benefits by up to 50 per cent.
Supporting Long-Term Care
Advancing the Safe Long Term Care Act to support new national long-term care standards.
Bigger Benefits for Seniors
Increased Old Age Security and Guaranteed Income Supplement ensures seniors have the financial support they need in retirement.
Budget 2024 highlights
750,000+ Tax-Free First Home Savings Accounts opened by Canadians
Solving the Housing Crisis: Canada’s Housing Plan
Unlocking 3.87 million net new homes by 2031, to ensure everyone can find an affordable place to call home. And, we’re making it easier to rent while saving for that first home.
- Changing how we build homes
- Unlocking 250,000 new homes on public lands
- The strengthened Canadian Mortgage Charter
Learn more about making homes more affordable .
Fairness for younger generations
The government is helping restore fairness for Millennials and Gen Z by making education, housing, and the everyday costs of living more affordable.
- Increasing student grants and loans to keep up with the costs of an education
- Launching a new Youth Mental Health Fund for access to support they need
- Providing job placement and employment support opportunities through the Youth Employment and Skills Strategy
90,000 new job opportunities for youth
Investing $2.4 billion to secure Canada’s AI advantage
Economic growth and productivity
Budget 2024 makes investments in innovation, growth, and increased productivity in Canada.
Budget 2024 includes new measures to accelerate job growth in Canada’s AI sector and beyond, boost productivity by helping researchers and businesses develop and adopt AI, and ensure this is done responsibly.
- Investing in Canada’s AI ecosystem
- Enhancing research support with $1.8 billion more in core research grant funding
- Creating the Canadian Entrepreneurs’ Incentive
Learn more about the government’s plan to enhance innovation and productivity in Canada .
Unlocking 3.87 million new homes by 2031.
Over 1.1 million more Canadians employed today than before the pandemic.
Affordable child care is supporting a record high 85.4% labour force participation rate for working aged women.
Economic and Fiscal Overview
The state of canada’s economy.
The Canadian economy is outperforming expectations. Both the IMF and the OECD project Canada to see the strongest economic growth in the G7 in 2025. In the face of higher interest rates, Canada has avoided the recession that some had predicted. Headline inflation has fallen significantly from its June 2022 peak of 8.1 per cent to 2.8 per cent in February 2024.
Chart 6 Consumer Price Inflation Outlook

Note: Last data point is 2024Q4.
Sources: Statistics Canada; Department of Finance Canada March 2024 survey of private sector economists.
Economic and Fiscal Projections
We’re asking the wealthiest to pay a bit more, their fair share, to keep taxes lower on the middle class, and ensure the next generation inherits not more debt, but Canada’s prosperity.
Budget 2024 is investing in fairness for every generation while delivering on our fiscal objectives. Canada is maintaining the lowest net debt- and deficit-to-GDP ratios in the G7, preserving Canada’s long-term fiscal sustainability.
Chart 21 Federal Debt-to-GDP Ratio Under Economic Scenarios

Sources: Department of Finance Canada March 2024 survey of private sector economists; Department of Finance Canada calculations.
Improving Tax Fairness for Every Generation
Tax fairness is important for every generation, and it is particularly significant for younger Canadians.
To make the tax system more fair for 99.87 per cent of Canadians, the inclusion rate for capital gains—the portion on which tax is paid—for the wealthiest with more than $250,000 in capital gains in a year will increase from one-half to two-thirds. Only 0.13 per cent of Canadians with an average income of $1.42 million are expected to pay more personal income tax on their capital gains in any given year.
Principal residences will continue to be exempt from capital gains.
Chart 8.4 Canada Has the Lowest Marginal Effective Tax Rate in the G7

Backgrounders
- Key Measures (available in non-official languages)
- Key Measures
- More Affordable Homes
- A Stronger Social Safety Net
- Fairness for Younger Generations
- Economic Growth and Productivity
- Growing Small Businesses
- Safer, Healthier Communities
- A Fair Future for Indigenous Peoples
- Tax Fairness for Every Generation
- The New Canadian Entrepreneurs' Incentive
Related documents
- News Release
- Address by the Deputy Prime Minister and Minister of Finance
- Canada’s Consumer-Driven Banking Framework
- Statement and Impacts Report on Gender, Diversity, and Inclusion
- Legislative Measures
- Tax Measures: Supplementary Information
PDF downloads

Page details
IMAGES
VIDEO
COMMENTS
The strengthening of health systems was not, initially, a core purpose of most single-disease global health initiatives. But it is now. As the drive to reach the goals taught us, commodities, like pills, vaccines, and bednets, and the cash to buy them will not have an impact in the absence of delivery systems that reach the poor.
The positive contributions of global health initiatives. According to the Organisation for Economic Co-operation and Development, the health sector has become a major recipient of development assistance from just over US$ 6 billion in 1999 to US$ 13.4 billion in 2005. 1 The bulk of this increase can be credited to disease-targeted programmes ...
The pursuit of health equity is not just a moral obligation. It is also a strategic imperative that benefits both the global population and the business community. The role of businesses in promoting health equity. Businesses wield considerable influence and resources, which can be mobilized to champion the cause of health equity.
The boundaries between domestic and foreign agendas are becoming ever more blurred, and health concerns mix increasingly with high politics. It must be recognised that global problems cannot be solved without global solutions. Health can improve global security and enhance human rights, development and trade.
Weak health systems are almost certainly the greatest impediment to better health in the world today. They are the central obstacle that blunts the power of global health initiatives. The tuberculosis community clearly states the problem. The emergence of drug-resistant TB represents not just a failure of the control programme, but a failure of ...
The 30 included articles spanned a wide variety of journals and disciplinary affiliations of authors (e.g., public health, global health, nursing, medicine, dentistry, health systems, anthropology, bioethics, and occupational therapy). GHPs were often described as geographically focused in a single city or region within a global South country.
Implications for future global health strategies. Global health is increasingly determined by cross-border relations, policy priorities and particularly by security concerns; the securitisation of health is meanwhile considered a key feature of health governance (Labonté & Gagnon, Citation 2010).Multiple agents at national and international levels interact to target and fight cross-border ...
health is doomed to fail in the absence of a more efficient and rational use of available resources. The bad news emerging from the health economics literature is that there are still major uncertainties about what the specific contribution of health spending to growth really is and, consequently, the optimal level of investment for health
Global Health Initiatives is a term used to refer to organisations that integrate the efforts of stakeholders around the world to mobilise and disburse funds to address health challenges. They do so by supporting implementation of health programmes in low- and middle-income countries. Since 2000 the number and diversity of GHIs has increased ...
Global health has been getting much more attention lately, in settings as varied as the World Economic Forum, TIME Magazine, and even rock concerts—and for good reason. There is a new global determination to address the great disparity in health status between rich and poor people, communities, and nations, and this determination is reflected in explicit commitments of political will and ...
This paper reviews country-level evidence about the impact of global health initiatives (GHIs), which have had profound effects on recipient coun. ... whether marginalized populations access and benefit from GHI-funded programmes; and about the cost-effectiveness and long-term sustainability of the HIV and AIDS programmes funded by the GHIs ...
The global health agenda brings together two critical action spheres of our time: managing interdependence and globalization, and addressing the growing inequalities within and between nations ...
Global health initiatives were established to tackle increasing global health threats, reduce disparities within communities and between nations and contribute to a world where people live healthier, safer and longer lives. The global health initiatives collaborative work in the Region covers several areas: AIDS, tuberculosis and malaria ...
Over the last two decades, Global Health Initiatives have contributed to enormous progress in protecting lives and improving the health of people globally. However, as the epidemiological, financial, and political landscape across the world shifts and brings new challenges, there is a need to think about how their roles and responsibilities ...
Here are a few of the best reasons why global health matters to everyone, no matter where they are from. Healthier Communities Around the Globe. The first benefit of improving global health is a humanitarian one. By investing in healthcare around the world, including in areas not capable of building the required healthcare systems on their own ...
Uncover the Global Health Landscape. In an ever-evolving world, the realm of global health is marked by both opportunities and complexities. Our report takes a closer look at the dynamic trends that are shaping the future of global health initiatives. From innovative financing strategies that are revolutionizing healthcare funding to unforeseen ...
Introduction. Global health care is a challenging phenomenon that supports the development of new perspectives and approaches to solving global health concerns, including nutrition, infectious disease, cancer, and chronic illness. It is important to address global health as a driving force in international healthcare expenditures because it ...
Few scholars discussed the concept of global health until the 1990s, and the number of papers on this topic has risen rapidly in the subsequent decade when global health was promoted under the Global Health Initiative - a global health plan signed by the U.S. President Barack Obama . As a key part of the national strategy in economic ...
Here, we examine the dynamic, contemporary roles of students in global health activities, including health delivery. We focus on 3 themes that guide engagement: (1) fostering an enabling policy environment (eg, toward greater health equity); (2) understanding and working within the local context and governments' needs; and (3) leading ...
HHS and many of its agencies have participated actively in the development and implementation of the President's Global Health Initiative. The initiative is designed to improve health outcomes related to control of HIV/AIDS, TB, malaria, and neglected tropical diseases in low-income countries. GHI recently entered a second phase of the ...
The WHO Maximizing Positive Synergies Collaborative Group1 provides an impressive and informative assessment of the effects of global health initiatives on country health systems. Nowhere, however, in the lengthy report does the concept or the word "disability" feature (except once under the pejorative disability-adjusted life years, where it acts as a proxy of "loss").
The reduction of health inequities is an ethical imperative, according to the WHO Commission on Social Determinants of Health (CSDH). Drawing on detailed multidisciplinary evidence assembled by the Globalization Knowledge Network that supported the CSDH, we define globalisation in mainly economic terms. We consider and reject the presumption that globalisation will yield health benefits as a ...
The advent of global health initiatives (GHIs) has changed the landscape and architecture of health financing in low and middle income countries, particularly in Africa [].GHIs arose as a funding mechanism out of the need to advocate, mobilise and hasten funding, for some key health problems facing the globe [].More than 100 GHIs have been created over the last 20 years with the aim of ...
The UN Population Fund (UNFPA) has warned in a new report that political and social polarisation has put at risk decades of gains in ending inequalities in sexual and reproductive health and rights, widening the access divide and threatening future progress.In the report, released on April 17, the organisation says that a relentless, well organised effort to push back against human rights and ...
Budget 2024 includes new measures to accelerate job growth in Canada's AI sector and beyond, boost productivity by helping researchers and businesses develop and adopt AI, and ensure this is done responsibly. Investing in Canada's AI ecosystem. Enhancing research support with $1.8 billion more in core research grant funding.