
Research Topics & Ideas: Healthcare
100+ Healthcare Research Topic Ideas To Fast-Track Your Project

Finding and choosing a strong research topic is the critical first step when it comes to crafting a high-quality dissertation, thesis or research project. If you’ve landed on this post, chances are you’re looking for a healthcare-related research topic , but aren’t sure where to start. Here, we’ll explore a variety of healthcare-related research ideas and topic thought-starters across a range of healthcare fields, including allopathic and alternative medicine, dentistry, physical therapy, optometry, pharmacology and public health.
NB – This is just the start…
The topic ideation and evaluation process has multiple steps . In this post, we’ll kickstart the process by sharing some research topic ideas within the healthcare domain. This is the starting point, but to develop a well-defined research topic, you’ll need to identify a clear and convincing research gap , along with a well-justified plan of action to fill that gap.
If you’re new to the oftentimes perplexing world of research, or if this is your first time undertaking a formal academic research project, be sure to check out our free dissertation mini-course. In it, we cover the process of writing a dissertation or thesis from start to end. Be sure to also sign up for our free webinar that explores how to find a high-quality research topic.
Overview: Healthcare Research Topics
- Allopathic medicine
- Alternative /complementary medicine
- Veterinary medicine
- Physical therapy/ rehab
- Optometry and ophthalmology
- Pharmacy and pharmacology
- Public health
- Examples of healthcare-related dissertations
Allopathic (Conventional) Medicine
- The effectiveness of telemedicine in remote elderly patient care
- The impact of stress on the immune system of cancer patients
- The effects of a plant-based diet on chronic diseases such as diabetes
- The use of AI in early cancer diagnosis and treatment
- The role of the gut microbiome in mental health conditions such as depression and anxiety
- The efficacy of mindfulness meditation in reducing chronic pain: A systematic review
- The benefits and drawbacks of electronic health records in a developing country
- The effects of environmental pollution on breast milk quality
- The use of personalized medicine in treating genetic disorders
- The impact of social determinants of health on chronic diseases in Asia
- The role of high-intensity interval training in improving cardiovascular health
- The efficacy of using probiotics for gut health in pregnant women
- The impact of poor sleep on the treatment of chronic illnesses
- The role of inflammation in the development of chronic diseases such as lupus
- The effectiveness of physiotherapy in pain control post-surgery

Topics & Ideas: Alternative Medicine
- The benefits of herbal medicine in treating young asthma patients
- The use of acupuncture in treating infertility in women over 40 years of age
- The effectiveness of homoeopathy in treating mental health disorders: A systematic review
- The role of aromatherapy in reducing stress and anxiety post-surgery
- The impact of mindfulness meditation on reducing high blood pressure
- The use of chiropractic therapy in treating back pain of pregnant women
- The efficacy of traditional Chinese medicine such as Shun-Qi-Tong-Xie (SQTX) in treating digestive disorders in China
- The impact of yoga on physical and mental health in adolescents
- The benefits of hydrotherapy in treating musculoskeletal disorders such as tendinitis
- The role of Reiki in promoting healing and relaxation post birth
- The effectiveness of naturopathy in treating skin conditions such as eczema
- The use of deep tissue massage therapy in reducing chronic pain in amputees
- The impact of tai chi on the treatment of anxiety and depression
- The benefits of reflexology in treating stress, anxiety and chronic fatigue
- The role of acupuncture in the prophylactic management of headaches and migraines

Topics & Ideas: Dentistry
- The impact of sugar consumption on the oral health of infants
- The use of digital dentistry in improving patient care: A systematic review
- The efficacy of orthodontic treatments in correcting bite problems in adults
- The role of dental hygiene in preventing gum disease in patients with dental bridges
- The impact of smoking on oral health and tobacco cessation support from UK dentists
- The benefits of dental implants in restoring missing teeth in adolescents
- The use of lasers in dental procedures such as root canals
- The efficacy of root canal treatment using high-frequency electric pulses in saving infected teeth
- The role of fluoride in promoting remineralization and slowing down demineralization
- The impact of stress-induced reflux on oral health
- The benefits of dental crowns in restoring damaged teeth in elderly patients
- The use of sedation dentistry in managing dental anxiety in children
- The efficacy of teeth whitening treatments in improving dental aesthetics in patients with braces
- The role of orthodontic appliances in improving well-being
- The impact of periodontal disease on overall health and chronic illnesses

Tops & Ideas: Veterinary Medicine
- The impact of nutrition on broiler chicken production
- The role of vaccines in disease prevention in horses
- The importance of parasite control in animal health in piggeries
- The impact of animal behaviour on welfare in the dairy industry
- The effects of environmental pollution on the health of cattle
- The role of veterinary technology such as MRI in animal care
- The importance of pain management in post-surgery health outcomes
- The impact of genetics on animal health and disease in layer chickens
- The effectiveness of alternative therapies in veterinary medicine: A systematic review
- The role of veterinary medicine in public health: A case study of the COVID-19 pandemic
- The impact of climate change on animal health and infectious diseases in animals
- The importance of animal welfare in veterinary medicine and sustainable agriculture
- The effects of the human-animal bond on canine health
- The role of veterinary medicine in conservation efforts: A case study of Rhinoceros poaching in Africa
- The impact of veterinary research of new vaccines on animal health
Topics & Ideas: Physical Therapy/Rehab
- The efficacy of aquatic therapy in improving joint mobility and strength in polio patients
- The impact of telerehabilitation on patient outcomes in Germany
- The effect of kinesiotaping on reducing knee pain and improving function in individuals with chronic pain
- A comparison of manual therapy and yoga exercise therapy in the management of low back pain
- The use of wearable technology in physical rehabilitation and the impact on patient adherence to a rehabilitation plan
- The impact of mindfulness-based interventions in physical therapy in adolescents
- The effects of resistance training on individuals with Parkinson’s disease
- The role of hydrotherapy in the management of fibromyalgia
- The impact of cognitive-behavioural therapy in physical rehabilitation for individuals with chronic pain
- The use of virtual reality in physical rehabilitation of sports injuries
- The effects of electrical stimulation on muscle function and strength in athletes
- The role of physical therapy in the management of stroke recovery: A systematic review
- The impact of pilates on mental health in individuals with depression
- The use of thermal modalities in physical therapy and its effectiveness in reducing pain and inflammation
- The effect of strength training on balance and gait in elderly patients
Topics & Ideas: Optometry & Opthalmology
- The impact of screen time on the vision and ocular health of children under the age of 5
- The effects of blue light exposure from digital devices on ocular health
- The role of dietary interventions, such as the intake of whole grains, in the management of age-related macular degeneration
- The use of telemedicine in optometry and ophthalmology in the UK
- The impact of myopia control interventions on African American children’s vision
- The use of contact lenses in the management of dry eye syndrome: different treatment options
- The effects of visual rehabilitation in individuals with traumatic brain injury
- The role of low vision rehabilitation in individuals with age-related vision loss: challenges and solutions
- The impact of environmental air pollution on ocular health
- The effectiveness of orthokeratology in myopia control compared to contact lenses
- The role of dietary supplements, such as omega-3 fatty acids, in ocular health
- The effects of ultraviolet radiation exposure from tanning beds on ocular health
- The impact of computer vision syndrome on long-term visual function
- The use of novel diagnostic tools in optometry and ophthalmology in developing countries
- The effects of virtual reality on visual perception and ocular health: an examination of dry eye syndrome and neurologic symptoms
Topics & Ideas: Pharmacy & Pharmacology
- The impact of medication adherence on patient outcomes in cystic fibrosis
- The use of personalized medicine in the management of chronic diseases such as Alzheimer’s disease
- The effects of pharmacogenomics on drug response and toxicity in cancer patients
- The role of pharmacists in the management of chronic pain in primary care
- The impact of drug-drug interactions on patient mental health outcomes
- The use of telepharmacy in healthcare: Present status and future potential
- The effects of herbal and dietary supplements on drug efficacy and toxicity
- The role of pharmacists in the management of type 1 diabetes
- The impact of medication errors on patient outcomes and satisfaction
- The use of technology in medication management in the USA
- The effects of smoking on drug metabolism and pharmacokinetics: A case study of clozapine
- Leveraging the role of pharmacists in preventing and managing opioid use disorder
- The impact of the opioid epidemic on public health in a developing country
- The use of biosimilars in the management of the skin condition psoriasis
- The effects of the Affordable Care Act on medication utilization and patient outcomes in African Americans
Topics & Ideas: Public Health
- The impact of the built environment and urbanisation on physical activity and obesity
- The effects of food insecurity on health outcomes in Zimbabwe
- The role of community-based participatory research in addressing health disparities
- The impact of social determinants of health, such as racism, on population health
- The effects of heat waves on public health
- The role of telehealth in addressing healthcare access and equity in South America
- The impact of gun violence on public health in South Africa
- The effects of chlorofluorocarbons air pollution on respiratory health
- The role of public health interventions in reducing health disparities in the USA
- The impact of the United States Affordable Care Act on access to healthcare and health outcomes
- The effects of water insecurity on health outcomes in the Middle East
- The role of community health workers in addressing healthcare access and equity in low-income countries
- The impact of mass incarceration on public health and behavioural health of a community
- The effects of floods on public health and healthcare systems
- The role of social media in public health communication and behaviour change in adolescents
Examples: Healthcare Dissertation & Theses
While the ideas we’ve presented above are a decent starting point for finding a healthcare-related research topic, they are fairly generic and non-specific. So, it helps to look at actual dissertations and theses to see how this all comes together.
Below, we’ve included a selection of research projects from various healthcare-related degree programs to help refine your thinking. These are actual dissertations and theses, written as part of Master’s and PhD-level programs, so they can provide some useful insight as to what a research topic looks like in practice.
- Improving Follow-Up Care for Homeless Populations in North County San Diego (Sanchez, 2021)
- On the Incentives of Medicare’s Hospital Reimbursement and an Examination of Exchangeability (Elzinga, 2016)
- Managing the healthcare crisis: the career narratives of nurses (Krueger, 2021)
- Methods for preventing central line-associated bloodstream infection in pediatric haematology-oncology patients: A systematic literature review (Balkan, 2020)
- Farms in Healthcare: Enhancing Knowledge, Sharing, and Collaboration (Garramone, 2019)
- When machine learning meets healthcare: towards knowledge incorporation in multimodal healthcare analytics (Yuan, 2020)
- Integrated behavioural healthcare: The future of rural mental health (Fox, 2019)
- Healthcare service use patterns among autistic adults: A systematic review with narrative synthesis (Gilmore, 2021)
- Mindfulness-Based Interventions: Combatting Burnout and Compassionate Fatigue among Mental Health Caregivers (Lundquist, 2022)
- Transgender and gender-diverse people’s perceptions of gender-inclusive healthcare access and associated hope for the future (Wille, 2021)
- Efficient Neural Network Synthesis and Its Application in Smart Healthcare (Hassantabar, 2022)
- The Experience of Female Veterans and Health-Seeking Behaviors (Switzer, 2022)
- Machine learning applications towards risk prediction and cost forecasting in healthcare (Singh, 2022)
- Does Variation in the Nursing Home Inspection Process Explain Disparity in Regulatory Outcomes? (Fox, 2020)
Looking at these titles, you can probably pick up that the research topics here are quite specific and narrowly-focused , compared to the generic ones presented earlier. This is an important thing to keep in mind as you develop your own research topic. That is to say, to create a top-notch research topic, you must be precise and target a specific context with specific variables of interest . In other words, you need to identify a clear, well-justified research gap.
Need more help?
If you’re still feeling a bit unsure about how to find a research topic for your healthcare dissertation or thesis, check out Topic Kickstarter service below.

You Might Also Like:

15 Comments

I need topics that will match the Msc program am running in healthcare research please

Hello Mabel,
I can help you with a good topic, kindly provide your email let’s have a good discussion on this.

Can you provide some research topics and ideas on Immunology?

Thank you to create new knowledge on research problem verse research topic
Help on problem statement on teen pregnancy

This post might be useful: https://gradcoach.com/research-problem-statement/

can you provide me with a research topic on healthcare related topics to a qqi level 5 student

Please can someone help me with research topics in public health ?

Hello I have requirement of Health related latest research issue/topics for my social media speeches. If possible pls share health issues , diagnosis, treatment.

I would like a topic thought around first-line support for Gender-Based Violence for survivors or one related to prevention of Gender-Based Violence

Please can I be helped with a master’s research topic in either chemical pathology or hematology or immunology? thanks

Can u please provide me with a research topic on occupational health and safety at the health sector

Good day kindly help provide me with Ph.D. Public health topics on Reproductive and Maternal Health, interventional studies on Health Education

may you assist me with a good easy healthcare administration study topic

May you assist me in finding a research topic on nutrition,physical activity and obesity. On the impact on children
Submit a Comment Cancel reply
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
- Print Friendly
- Open access
- Published: 23 June 2020
How to strengthen a health research system: WHO’s review, whose literature and who is providing leadership?
- Stephen R. Hanney ORCID: orcid.org/0000-0002-7415-5932 1 ,
- Lucy Kanya 1 , 2 ,
- Subhash Pokhrel 1 ,
- Teresa H. Jones 1 &
- Annette Boaz 3
Health Research Policy and Systems volume 18 , Article number: 72 ( 2020 ) Cite this article
7510 Accesses
20 Citations
59 Altmetric
Metrics details
Health research is important for the achievement of the Sustainable Development Goals. However, there are many challenges facing health research, including securing sufficient funds, building capacity, producing research findings and using both local and global evidence, and avoiding waste. A WHO initiative addressed these challenges by developing a conceptual framework with four functions to guide the development of national health research systems. Despite some progress, more is needed before health research systems can meet their full potential of improving health systems. The WHO Regional Office for Europe commissioned an evidence synthesis of the systems-level literature. This Opinion piece considers its findings before reflecting on the vast additional literature available on the range of specific health research system functions related to the various challenges. Finally, it considers who should lead research system strengthening.
The evidence synthesis identifies two main approaches for strengthening national health research systems, namely implementing comprehensive and coherent strategies and participation in partnerships. The literature describing these approaches at the systems level also provides data on ways to strengthen each of the four functions of governance, securing financing, capacity-building, and production and use of research. Countries effectively implementing strategies include England, Ireland and Rwanda, whereas West Africa experienced effective partnerships. Recommended policy approaches for system strengthening are context specific. The vast literature on each function and the ever-growing evidence-base are illustrated by considering papers in just one key journal, Health Research Policy and Systems, and analysing the contribution of two national studies. A review of the functions of the Iranian system identifies over 200 relevant and mostly national records; an analysis of the creation of the English National Institute for Health Research describes the key leadership role played by the health department. Furthermore, WHO is playing leadership roles in helping coordinate partnerships within and across health research systems that have been attempting to tackle the COVID-19 crisis.
Conclusions
The evidence synthesis provides a firm basis for decision-making by policy-makers and research leaders looking to strengthen national health research systems within their own national context. It identifies five crucial policy approaches — conducting situation analysis, sustaining a comprehensive strategy, engaging stakeholders, evaluating impacts on health systems, and partnership participation. The vast and ever-growing additional literature could provide further perspectives, including on crucial leadership roles for health ministries.
Peer Review reports
Interest in strengthening health research systems has intensified following increasing recognition of the importance of research in achieving key goals such as universal health coverage [ 1 ] and the Sustainable Development Goals (SDGs) [ 2 ]. However, achieving progress in health research faces many challenges, including securing sufficient funds [ 3 , 4 , 5 , 6 , 7 , 8 , 9 ], building and retaining capacity [ 3 , 7 , 10 , 11 , 12 , 13 , 14 ], producing research findings, and using both local and global evidence [ 1 , 15 , 16 , 17 , 18 , 19 , 20 ].
Chalmers and Glasziou [ 21 ] dramatically highlighted the extent of the challenges facing health research by claiming, in 2009, that even where there was funding and capacity, up to 85% of all biomedical research was wasted because it asked the wrong questions, was poorly designed, or was either not published or poorly reported, with only about 50% of studies being published in full.
Many of these challenges have long been recognised and the adoption of a systems approach advocated. In 2000, the Bangkok Declaration on Health Research for Development promoted the importance of a systems approach, following consideration of how a health research system could “be integrated with a nation’s health development plan” [ 15 ]. It suggested that establishing and strengthening an effective health research system needed coherent and coordinated health research strategies [ 15 ]. National strategies should have specific combinations of various health research system components, tailored to the country’s circumstances.
The WHO’s Knowledge for Better Health initiative involved further work on these issues [ 3 , 16 ]. The Mexico Statement on Health Research, issued in 2004 by a Ministerial Summit, called for nations to take actions to strengthen their national health research systems (NHRSs). It was endorsed in 2005 by the Fifty-eighth World Health Assembly in a resolution committing its Member States to strengthening their NHRSs as a pathway to improve their overall health system [ 22 ].
As part of the initiative, Pang et al. [ 3 ] developed a conceptual framework to guide the analysis and strengthening of health research systems, including development of a health research strategy. While this can be used for planning, monitoring and evaluation of health research systems, it did not claim to provide a precise blueprint. The framework defined a health research system as “the people, institutions, and activities whose primary purpose in relation to research is to generate high-quality knowledge that can be used to promote, restore, and/or maintain the health status of populations; it should include the mechanisms adopted to encourage the utilization of research” [ 3 ].
The framework indicates the range of constituent components and how they can best be brought together into a coherent system. It identified four main functions for an effective system, namely stewardship, financing, capacity-building (or creating and sustaining resources), and producing and using research [ 3 ]. Each function is defined by operational components and consists of one or more of a total of nine such components.
Since then, progress is evidenced by analyses of developments in individual countries, including the National Institute for Health Research (NIHR) in England [ 23 , 24 , 25 ], and in repeat surveys conducted in various WHO regions, including Africa [ 4 , 26 , 27 ] and the Pan-American Health Organization (PAHO) [ 28 ]. However, as reported by those surveys and other publications, many challenges remain. For example, in February 2020 a new analysis by the WHO Global Observatory on Health R&D examined health research funding, concluding that “neglected diseases such as those on the WHO list of neglected tropical diseases remain very neglected in terms of R&D investments” [ 29 ].
Nevertheless, there are various initiatives underway, including in WHO’s Regional Office for Europe, which commissioned an evidence synthesis on the topic as part of its Action Plan to Strengthen the use of Evidence, Information and Research for Policy-making in the WHO European Region [ 18 ]. The synthesis is published in the WHO Region’s Health Evidence Network (HEN) report series and consists of a scoping review addressing the question “What is the evidence on policies, interventions and tools for establishing and/or strengthening NHRSs and their effectiveness?” [ 30 ].
The evidence synthesis focuses on the systems level and so primarily includes publications taking a systems approach at either the national or multi-national level. Not surprisingly, Health Research Policy and Systems ( HARPS ) is the single largest source of papers included in the HEN report. These were papers directly identified in the review’s search or papers included in the HEN report to illustrate a key point because they had been cited in one of the WHO reports or other systems-level collations of papers included in the synthesis.
While the system level papers did provide considerable data about each function, limited resources to conduct the scoping review meant that we had to exclude papers focusing solely on one specific function of a health research system or on just one field of health research. As acknowledged in the HEN report’s agenda for further research, there is a large number of publications (papers and grey literature) covering each function [ 30 ]. Therefore, reviewing all of these publications would be a major task but some exploration of the extent of the task, and the nature of such literature, could be informative. Furthermore, additional papers are continuously emerging, including from the various initiatives that are ongoing or just underway, for example, the European Health Research Network [ 31 ].
The three sections of this paper sequentially address the question of how to strengthen a health research system by:
Describing key points and conclusions from WHO’s HEN report.
Illustrating the nature of the ever-widening literature available on each function, or component, of a health research system by examining two sources in particular. First, the full range of papers published in HARPS in the 30 months up to February 2020. Second, the range of data gathered from publications or interviews that is included in detailed studies of the national health research systems in two countries – Iran [ 32 ] and England [ 33 ]; between them, these two papers also illustrate diverse aspects of the additional material that could be drawn upon.
Considering a key question in the analysis of the current and future initiatives, namely who is going to steer the development of health research systems? Here, information and insights from the HEN about this sometimes-controversial issue, along with wider continuing analysis, are drawn on in the more flexible and speculative way that can be undertaken in an Opinion piece compared to a formal evidence synthesis.
WHO’s review, whose literature and who is providing leadership?
Who’s review.
The evidence synthesis described by the HEN report [ 30 ] starts by describing the importance of NHRSs in helping to achieve universal health coverage [ 1 ] and the SDGs [ 2 ]. It goes on to analyse the challenges facing health research and describes how issues remain unresolved despite the development and application of a systems approach including WHO’s framework for health research systems [ 3 ]. Many countries do not have comprehensive national health research policies or strategies that would facilitate the introduction of a systems approach. Therefore, challenges remain around two key and overlapping sets of issues. First, how to develop a systems approach to maximise the benefits from the research resources available – this can be a challenge even in high-income countries with considerable research funding. Second, how best to strengthen each specific function and component of a health research system [ 30 ].
The HEN identifies two main systems-level approaches to strengthening NHRSs. The first is comprehensive and coherent strategies, which can be contained in either policy documents, such as those from the English NIHR [ 34 ], the Irish Health Research Board (HRB) [ 35 ] and the Rwandan Ministry of Health [ 14 ], or in specific legislation as in the Philippines [ 36 ]. The second systems-level approach involves partnerships and multi-country initiatives, especially with international organisations. Two initiatives from the West African Health Organization (WAHO) are particularly important examples [ 5 , 37 ]. Here, the ministries of health of the 15 West African member countries worked together in a joint initiative covering all the countries and with funding and expertise from a range of partners, including the Council on Health Research for Development (COHRED), the Canadian International Research Centre, the Special Programme for Research and Training in Tropical Diseases, and the Wellcome Trust. All WHO Regions have seen multi-country activities by WHO and/or COHRED to strengthen NHRSs, including the repeat surveys that identify areas for action [ 4 , 26 , 28 ].
Then, broadly using the WHO framework as the structure [ 3 ], the HEN identifies key points from systems-level literature on each of the four functions and nine components. The components of the stewardship and governance function include defining a vision, ethical review, research priority-setting, and appropriate monitoring and evaluation [ 3 ]. Consultation with health system stakeholders should enhance the relevance of the research priorities to the healthcare system, with examples of extensive priority-setting engagement activities sometimes being seen as a key aspect of building the NHRS as in Brazil [ 38 ]. Evaluating the impact of research on policy and practice should help researchers to focus on achieving such impact and was therefore promoted in the World Health Report 2013 [ 1 ].
Securing finance can involve obtaining funding from sources within the country and from external donors or multi-national organisations [ 30 ]. Targets for research expenditure, such as the 2% of national health expenditure set by the 1990 Commission on Health Research for Development [ 39 ], can usefully be brought into health research system strategies as in Rwanda [ 14 ]. Major health research strategies from countries within the European Union can highlight the importance of European Union funding as in France [ 40 ], Ireland [ 35 ] and Malta [ 41 ]. Requests for funding can be more effective when linked to other parts of the overall strategy, including identified priorities that need supporting through donor funding [ 42 ] and assessments of the benefits obtained from previous funding such as in England [ 24 ].
Capacity-building involves building, strengthening and sustaining the human and physical capacity to conduct, absorb and utilise health research [ 3 ]. In 2016, Santoro et al. [ 43 ] identified the generally low levels of research production in 17 countries of the former Soviet Union and south-eastern Europe and made recommendations for the sustained investment in training and career development of researchers, which should go beyond scholarships for training abroad and involve comprehensive strategies to ensure clear career structures. Strategies such as that from Inserm in France set out comprehensive plans for capacity-building [ 40 ] and strategies in both England and South Africa addressed priority gaps identified in the research capacity within the healthcare professions [ 34 , 44 ]. Donors can play an important part in building capacity but, recognising the need to avoid donor domination, often do so through partnerships. These can take diverse forms ranging from multi-country initiatives, such as that by WAHO, which included an initiative focusing on the challenges of post-conflict countries but was unable to meet all the needs [ 37 ], to accounts that focus on the partnership to address a broad range of capacity issues in a single country such as Malawi [ 7 ], to partnerships between individual institutions. Examples of the latter can feature particular challenges – the James Cook University in Australia worked with the Atoifi Adventist Hospital in Malaita, the most populous province of the Solomon Islands, to start establishing health research system capacity on the island using an inclusive, participatory approach [ 45 ]. Increasingly, there are also south–south partnerships, for example, an account of the Panamanian health research system described how the country’s first doctoral programme in biotechnology was established with support from Acharya Nagarjuna University in India [ 46 ]. The Rwandan strategy described plans to tackle the ‘brain drain’ through making the country an appealing place to conduct health research in terms of job requirements and providing opportunities for career advancement [ 14 ].
The three mutually reinforcing components of the producing and using research function encourage the production of scientifically valid findings that are relevant for users and communicated to them in an effective manner [ 30 ]. Major research funding bodies increasingly seek to address the waste issues raised by Chalmers and Glasziou [ 21 ] by working together in the Ensuring Value in Research (EViR) Funders’ Collaboration and Development Forum. It issued a consensus statement committing the organisations signing it to “require robust research design, conduct and analysis” [ 47 ]. The Forum is convened by the English NIHR, the Netherlands Organization for Health Research and Development, and the Patient-Centered Outcomes Research Institute (United States) with the active support of major research funding organisations from Australia, Ireland (HRB), Italy, Sweden and Wales, plus the Special Programme for Research and Training in Tropical Diseases [ 48 ]. The first WAHO intervention also worked to boost research publications, including by creating a regional peer-reviewed, multilingual journal [ 5 ]. How research is produced can increase the chance that the evidence will be used in the health system, for example, the English NIHR strategy noted that leading medical centres with substantial funding to conduct translational research can act as “early adopters of new insights in technologies, techniques and treatments for improving health” [ 34 ].
Fostering the use of research requires specific knowledge translation and management approaches that draw on both locally produced and globally available evidence. Various health research strategies promote the role of Cochrane, including in England, where a unified knowledge management system to meet the needs of various stakeholders, including patients and their carers, involves funding both Cochrane and a review centre focusing on the needs of the National Health System [ 34 ]. In Ireland, the HRB strategy facilitated evidence-informed decisions through promoting access to the Cochrane Library and supporting training in conducting high-quality Cochrane reviews [ 35 ]. South Africa Cochrane featured as an important element in the NHRS [ 44 ]. The Rwandan strategy stated that “The Government of Rwanda is committed to using research findings to make evidence-based decisions that will improve health in Rwanda” [ 14 ]. It aimed to orientate various functions, including agenda-setting, monitoring and evaluation, and capacity-building, towards facilitating this challenging aim. The World Health Report 2013 highlighted various mechanisms that health research systems could adopt, including EVIPNet (Evidence-informed Policy Network), to promote the use of research [ 1 , 49 ].
The review also considers the effectiveness of approaches to strengthening NHRSs. Several reviews identified the effectiveness of the comprehensive approach taken by Professor Dame Sally Davies in creating the English NHRS [ 23 , 25 , 50 ]. The title of one analysis, ‘NIHR at 10: 100 examples, 10 themes, 1 transformation’, emphasises that the success of the NIHR depended on a range of elements being brought together in one transformation [ 25 , 50 ]. One of the 10 themes was the involvement of patients in decisions about research priorities and processes and, based on this, another recent analysis highlighted England and Alberta (Canada) as having health research systems that had made important progress [ 51 ]. Davies herself reflected on the success of the NIHR and stated: “What we envisaged was integrating a health research system into the health care delivery system so that the two would become interdependent and synergistic ” [ 24 ]. WHO’s Regional Office for Africa drew on their series of surveys of the performance of countries in building NHRSs and analysed the data from the 2014 and 2018 surveys using the NHRS barometer that they developed to score progress on a range of items linked to the list of NHRS functions [ 11 , 26 ]. In the 2014 survey, the Rwandan system was identified as the best performing and it, along with the majority of systems, was reported to have further improved in the 2018 survey; by then, South Africa was reported to have the best performance in Africa. The surveys also illustrate how the multi-country approach makes a useful contribution to strengthening NHRSs by helping to target action. Furthermore, the WAHO interventions made some progress but, while the evaluations identified the importance of political will and leadership provided by WAHO’s parent organisation of West African states, they also emphasised that building capacity for a whole NHRS is a significant task requiring commitment over the long-term [ 17 , 37 ].
The HEN review collated a range of examples of tools for NHRS strengthening. These were identified from the systems level discussions of NHRS strategies and partnerships and/or the major reports calling for NHRS strengthening such as the World Health Report 2013 [ 1 ]. The HEN lists these in an Annex [ 30 ].
The discussion in the HEN draws on the literature that was included to identify five key policies that those responsible for strengthening NHRSs could consider [ 30 ], namely conduct context, or situational, analyses to inform strengthening activities [ 5 , 34 , 35 , 37 , 52 , 53 , 54 ], develop a comprehensive and coherent strategy [ 14 , 34 , 35 , 36 ], engage stakeholders in the development and operation of the strategy [ 7 , 23 , 34 , 35 , 38 , 41 , 44 , 51 , 55 , 56 , 57 , 58 , 59 ], adopt monitoring and evaluation tools that focus on the objectives of the NHRS, including health improvement [ 1 , 14 , 24 , 60 , 61 ], and develop partnerships [ 5 , 11 , 28 , 37 , 62 ]. Examples of the evidence to support or illustrate each policy are given in Table 1 .
In summary, therefore, this section shows that the WHO evidence synthesis, published as a HEN report [ 30 ], provides a firm basis for decision-making by policy-makers and research leaders looking to strengthen the health research system in their country. It analyses, in turn, the individual functions and components within a system and identifies a series of tools that can be used for strengthening many of them. Finally, this section highlights the five crucial policy approaches that the HEN report suggests can be applied as appropriate to the context of the country (Table 1 ).
Whose literature?
As noted above, the HEN was a scoping review and focused on the literature at the systems level rather than on publications (papers and grey literature) related solely to specific functions, types or fields of research [ 30 ]. Therefore, there is scope for further work to incorporate an even wider range of publications than the 112 included in the HEN review [ 30 ]. The discussion in the HEN suggests that further research could usefully take the form of a series of reviews on the extensive literature on each of the NHRS functions or components, which could then be collated [ 30 ]. Just two of the many available sources illustrate the nature of the vast literature available on each function, or component, of a health research system and the way the literature on that, and the system level developments, is ever-widening. First, we can examine the papers published in HARPS, the specialist journal in the field of building NHRSs. Second, we can focus on two very different but detailed studies of individual NHRSs – one conducted for a PhD thesis to show the 50 year history of the development of all the functions in the Iranian health research system [ 32 ] and the other an interview-based study to understand the factors behind the creation of the NIHR with its new strategy [ 33 ].
In terms of further reviews of the literature on specific functions or components, HARPS would probably be a key source. In the summer of 2017, an analysis by the retiring editors of the papers published in the journal from its inception in 2002 identified many papers that had been published on each of the functions or components of a health research system [ 63 ]. While this editors’ analysis was included in the HEN review because it organised its discussion of the papers at the systems level, the individual papers in it were, in general, only included in the HEN review if they, too, adopted a systems approach at the national or partnership level, or were also cited in a report such as the World Health Report 2013 [ 1 ]. Examples of such papers include Viergever et al. on priority-setting [ 59 ], Bates et al. on capacity-building [ 64 ], and Lavis et al. on the SUPPORT tools for evidence-informed policy-making [ 65 ]. Therefore, many additional papers related to specific functions (or fields) could be consulted, in a formal review or otherwise, in any future series of reviews, each with a narrow focus on strengthening a specific function.
To further inform this current Opinion piece, a quick ‘hand-search’ was conducted of the papers published in HARPS in the 30 months since the previous analysis in mid-2017 [ 63 ]. This again identified a wide range of papers on specific components, especially priority-setting, evaluation of research impacts, capacity-building and the translation of research (or knowledge mobilisation). Various papers linked the final two points and discussed capacity-building and knowledge translation [ 13 , 66 ]. Such a focus is entirely consistent with the aim described by the incoming editors in Autumn 2017 of bringing “all elements of the research–policy world together – such that the research which is done is useful and that it is used” [ 67 ]. In this more recent phase of HARPS , there have also been important papers on issues related to the policies ‘recommended’ at the end of the HEN and listed above, including the contribution of stakeholder engagement in research [ 68 ].
The more recent papers could sometimes provide useful further tools on specific functions. Their narrow focus meant they had not been directly included through the HEN search and, further, they had not been included in any of the major reports also used as sources for tools such as the World Health Report 2013 [ 1 ]. In some instances, this was because they were too recent, for example, the ISRIA statement by Adam et al. [ 69 ] describing the ten-point guidelines for an effective process of research impact assessment prepared by the International School on Research Impact Assessment (ISRIA). Even more recently, the Intervention Scalability Assessment Tool, developed by Milat et al. [ 70 ], was proposed for use not only by health policy-makers and practitioners for selecting interventions to scale up but also to help design research to fill evidence gaps. This analysis of the papers from just one journal reinforces the message that there is likely to be a plentiful supply of literature for a future review on any of the main specific components.
This message is further reinforced by a more detailed analysis of the papers in HARPS in the first 2 months of 2020. Articles on the main components of a NHRS were supplemented by some important papers on topics that are highly relevant but which feature less frequently in HARPS. These include a study aimed at reducing the research waste that arises from disproportionate regulation by examining the practices for exempting low-risk research from ethics review in four high-income countries [ 71 ], the Global Observatory’s paper on research funding described earlier [ 29 ], a study on the governance of national health research funding institutions [ 72 ], and one on a more recent topic of growing significance – an analysis of attempts to boost gender equality in health research [ 73 ]. Additionally, some of the papers on specific components, such as impact evaluation or use of evidence, are extending the analysis. Examples include consideration of how research impact assessments are implemented in practice within research organisations [ 74 ] and how evidence is used in decision-making in crisis zones [ 75 ]. To illustrate the volume of studies being produced, there has been a flurry of studies, in the first 2 months of 2020 alone, on the collaboration and coproduction of health research. The titles include ‘Building an integrated knowledge translation (IKT) evidence base: colloquium proceedings and research direction’ [ 76 ], ‘Using a ‘rich picture’ to facilitate systems thinking in research coproduction’ [ 77 ], ‘Exploring the evolution of engagement between academic public health researchers and decision-makers: from initiation to dissolution’ [ 78 ], ‘Research co-design in health: a rapid overview of reviews’ [ 79 ], and ‘Conceptualising the initiation of researcher and research user partnerships: a meta-narrative review’ [ 80 ].
Finally, another article in May 2020 presented a new conceptual model for health research systems to strengthen health inequalities research [ 81 ]. Here, we have focused on just one journal, HARPS, because it was the largest single source of papers in the HEN report, which totalled 140 publications (additional publications were included to the 112 in the review to help set the background, provide examples of key tools, etc). However, even with the review’s focus on the system level, HARPS only provided 22% (31 out of 140) of the publications; 31% (43 of 140) came from other journals and 47% (66 of 140) were other types of publication. If the focus was shifted to including papers on specific functions it is highly likely that there would be a higher proportion of papers from other journals.
The authors of two single-country papers on the development of the health research system, Mansoori [ 32 ] about Iran and Atkinson et al. [ 33 ] on the creation of the NIHR in England, both highlight the importance of context but also claim their findings could have wider application. Examining these two papers is also informative because of the differences between the studies, including one being located in a low- or middle-income country, and the other not.
Mansoori’s narrative review of studies addressing the health research system of Iran included 204 relevant and mostly national records, categorised using an approach informed by the functions and components of WHO’s NHRS framework [ 32 ]. The papers and grey literature documents included were all available in English or Persian, and mostly published in journals other than HARPS, and illustrate the vast literature available at a global level on the various components of a NHRS . They informed an impressively detailed account of the various NHRS components and the attempts to strengthen them. For example, the account of the development of the national level ethical overview includes a fully documented chronology of the progress over 25 years and some insightful analysis of how the progress was facilitated by the pivotal role of Professor Bagher Larijani, who was a prominent medical practitioner, leading researcher and founder of the Medical Ethics Research Centre in Iran. He was able to “use the confidence that Iranian authorities had in him as an opportunity” [ 32 ].
While Mansoori’s review was included in the HEN review, only a tiny fraction of the available data about Iran could be included, primarily in a brief description of the system’s effectiveness [ 30 ]. However, the full paper could usefully inform the approach of researchers and/or policy-makers planning a detailed analysis of their own NHRS prior to embarking on exercises to strengthen it, and “ [t] he findings emphasized that improvement of HRS functions requires addressing context-specific problems” [ 32 ]. As an illustration, Mansoori’s review identified a need for “ a more systematic, inclusive” approach to research priority-setting [ 32 ] and, in the same stream of research, she co-led just such a priority-setting exercise to help address the knowledge gaps related to achieving both Iran’s national health policies and the SDGs [ 82 ].
Atkinson et al. examined the creation of what might be viewed as the most successful attempt to strengthen a health research system in their paper ‘‘All the stars were aligned’? The origins of England’s National Institute for Health Research’ [ 33 ]. Compared with Mansoori, the authors adopted a different but equally detailed approach in their analysis, which was conducted principally through interviews and a witness seminar but also drew on the existing literature and documents [ 33 ]. They showed how the formation of the NIHR was led from the Department of Health by a key group driven by Sally Davies. They aimed to improve patient care through both the strengthening of evidence-based medicine and through boosting the infrastructure to facilitate pharmaceutical clinical trials that would also meet wider industrial and economic goals.
As with Mansoori’s study, consideration was given to how the full analysis could be informative to any planned detailed study or reforms in any other country. The key observations were similar to the recommendations from the HEN report with a focus on stakeholder engagement and building support: “ [t] wo measures likely to contribute to political support are to place the greatest emphasis on ‘problem’ rather than ‘investigation’ research, and to devote attention to measuring and reporting research ‘payback’ ” [ 33 ]. Atkinson et al.’s paper is also a link to the other main source considered here because it was a recent paper published in HARPS.
In summary, if further analysis and research beyond that in the WHO evidence synthesis [ 30 ] is thought to be relevant in the particular country looking to strengthen its health research system, this Opinion piece indicates some of the types of additional sources of information that are available and how they might be organised. The vast literature on each function and the ever-growing evidence base are illustrated by considering papers in just one key journal, HARPs, and analysing the contribution of two national studies. A review of the functions of the Iranian system identifies over 200 relevant, mostly national, records and an analysis of the creation of the English NIHR describes the key leadership role played from the health department.
Who is providing leadership?
The above analysis demonstrates that there is no shortage of useful material on which to draw when strengthening health research systems. However, key questions remain as to who might best lead or steer attempts to strengthen such a system.
The papers by both Mansoori [ 32 ] and Atkinson et al. [ 33 ] illustrate that, where a key committed individual has the capacity and opportunity to provide leadership, this can be a vital element in making progress. However, the institutional factors are also crucial.
The HEN developed the argument that a department or ministry of health will have a particular interest and perhaps experience in promoting research agendas that meet the needs of the healthcare system and in helping to develop mechanisms to use the findings from such research, where appropriate, to inform local policy and practice [ 30 ]. The health ministry or a research council responsible to it played an important role in the various systems identified above as being effective, as was also the case in the WAHO initiative [ 30 ]. In some cases, as with Zambia, more progress was made once the ministry of health elected to play a more important role, sometimes in place of other stakeholders [ 57 ]. Examples of the important role that health ministries can play were described in the 2013 World Health Report, including on Paraguay: “ the support of the Minister of Health backed by the President of Paraguay has been a key factor in the development of a national health research system” [ 1 ]. Additionally, naturally enough, the activities of the various WHO regional offices in boosting NHRSs tend to focus on working with the national ministries of health, including work in Europe [ 31 ] and by PAHO [ 28 ]. Conversely, several analyses illustrate that progress in strengthening the NHRS might be limited where key parts of the ministry of health, for whatever reason, do not provide support [ 9 , 83 ].
Nevertheless, some disadvantages or dangers were identified when the ministry of health plays the leading role. First, in England prior to the creation of the NIHR as well as in some other countries, the research funds controlled by the health ministry were sometimes appropriated by other parts of the health system when they were under particular pressure for resources [ 84 ]. Similarly, there have been a few reports that health research funding lost out when donor funds that had previously been allocated specifically for health research programmes were replaced by donations of funds to be allocated by the nation’s own health system according to its own priorities [ 85 , 86 ]. One way of attempting to mitigate the danger is, as undertaken by the NIHR and described by Atkinson, by building support for health research through measuring and reporting the payback from research [ 24 , 33 ].
The second danger arises because, traditionally, many researchers argued that the best science came when they had the freedom to identify the key research topics, rather than having priorities set by others [ 84 ]. Therefore, they argued, the responsibility for funding and organising health research should be left to organisations that are part of the research system and independent of the health system [ 84 ]. Furthermore, despite the growth of interest in coproduction approaches noted above, there have also been recent doubts raised about the assumption that coproduction is always the most appropriate approach [ 87 ]. This issue clearly requires sensitive handling. Indeed, Atkinson et al. [ 33 ] argue that one of the great successes of the NIHR is that this issue has been so skilfully handled by the NIHR that external input, or stakeholder engagement, in setting agendas has become widely accepted and the structures created give ministers a sense of ownership without sacrificing scientific independence.
The efforts of WAHO [ 5 , 37 ] and the WHO regional offices for Africa and PAHO [ 11 , 26 , 28 , 62 ] indicate that partnerships can be helpful. In Europe, the WHO regional office worked with Member States to create the European Health Research Network, which is intended to help nations with limited NHRSs who wish to make more progress [ 31 ].
Partnerships can provide important support and encouragement, but the evidence suggests there must be strong political will somewhere within the political and/or health systems for a health research system to be fully strengthened. The Central Asian countries in WHO’s European Region seem to provide an illustration of this point. A COHRED collaborative initiative successfully resulted in situation analyses being produced in each country and then jointly discussed as the basis for action [ 88 ], but according to the analysis by Santoro et al. [ 43 ], limited progress seems to have been made in the subsequent years.
The importance of partnerships and collaboration in focusing research efforts in an extreme crisis, with a leadership role for the WHO, has been seen in the race to find treatments for COVID-19 and vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes the COVID-19 disease [ 89 ]. In many NHRSs across the globe, including in the Philippines, scientists are coming together to participate in WHO’s Solidarity Trial, which will test the safety and effectiveness of various possible therapies for treating COVID-19 [ 90 ]. Sarah Gilbert, leader of Oxford University’s Jenner Institute’s work on developing one of the leading vaccine candidates explained that cooperation was vital for tackling the crisis: “Work is continuing at a very fast pace, and I am in no doubt that we will see an unprecedented spirit of collaboration and cooperation, convened by WHO, as we move towards a shared global goal of COVID-19 prevention through vaccination” [ 91 ]. A key issue going forward is how such cooperation can be built on in strengthening NHRSs into the future. For now, it is recommended that a prospective study be conducted to analyse all that is being done in different NHRSs to speed up research during the pandemic, with a view to taking lessons about cooperation, partnerships and other matters into strengthening NHRSs in the future [ 89 ].
The WHO evidence synthesis, published as a HEN report [ 30 ], provides a firm basis for decision-making by policy-makers and research leaders looking to strengthen the health research system in their country. It identifies five crucial policy approaches that can be applied as appropriate to the context of the country – conducting situation analyses, sustaining a comprehensive strategy, engaging stakeholders, evaluating impacts on health policies and practices, and partnership participation. It also analyses, in turn, the individual functions and components within a system and identifies a series of tools that can be used for strengthening many of them.
If further analysis and research is thought to be relevant in the particular country looking to strengthen its health research system, this Opinion piece indicates some of the types of additional sources of information that are available. The Opinion piece also discusses aspects of the sometimes-controversial question of who should lead or steer attempts to strengthen NHRSs. Again, the context of the particular nation will be crucial in determining the most appropriate course to take, as emphasised by both Mansoori [ 32 ] and Atkinson et al. [ 33 ], but at least some involvement of the ministry of health is likely to be beneficial; additionally, sometimes, key individuals can play a crucial leadership role in strengthening the whole system or one component. In countries with a less developed tradition of conducting health research, partnerships with other countries and/or with international organisations can help lead the progress and learning for all partners. The valuable role that international organisations, such as WHO, can play in leading partnerships and cooperation to strengthen health research systems is being highlighted during the COVID-19 crisis.
Overall, therefore, the full WHO HEN report not only provides a detailed analysis of NHRS strengthening, it also provides a structure within which an even wider and ongoing literature can be considered. Additionally, it contains a perhaps more nuanced account, on which this paper builds, of some aspects of the literature around the issue of who should provide leadership in developing NHRSs and identifies the importance of ministry of health involvement.
Availability of data and materials
The full details of the papers included in the Health Evidence Network Evidence Synthesis are provided in that report, which is cited in this paper as reference [ 30 ]. The additional analysis of papers from Health Research Policy and Systems was based on the open access publications.
Abbreviations
Council on Health Research for Development
Health Research Policy and Systems
Health Evidence Network
Health Research Board
National Health Research System
National Institute for Health Research
Pan-American Health Organization
- Sustainable Development Goals
West African Health Organization
World Health Organization. The World Health Report 2013: research for universal health coverage. Geneva: WHO; 2013. https://apps.who.int/iris/bitstream/handle/10665/85761/9789240690837_eng.pdf?sequence=2 . Accessed 19 Dec 2019.
Book Google Scholar
United Nations. Transforming our world: the 2030 agenda for sustainable development. General Assembly resolution 70/1. New York: UN; 2015. https://www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/1&Lang=E . Accessed 19 Dec 2019.
Google Scholar
Pang T, Sadana R, Hanney S, Bhutta ZA, Hyder AA, Simon J. Knowledge for better health: a conceptual framework and foundation for health research systems. Bull World Health Organ. 2003;81(11):815–20.
PubMed Google Scholar
Kirigia JM, Ota MO, Motari M, Bataringaya JE, Mouhouelo P. National health research systems in the WHO African Region: current status and the way forward. Health Res Policy Syst. 2015;13:61. https://doi.org/10.1186/s12961-015-0054-3 .
Article PubMed PubMed Central Google Scholar
Aidam J, Sombié I. The West African Health Organization’s experience in improving the health research environment in the ECOWAS region. Health Res Policy Syst. 2016;14:30. https://doi.org/10.1186/s12961-016-0102-7 .
Grépin KA, Pinkstaff CB, Shroff ZC, Ghaffar G. Donor funding health policy and systems research in low- and middle-income countries: how much, from where and to whom. Health Res Policy Syst. 2017;15:68. https://doi.org/10.1186/s12961-017-0224-6 .
Cole DC, Nyirenda LJ, Fazal N, Bates I. Implementing a national health research for development platform in a low-income country: a review of Malawi’s Health Research Capacity Strengthening Initiative. Health Res Policy Syst. 2016;14:24. https://doi.org/10.1186/s12961-016-0094-3 .
D'Souza C, Sadana R. Why do case studies on national health research systems matter? Identifying common challenges in low- and middle-income countries. Soc Sci Med. 2006;62(8):2072–8. https://doi.org/10.1016/j.socscimed.2005.08.022 .
Article PubMed Google Scholar
AlKhaldi M, Alkaiyat A, Abed Y, Pfeiffer C, Halaseh R, Salah R, et al. The Palestinian health research system: who orchestrates the system, how and based on what? A qualitatitve assessment. Health Res Policy Syst. 2018;16:69. https://doi.org/10.1186/s12961-018-0347-4 .
Ekeroma AJ, Biribo S, Herman J, Hill A, Kenealy T. Health research systems in six Pacific island countries and territories. J Res Dev. 2016;4:1. https://doi.org/10.4172/2311-3278.1000141 .
Article Google Scholar
Kirigia JM, Ota MO, Senkubuge F, Wiysonge CS, Mayosi BM. Developing the African national health research systems barometer. Health Res Policy Syst. 2016;14:53. https://doi.org/10.1186/s12961-016-0121-4 .
Ghannem H, Becerra-Posada F, IJsselmuiden C, Helwa I, de Haan S. National research for health system mapping in 5 countries in the Eastern Mediterranean Region and perspectives on strengthening the systems. East Mediterr Health J. 2011;17(3):260–1.
Shroff Z, Javadi D, Gilson L, Kang R, Ghaffar G. Institutional capacity to generate and use evidence in LMICs: current state and opportunities for HPSR. Health Res Policy Syst. 2017;15:94. https://doi.org/10.1186/s12961-017-0261-1 .
Health Sector Research Policy. Kigali: Rwanda Ministry of Health; 2012. http://moh.gov.rw/fileadmin/templates/policies/Health_Sector_Research_Policy.pdf . Accessed 1 Jan 2020.
Report of the International Conference on Health Research for Development, Bangkok, 10–13 October 2000. Geneva: International Organizing Committee; 2001. http://www.cohred.org/downloads/708.pdf . Accessed 1 Jan 2020.
World Health Organization. World report on knowledge for better health: strengthening health systems. Geneva: WHO; 2004. https://apps.who.int/iris/bitstream/handle/10665/43058/9241562811.pdf?sequence=1&isAllowed=y . Accessed 19 Dec 2019.
World Health Organization. National Health Research Systems: report of an international workshop. International Workshop on National Health Research Systems, Cha-am, Thailand, 12–15 March 2001. Geneva: WHO; 2002. https://apps.who.int/iris/bitstream/handle/10665/42455/a74582.pdf?sequence=1&isAllowed=y . Accessed 19 Dec 2019.
Action Plan to Strengthen the Use of Evidence, Information and Research for Policy-making in the WHO European Region. Regional Committee for Europe 66th session; EUR/RC66/12 + EUR/RC66/Conf.Doc./8. Copenhagen; WHO Regional Office for Europe; 2016. http://www.euro.who.int/__data/assets/pdf_file/0006/314727/66wd12e_EIPActionPlan_160528.pdf?ua=1 . Accessed 19 Dec 2019.
Edwards A, Zweigenthal V, Olivier J. Evidence map of knowledge translation strategies, outcomes, facilitators and barriers in African health systems. Health Res Policy Syst. 2019;17:16. https://doi.org/10.1186/s12961-019-0419-0 .
Murunga VI, Oronje RN, Bates I, et al. Review of published evidence on knowledge translation capacity, practice and support among researchers and research institutions in low- and middle-income countries. Health Res Policy Syst. 2020;18:16. https://doi.org/10.1186/s12961-019-0524-0 .
Chalmers I, Glasziou P. Avoidable waste in the production and reporting of research evidence. Lancet. 2009;374(9683):86–9. https://doi.org/10.1016/S0140-6736(09)60329-9 .
World Health Organization. Ministerial Summit on Health Research. Report by the Secretariat. In: Fifty-eighth World Health Assembly, Provisional Agenda Item 13.18 (A58/22). Geneva: WHO; 2005. http://apps.who.int/gb/archive/pdf_files/WHA58/A58_22-en.pdf . Accessed 17 Jan 2020.
Hanney S, Kuruvilla S, Soper B, Mays N. Who needs what from a national health research system: lessons from reforms to the English Department of Health's R&D system. Health Res Policy Syst. 2010;8:11. https://doi.org/10.1186/1478-4505-8-11 .
Davies S. Ten years of the NIHR: achievements and challenges for the next decade (23rd Annual Lecture, Royal College of Physicians). London: Office of Health Economics; 2017. https://www.ohe.org/sites/default/files/10%20years%20of%20NIHR%20V8.pdf . Accessed 1 Jan 2020.
Morgan Jones M, Kamenetzky A, Manville C, Ghiga I, MacLure C, Harte E, et al. The National Institute for Health at 10 years: an impact synthesis. Summary report. Santa Monica: RAND Corporation; 2016. http://www.rand.org/content/dam/rand/pubs/research_reports/RR1500/RR1574/RAND_RR1574.summary.pdf . Accessed 19 Dec 2019.
Rusakaniko S, Makanga M, Ota MO, Bockarie M, Banda G, Okeibunor J, et al. Strengthening national health research systems in the WHO African Region: progress towards universal health coverage. Glob Health. 2019;15:50. https://doi.org/10.1186/s12992-019-0492-8 .
Nabyonga-Orem J, Okeibunor J. Towards universal health coverage: can health research systems deliver contextualised evidence to guide progress in Africa? BMJ Glob Health. 2019;4:e001910. https://doi.org/10.1136/bmjgh-2019-001910 .
Becerra-Posada F, Minayo M, Quental C, de Haan S. National research for health systems in Latin America and the Caribbean: moving towards the right direction? Health Res Policy Syst. 2014;12:13. https://doi.org/10.1186/1478-4505-12-13 .
Ralaidovy AH, Adam T, Boucher P. Resource allocation for biomedical research: analysis of investments by major funders. Health Res Policy Syst. 2020;18:20. https://doi.org/10.1186/s12961-020-0532-0 .
Hanney S, Kanya L, Pokhrel S, Jones T, Boaz A. What is the evidence on policies, interventions and tools for establishing and/or strengthening national health research systems and their effectiveness? Health Evidence Network (HEN) synthesis report 69. Copenhagen: WHO Regional Office for Europe; 2020. https://apps.who.int/iris/bitstream/handle/10665/331703/9789289054942-eng.pdf .
Strengthening national health research systems: implementation of the action plan to strengthen the use of evidence, information and research for policy-making in the WHO European region. Report of the first multicountry meeting on research for health, Sofia, Bulgaria, 15–17 November 2017. Copenhagen: WHO Regional Office for Europe; 2018. http://www.euro.who.int/__data/assets/pdf_file/0009/367371/who-nhrs-meeting-report-eng.pdf?ua=1 . Accessed 19 Dec 2019.
Mansoori P. Evolution of Iran’s health research system over the past 50 years: a narrative review. J Glob Health. 2018;8(2):020703. https://doi.org/10.7189/jogh.08.020703 .
Atkinson P, Sheard S, Walley T. ‘All the stars were aligned’? The origins of England’s National Institute for Health Research. Health Res Policy Syst. 2019;17:95. https://doi.org/10.1186/s12961-019-0491-5 .
Department of Health. Best research for best health: a new national health research strategy. The NHS contribution to health research in England. London: Department of Health; 2006. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/568772/dh_4127152_v2.pdf . Accessed 1 May 2020.
Research, Evidence, Action. Health Research Board Strategy 2016–2020. Dublin: Health Research Board; 2015. https://www.hrb.ie/fileadmin/publications_files/HRB_Strategy_2016-2020.pdf . Accessed 1 Jan 2020.
An Act Institutionalizing the Philippine National Health Research System. Republic Act No. 10532. Manilla: Republic of the Philippines; 2013. https://www.officialgazette.gov.ph/2013/05/07/republic-act-no-10532/ . Accessed 19 Dec 2019.
Sombié I, Aidam J, Montorzi G. Evaluation of regional project to strengthen national health research systems in four countries in West Africa: lessons learned. Health Res Policy Syst. 2017;15(Suppl. 1):46. https://doi.org/10.1186/s12961-017-0214-8 .
Guimarães R, Santos LMP, Angulo-Tuesta A, Serruya SJ. Defining and implementing a national policy for science, technology, and innovation in health: lessons from the Brazilian experience. Cad Saude Publica. 2006;22(9):1775–85. https://doi.org/10.1590/s0102-311x2006000900002 .
Commission on Health Research for Development. Health research: essential link to equity and development. New York: Oxford University Press; 1990.
Inserm 2020 Strategic Plan. Paris: Institut National de la Santé et de la Recherche Médicale; 2015. https://www.inserm.fr/sites/default/files/2017-11/Inserm_PlanStrategique_2016-2020_EN.pdf . Accessed 19 Dec 2019.
Draft National Strategy for Health Research and Innovation. Il-Kalkara: Malta Council for Science and Technology; 2011. https://rio.jrc.ec.europa.eu/en/file/7363/download?token=2MYIdvgP . Accessed 19 Dec 2019.
Matthys B, Murugi J, de Haan S, Mausezahl D, Wyss K. Research for health and health system strengthening in Africa. Record paper 9. Geneva: Council on Health Research for Development; 2009. http://www.cohred.org/downloads/cohred_publications/COHREDRP9_Research%20_for_Health_System%20_Strengthening_in_Africa.pdf . Accessed 1 Jan 2020.
Santoro A, Glonti K, Bertollini R, Ricciardi W, McKee M. Mapping health research capacity in 17 countries of the former Soviet Union and south-eastern Europe: an exploratory study. Eur J Pub Health. 2016;26(2):349–54. https://doi.org/10.1093/eurpub/ckv186.
Senkubuge F, Mayosi BM. The state of the National Health Research system in South Africa. In: Padarath A, English R, editors. South African Health Review 2012/13. Durban: Health Systems Trust; 2013. p. 141–50.
Redman-Maclaren ML, Maclaren DJ, Solomon J, Muse A, Asugeni R, Harrington H, et al. Research workshop to research work: initial steps in establishing health research systems on Malaita, Solomon Islands. Health Res Policy Syst. 2010;8:33. https://doi.org/10.1186/1478-4505-8-33 .
Romero LI, Quental C. The Panamanian health research system: a baseline analysis for the construction of a new phase. Health Res Policy Syst. 2013;11:33. https://doi.org/10.1186/1478-4505-11-33 .
Chinnery F, Dunham KM, van der Linden B, Westmore M, Whitlock E. Ensuring value in health-related research. Lancet. 2018;391(10123):836–7. https://doi.org/10.1016/S0140-6736(18)30464-1 .
Ensuring Value in Research (EViR) Funders’ Collaboration and Development Forum. EViR Funders’ Forum; 2019. www.ensuringvalueinresearch.org . Accessed 19 Dec 2019.
Evidence-informed Policy Network (EVIPNet). Copenhagen: WHO Regional Office for Europe; 2020. http://www.euro.who.int/en/data-and-evidence/evidence-informed-policy-making/evidence-informed-policy-network-evipnet . Accessed 1 Jan 2020.
Hanney SR, González-Block MA. Building health research systems: WHO is generating global perspectives, and who's celebrating national successes? Health Res Policy Syst. 2016;14:90. https://doi.org/10.1186/s12961-016-0160-x .
Miller FA, Patton SJ, Dobrow M, Marshall DA, Berta W. Public involvement and health research system governance: a qualitative study. Health Res Policy Syst. 2018;16:87. https://doi.org/10.1186/s12961-018-0361-6 .
Montorzi G, de Haan S, IJsselmuiden C. Priority setting for research for health: a management process for countries. Geneva: Council on Health Research for Development; 2010. http://www.cohred.org/downloads/Priority_Setting_COHRED_approach_August_2010.pdf . Accessed 1 Jan 2020.
Marais D, Sombié I, Becerra-Posada F, Montorzi G, de Haan S. Governance, priorities and policies in national research for health systems in West Africa. Geneva: Council on Health Research for Development; 2011. https://www.healthresearchweb.org/files/West_Africa_Working_Paper_Final.pdf . Accessed 1 Jan 2020.
Sombié I, Aidam J, Konate B, Some TD, Kambou SS. The state of the research for health environment in the ministries of health of the Economic Community of the West African States (ECOWAS). Health Res Policy Syst. 2013;11:35. https://doi.org/10.1186/1478-4505-11-35 .
Directions for health research in BC. Vancouver: Michael Smith Foundation for Health Research; 2014. https://www.msfhr.org/sites/default/files/BC_health_research_strategy_FINAL.pdf . Accessed 19 Dec 2019.
New Zealand health research strategy 2017–2027. Wellington: Ministry of Business, Innovation and Employment/Ministry of Health; 2017. https://www.health.govt.nz/system/files/documents/publications/nz-health-research-strategy-jun17.pdf . Accessed 1 Jan 2020.
Chanda-Kapata P, Campbell S, Zarowsky C. Developing a national health research system: participatory approaches to legislative, institutional and networking dimensions in Zambia. Health Res Policy Syst. 2012;10:17. https://doi.org/10.1186/1478-4505-10-17 .
Miller FA, Patton SJ, Dobrow M, Berta W. Public involvement in health research systems: a governance framework. Health Res Policy Syst. 2018;16:79. https://doi.org/10.1186/s12961-018-0352-7 .
Viergever RF, Olifson S, Ghaffar A, Terry RF. A checklist for health research priority setting: nine common themes of good practice. Health Res Policy Syst. 2010;8:36. https://doi.org/10.1186/1478-4505-8-36 .
Nason E, Janta B, Hastings G, Hanney S, O'Driscoll M, Wooding S. Health research: making an impact. The economic and social benefits of HRB-funded research. Dublin: Health Research Board; 2008. https://www.hrb.ie/fileadmin/2._Plugin_related_files/Publications/2017_and_earlier_Pubs/Grant_Evaluation_Reports/Health_Research_-_Making_an_Impact.pdf . Accessed 19 Dec 2019.
Buxton M, Hanney S. How can payback from health services research be assessed? J Health Serv Res Policy. 1996;1(1):35–43.
Article CAS Google Scholar
Kristensen-Cabrera AI, Cuervo LG. Cross-sectional study on the utilization of the Pan American Health Organization/World Health Organization policy on research for health. Rev Panam Salud Publica. 2018;42:e77. https://doi.org/10.26633/RPSP.2018.77 .
Hanney SR, González-Block MA. ‘Knowledge for better health’ revisited: the increasing significance of health research systems – a review by departing Editors-in-Chief. Health Res Policy Syst. 2017;15:81. https://doi.org/10.1186/s12961-017-0248-y .
Bates I, Taegtmeyer M, Squire SB, Ansong D, Nhlema-Simwaka B, Baba A, et al. Indicators of sustainable capacity building for health research: analysis of four African case studies. Health Res Policy Syst. 2011;9:14. https://doi.org/10.1186/1478-4505-9-14 .
Lavis JN, Oxman AD, Lewin S, Fretheim A. SUPPORT tools for evidence-informed health policymaking (STP). Health Res Policy Syst. 2009;7(Suppl. 1):I1. https://doi.org/10.1186/1478-4505-7-S1-I1 .
Haynes A, Brennan S, Redman S, et al. Policymakers’ experience of a capacity-building intervention designed to increase their use of research: a realist process evaluation. Health Res Policy Syst. 2017;15:99. https://doi.org/10.1186/s12961-017-0234-4 .
Turner T, El-Jardali F. Building a bright, evidence-informed future: a conversation starter from the incoming editors. Health Res Policy Syst. 2017;15:88. https://doi.org/10.1186/s12961-017-0257-x .
Peters DH, Bhuiya A, Ghaffar A. Engaging stakeholders in implementation research: lessons from the Future Health Systems Research Programme experience. Health Res Policy Syst. 2017;15:104. https://doi.org/10.1186/s12961-017-0269-6 .
Adam P, Ovseiko PV, Grant J, et al. ISRIA statement: ten-point guidelines for an effective process of research impact assessment. Health Res Policy Syst. 2018;16:8. https://doi.org/10.1186/s12961-018-0281-5 .
Milat A, Lee K, Conte K, et al. Intervention Scalability Assessment Tool: a decision support tool for health policy makers and implementers. Health Res Policy Syst. 2020;18:1. https://doi.org/10.1186/s12961-019-0494-2 .
Scott AM, Kolstoe S, Ploem MC, et al. Exempting low-risk health and medical research from ethics reviews: comparing Australia, the United Kingdom, the United States and the Netherlands. Health Res Policy Syst. 2020;18:11. https://doi.org/10.1186/s12961-019-0520-4 .
Smits P, Champagne F. Governance of health research funding institutions: an integrated conceptual framework and actionable functions of governance. Health Res Policy Syst. 2020;18:22. https://doi.org/10.1186/s12961-020-0525-z .
Kalpazidou Schmidt E, Ovseiko PV, Henderson LR, et al. Understanding the Athena SWAN award scheme for gender equality as a complex social intervention in a complex system: analysis of Silver award action plans in a comparative European perspective. Health Res Policy Syst. 2020;18:19. https://doi.org/10.1186/s12961-020-0527-x .
Kamenetzky A, Hinrichs-Krapels S. How do organisations implement research impact assessment (RIA) principles and good practice? A narrative review and exploratory study of four international research funding and administrative organisations. Health Res Policy Syst. 2020;18:6. https://doi.org/10.1186/s12961-019-0515-1 .
Khalid AF, Lavis JN, El-Jardali F, et al. Supporting the use of research evidence in decision-making in crisis zones in low- and middle-income countries: a critical interpretive synthesis. Health Res Policy Syst. 2020;18:21. https://doi.org/10.1186/s12961-020-0530-2 .
Boland L, Kothari A, McCutcheon C, et al. Building an integrated knowledge translation (IKT) evidence base: colloquium proceedings and research direction. Health Res Policy Syst. 2020;18:8. https://doi.org/10.1186/s12961-019-0521-3 .
Article CAS PubMed PubMed Central Google Scholar
Conte KP, Davidson S. Using a ‘rich picture’ to facilitate systems thinking in research coproduction. Health Res Policy Syst. 2020;18:14. https://doi.org/10.1186/s12961-019-0514-2 .
Jessani NS, Valmeekanathan A, Babcock C, et al. Exploring the evolution of engagement between academic public health researchers and decision-makers: from initiation to dissolution. Health Res Policy Syst. 2020;18:15. https://doi.org/10.1186/s12961-019-0516-0 .
Slattery P, Saeri AK, Bragge P. Research co-design in health: a rapid overview of reviews. Health Res Policy Syst. 2020;18:17. https://doi.org/10.1186/s12961-020-0528-9 .
Zych MM, Berta WB, Gagliardi AR. Conceptualising the initiation of researcher and research user partnerships: a meta-narrative review. Health Res Policy Syst. 2020;18:24. https://doi.org/10.1186/s12961-020-0536-9 .
Cash-Gibson L, Harris M, Guerra G, et al. A novel conceptual model and heuristic tool to strengthen understanding and capacities for health inequalities research. Health Res Policy Syst. 2020;18:42. https://doi.org/10.1186/s12961-020-00559-z .
Mansoori P, Majdzadeh R, Abdi Z, Rudan I, Chan KY, The Iranian CHNRI Health Research Priority Setting Group, et al. Setting research priorities to achieve long-term health targets in Iran. J Glob Health. 2018;8(2):020702. https://doi.org/10.7189/jogh.08.020702 .
Palmer A, Anya SE, Bloch P. The political undertones of building national health research systems: reflections from the Gambia. Health Res Policy Syst. 2009;7:13. https://doi.org/10.1186/1478-4505-7-13 .
Shergold M, Grant J. Freedom and need: the evolution of public strategy for biomedical and health research in England. Health Res Policy Syst. 2008;6:2. https://doi.org/10.1186/1478-4505-6-2 .
Kok MO, Gyapong JO, Wolffers I, Ofori-Adjei D, Ruitenberg EJ. Towards fair and effective north–south collaboration: realizing a programme for demand-driven and locally led research. Health Res Policy Syst. 2017;15:96. https://doi.org/10.1186/s12961-017-0251-3 .
Editorial. Bringing health research forward. Tanzan J Health Res. 2009;11(4):iii–iv.
Oliver K, Kothari A, Mays N. The dark side of coproduction: do the costs outweigh the benefits for health research? Health Res Policy Syst. 2019;17:33. https://doi.org/10.1186/s12961-019-0432-3 .
Ahmedov M, de Haan S, Sarymsakova B. Strengthening health research systems in Central Asia: a system mapping and consultative process. Working paper 2. Geneva: Council on Health Research for Development; 2007. http://www.cohred.org/downloads/cohred_publications/wp2_CentralAsia.pdf . Accessed 1 Jan 2020.
Hanney SR, Wooding S, Sussex J, et al. From COVID-19 research to vaccine application: why might it take 17 months not 17 years and what are the wider lessons?. Health Res Policy Syst. 2020;18:61. https://doi.org/10.1186/s12961-020-00571-3 .
WHO Western Pacific: Philippines. PH solidarity trial for COVID-19 treatments receives green light from ethics review body. Press release. WHO. 22 April 2020. https://www.who.int/philippines/news/detail/22-04-2020-ph-solidarity-trial-for-covid-19-treatments-receives-green-light-from-ethics-review-body . Accessed 15 May 2020.
Lane R. Sarah Gilbert: carving a path towards a COVID-19 vaccine. Lancet. 2020;395:1247. https://doi.org/10.1016/S0140-6736(20)30796-0 .
Download references
Acknowledgements
We thank colleagues at WHO’s Regional Office for Europe for the inputs to the original Health Evidence Network Evidence Synthesis. The authors are responsible for the content of this Opinion piece.
The WHO’s Regional Office for Europe funded the Health Evidence Network Evidence Synthesis. The additional literature searching and analysis for this Opinion piece, along with its drafting, was unfunded. Annette Boaz, Kingston University and St George’s University of London, is supported by the National Institute for Health Research (NIHR) Applied Research Collaboration South London (NIHR ARC South London) at King’s College Hospital NHS Foundation Trust. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Author information
Authors and affiliations.
Health Economics Research Group, Institute of Health, Environment and Societies, Brunel University London, Uxbridge, UB8 3PH, United Kingdom
Stephen R. Hanney, Lucy Kanya, Subhash Pokhrel & Teresa H. Jones
Department of Health Policy, London School of Economics and Political Science, London, United Kingdom
Faculty of Health, Social Care and Education, a partnership between Kingston University and St George’s, University of London, London, United Kingdom
Annette Boaz
You can also search for this author in PubMed Google Scholar
Contributions
SP, LK and SH planned the original phase of the WHO evidence synthesis, including the search strategy. LK led the original literature search and contributed article selection and data extraction and analysis. AB and SH planned the second phase of the evidence synthesis. TJ led the second phase of the literature search and contributed to the article selection and data extraction. AB contributed to the final version of the Health Evidence Network report. SH led the data extraction and analysis and drafting of the report. SH conducted the additional analysis of the literature and initial drafting for this Opinion piece. All authors commented on the Opinion piece and approved the final version.
Corresponding author
Correspondence to Stephen R. Hanney .
Ethics declarations
Ethics approval and consent to participate.
Not applicable.
Consent for publication
The full version of the evidence synthesis was published by WHO’s Regional Office for Europe, and all the data used for the report and this Opinion piece are publicly available.
Competing interests
The authors have no competing interests to declare. AB is a member of the World Health Organization European Advisory Committee on Health Research. SH was co-editor of Health Research Policy and Systems from 2006 to 2017.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Hanney, S.R., Kanya, L., Pokhrel, S. et al. How to strengthen a health research system: WHO’s review, whose literature and who is providing leadership?. Health Res Policy Sys 18 , 72 (2020). https://doi.org/10.1186/s12961-020-00581-1
Download citation
Received : 13 March 2020
Accepted : 21 May 2020
Published : 23 June 2020
DOI : https://doi.org/10.1186/s12961-020-00581-1
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Biomedical research
- Capacity-building
- Evidence-based practice
- Health ministries
- Health research systems
- Health services research
- Policy-making
- Priority-setting
- Research utilisation
- Translational medical research
ISSN: 1478-4505
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]
- Career Center
- Member Login
Report Identifies Directions for the Field of Public Health Services and Systems Research
Domains and research questions to guide public health services and systems research (PHSSR) were generated through a one-year multi-stage, participatory process.

A Research Agenda for an Evolving Public Health System: Directions for the Field of Public Health Services and Systems Research
An effective, high-performing public health system requires current, relevant, and reliable research to inform public health practice strategies. The need for funding and support to strengthen the evidence-base to guide and evaluate system improvements remains imperative, creating inspiration for an updated research agenda for the field of public health services and systems research (PHSSR).
AcademyHealth in collaboration with the American Public Health Association (APHA), with funding from Kaiser Permanente, developed a renewed research agenda for the evidence needed to inform and improve public health programs, systems, and services in the next decade. Based on the input of leading experts from health care systems, academia, philanthropy, government agencies, and community-based organizations, the report outlines PHSSR priorities in the following seven domains:
- Health Equity
- Cross-Sector Partnerships and Engagement
- Data and Information Technology
- Financing and Resources
- Law and Governance
- Communication and Narrative
Each domain features 10-13 prioritized research questions, generated through an online prioritization activity. Questions were further informed by an advisory group alongside listening sessions held with federal agencies and the AcademyHealth PHSSR Interest Group. The prioritized questions underscore measuring and achieving progress for health equity; barriers to data modernization; and issues related to enumerating, hiring, and retaining the public health workforce.
The renewed agenda acknowledges that it will face barriers that previous agendas also faced in seeking funding, however, opportunities for adoption are outlined such as the Public Health Infrastructure Saves Lives Act and the public health workforce loan repayment program. Advocacy remains a priority for a sustainable public health infrastructure, including sustainable funding to support this research agenda.
This paper is in the following e-collection/theme issue:
Published on 8.4.2024 in Vol 26 (2024)
Longitudinal Monitoring of Clinician-Patient Video Visits During the Peak of the COVID-19 Pandemic: Adoption and Sustained Challenges in an Integrated Health Care Delivery System
Authors of this article:
Original Paper
- Jessica A Palakshappa 1, 2 , MD, MS ;
- Erica R Hale 1, 2 , MS ;
- Joshua D Brown 1 , PhD ;
- Carol A Kittel 2 , MA ;
- Emily Dressler 2 , PhD ;
- Gary E Rosenthal 1, 2 , MD ;
- Sarah L Cutrona 3, 4 , MD, MPH ;
- Kristie L Foley 2 , MS, PhD ;
- Emily R Haines 2 , PhD ;
- Thomas K Houston II 1, 2 , MD, MPH
1 Atrium Health Wake Forest Baptist, Winston Salem, NC, United States
2 Wake Forest University School of Medicine, Winston Salem, NC, United States
3 Department of Population and Quantitative Health Sciences, University of Massachusetts Chan Medical School, Worcester, MA, United States
4 Center for Healthcare Organization and Implementation Research, Veterans Affairs Bedford Healthcare System, Bedford, MA, United States
Corresponding Author:
Jessica A Palakshappa, MD, MS
Wake Forest University School of Medicine
1 Medical Center Blvd
Winston Salem, NC, 27157
United States
Phone: 1 336 716 8465
Email: [email protected]
Background: Numerous prior opinion papers, administrative electronic health record data studies, and cross-sectional surveys of telehealth during the pandemic have been published, but none have combined assessments of video visit success monitoring with longitudinal assessments of perceived challenges to the rapid adoption of video visits during the pandemic.
Objective: This study aims to quantify (1) the use of video visits (compared with in-person and telephone visits) over time during the pandemic, (2) video visit successful connection rates, and (3) changes in perceived video visit challenges.
Methods: A web-based survey was developed for the dual purpose of monitoring and improving video visit implementation in our health care system during the COVID-19 pandemic. The survey included questions regarding rates of in-person, telephone, and video visits for clinician-patient encounters; the rate of successful connection for video visits; and perceived challenges to video visits (eg, software, hardware, bandwidth, and technology literacy). The survey was distributed via email to physicians, advanced practice professionals, and clinicians in May 2020. The survey was repeated in March 2021. Differences between the 2020 and 2021 responses were adjusted for within-respondent correlation across surveys and tested using generalized estimating equations.
Results: A total of 1126 surveys were completed (511 surveys in 2020 and 615 surveys in 2021). In 2020, only 21.7% (73/336) of clinicians reported no difficulty connecting with patients during video visits and 28.6% (93/325) of clinicians reported no difficulty in 2021. The distribution of the percentage of successfully connected video visits (“Over the past two weeks of scheduled visits, what percentage did you successfully connect with patients by video?”) was not significantly different between 2020 and 2021 ( P =.74). Challenges in conducting video visits persisted over time. Poor connectivity was the most common challenge reported by clinicians. This response increased over time, with 30.5% (156/511) selecting it as a challenge in 2020 and 37.1% (228/615) in 2021 ( P =.01). Patients not having access to their electronic health record portals was also a commonly reported challenge (109/511, 21.3% in 2020 and 137/615, 22.3% in 2021, P =.73).
Conclusions: During the pandemic, our health care delivery system rapidly adopted synchronous patient-clinician communication using video visits. As experience with video visits increased, the reported failure rate did not significantly decline, and clinicians continued to report challenges related to general network connectivity and patient access to technology.
Introduction
Interest in telehealth from policy makers, health care providers, patients, and families continues to grow [ 1 ], including newer modalities such as video visits [ 2 ]. Video visits refer to clinician-patient communication that includes real time video and audio assessment of the patient when the clinician is in a different location. Video visits have the potential to improve efficiency for clinicians and to improve access for patients, particularly those who reside in rural areas or with transportation barriers [ 3 ]. The technology to support video visits has existed for decades; however, only a small minority of clinicians used this form of telehealth in their practices [ 4 ] prior to the COVID-19 pandemic. There are multiple reasons why telehealth adoption was slow despite its potential benefits including changing cost and reimbursement policies, federal and state licensing laws, incompatible electronic health records, and gaps in internet access in certain areas.
The COVID-19 pandemic and subsequent public health emergency led to fundamental shifts in how health care was delivered in the United States, including the rapid adoption of telehealth services. Before the public health emergency, approximately 13,000 fee-for-service Medicare beneficiaries received telehealth services in a week and that number increased to nearly 1.7 million beneficiaries by the last week of April 2020 [ 5 ]. While the need to avoid in-person contact fueled the initial rapid rise, regulations and restrictions were temporarily lifted during this time facilitating its use. Clinicians were also paid for telehealth services at the same rate as in-person medical services. Several studies have reported on the rapid uptake of telehealth, including video visits, in this context [ 6 - 8 ]. However, few reports have explored rates of success and failure of video visits over time. The challenges clinicians face in conducting video visits have also not been explored. Understanding these challenges will be important for improving and expanding the reach of telehealth services after the pandemic has ended.
In the context of the rapidly increasing use of telehealth to conduct video visits, and consistent with the sociotechnical model’s [ 9 ] emphasis on monitoring the implementation of health information technology in complex adaptive health care systems, our health care delivery system initiated a series of brief assessments of video visit adoption. The research objective of this report is to summarize the findings of the video visit monitoring including (1) the use of video visits (compared with in-person and telephone visits) over time during the pandemic, (2) video visit successful connection rates, and (3) changes in perceived video visit challenges. With patient and clinician skills and experience with video visits increasing over time, our primary hypothesis was that clinicians’ perceived challenges to completing video visits (eg, software, hardware, bandwidth, and technology literacy) would decline over time.
Study Design
The design was a longitudinal series of 2 cross-sectional assessments (2020 and 2021). In summary, for the dual purpose of monitoring and improving telehealth implementation in our health care delivery system, institutional leaders developed a brief web-based survey regarding the use of video visits and challenges. The survey was initially distributed in 2020. Given the ongoing public health emergency and the need to re-evaluate telehealth use, the survey was repeated in 2021. Institutional leaders encouraged clinicians to complete the survey, communicating encouragement via emails and announcements at in-person faculty and departmental meetings.
Ethical Considerations
As the brief assessments were distributed by the clinical system as part of ongoing quality improvement, the project was approved as an research protocol as exempt from human participants approval by the Wake Forest University School of Medicine Institutional Review Board (IRB00077473). The survey did not collect identifying information from the participants.
Survey Development
Published in 2010 by Sittig and Singh [ 9 ], the sociotechnical model of health information technology was the first to fully emphasize the importance of system monitoring in implementation frameworks. Key aspects of monitoring, including measuring how the technology is being used by clinicians and whether implementation outcomes are being achieved, were considered when developing the survey. The survey was developed with a literature search, expert review, and iterative pilot-testing (see Multimedia Appendix 1 ). The final survey included 12 questions related to rates of in-person, telephone, and video for clinician-patient encounters; the rate of successful connection for video visits; and perceived challenges to video visits (eg, software, hardware, bandwidth, and technology literacy).
Study Population
The study population included all outpatient clinicians practicing across the health care delivery system; we excluded clinicians without direct patient care responsibilities. The system includes 5 hospitals and over 350 primary care and specialty clinics that provide care to over 2 million persons annually. The brief assessment was distributed to clinicians in 2020 and 2021 (1937 clinicians and 2843 clinicians, respectively).
Survey Distribution and Data Collection
As we are an integrated health care delivery system, we had access to the contact details of all providers. Our group practice clinical operations executive committee facilitated the survey distribution by requesting that each department chair and clinical service line director send an email to their team of providers to notify them of the survey and encourage completion. Surveys were collected and managed using REDCap (Research Electronic Data Capture), a secure, web-based app designed to support data capture [ 10 , 11 ]. A unique survey link was distributed via email to each clinician in May 2020 and March 2021. The system sent up to 2 reminder emails if the recipient had not yet completed the survey.
Statistical Analysis
To take full advantage of the data collected, we first analyzed the results as 2 cross-sectional surveys. In this primary analysis, we included all respondents in each year. We recognize that a subset of clinicians also responded in both years. Thus, as a secondary analysis, we analyzed the data limited to the longitudinal cohort who participated in both years. First, summary statistics are presented as count (frequency) for categorical variables and mean (SD) or median (IQR) for continuous variables as appropriate. Generalized estimating equations were then used to model frequency distributions of in-person, telephone, and video visits, and patient and clinician challenges. These logit models were adjusted for within-respondent correlation across surveys via an exchangeable correlation structure. P values of .05 were considered statistically significant. P values for multiple comparisons in frequency distributions of in-person, telephone, and video visits between physicians, advanced practice professionals (APPs), and other clinicians were adjusted via the Tukey-Kramer method to control for type I errors with a corrected P value <.05 deemed statistically significant [ 12 ]. All statistical analyses were performed with R (version 4.2.1; R Core Team) [ 13 ].
We recognize that a subset of clinicians responded in both years. Thus, as a secondary analysis, we analyzed the data limited to the longitudinal cohort who participated in both surveys. For the secondary analysis, matched pairs analyses were performed as were performed in the entire sample with only those responses from clinicians that completed both surveys.
Surveillance Participation and Participant Characteristics
In 2020, 1937 surveys were sent and 511 responses were received (response rate 26.4%). In 2021, 2843 surveys were sent and 615 responses were received (response rate 21.6%). In both years, over 55% of the respondents were physicians from a wide range of clinical specialties. About half of the clinicians who completed the survey in 2020 also completed it in 2021 ( Table 1 ).
a n=511 responses in 2020 and n=615 responses in 2021.
b n=300 responses in 2020 and n=353 responses in 2021.
Health Care Delivery by In-Person and Telephone
To place the volume of telehealth in context, we first asked about the number of in-person encounters completed over the past 2 weeks ( Table 2 ). The distribution of responses differed between 2020 and 2021 ( P <.001). Modeled probabilities show fewer respondents reported zero (22.2% vs 4.9%) or 1 to 10 (33.5% vs 11.5%) in-person visits in 2021 as compared with 2020. The volume of in-person visits increased over time ( Table 2 ). Further, the majority of respondents (399/509, 78.4%) reported at least 1 telephone visit in 2020 and 65.7% (369/562) in 2021 although the distribution of responses differed from 2020 to 2021 ( P <.001).
a Differences in frequency distributions between 2020 and 2021 tested via generalized estimating equation modeling; P value adjusted using Tukey-Kramer method to control for type I errors.
Health Care Delivery by Video Visits
Many health care providers were engaged in virtual care, with 65.9% (336/510) health care providers reporting video visit encounters in 2020 and 57.6% (325/564) health care providers reporting video visit encounters in 2021 ( Table 2 ) although the distribution of responses again changed from 2020 to 2021 ( P <.001). Compared with 2020, fewer 2021 respondents reported 11-25 (18.6% vs 6.7%), 26-50 (5.9% vs 2.8%), or over 50 (2.4% vs 2%) visits.
Secondary analyses were robust to missing data and showed that the results (distributions of in-person, phone, and video visits) did not change when limiting the data to only respondents who participated in both surveys.
Comparing Health Care Delivery by Physicians, APPs, and Others
We also compared health care delivery modality by type of clinician (physicians, APPs, or others). Patterns of health care delivery reported in the overall sample were similar in the physician, APP, and other subgroups. There were no significant differences between physicians and APPs in the number of patient encounters that were completed as in-person, telephone visits, or video visits in 2020 or 2021.
Perceived Challenges to Patient-Clinician Connection Using Video Visits
The use of video visits came with challenges. In 2020, only 21.7% (73/336) of clinicians reported no difficulty connecting with patients during video visits and 28.6% (93/325) of clinicians reported no difficulty in 2021 ( Figure 1 ). The distribution of the percentage of successfully connected video visits (“Over the past two weeks of scheduled visits, what percentage did you successfully connect with patients by video?”) was not significantly different between 2020 and 2021 ( P =.74, Figure 1 ). There was also no significant difference between physicians and APPs in the rate of successful video connection with patients in either year.

Clinicians were asked about the challenges in successfully completing video visits (see Table 3 ). The most commonly reported challenge was poor connectivity. This response increased over time with 30.5% (156/511) selecting it as a challenge in 2020 and 37.1% (228/615) selecting it as a challenge in 2021 ( P =.01). Patients not having access to their electronic health record portals was also a commonly reported challenge (109/511, 21.3% in 2020 and 137/615, 22.3% in 2021; P =.73).
a P value adjusted using the Tukey-Kramer method to control for type I errors.
b For some clinical video visits, a prerequisite was that patients needed to have registered with the patient portal.
Principal Findings
Although telehealth technology was available in our health care delivery system prior to the COVID-19 pandemic, it saw only limited use for providing synchronous care to patients prior to the pandemic. Inconsistent reimbursement for services, restrictions on the physical location of patients and clinicians during telehealth, and rules about types of visits that were acceptable for telehealth services all contributed to its limited use [ 14 , 15 ]. With the pandemic, and consistent with other reports, our health care delivery system rapidly expanded the provision of clinical care by way of video visits. Later in the pandemic, in-person visits did increase, but the use of video visits remained well above prepandemic levels.
Overall, there has been a shift toward a more positive sentiment about telehealth and telemedicine since the start of the pandemic. A scoping review by Doraiswamy et al [ 16 ] reported 543 telehealth-related papers (mostly opinions, commentaries, and perspectives; 61%) published across 331 different journals from January to June 2020. Most of these new reports had a “celebratory” or favorable sentiment about the use of telehealth. The scope of the increase in telehealth during the public health emergency likely contributed to this sentiment though concerns about patient and clinician connection, the lack of physical examinations, and cost-effectiveness were still noted by some. Although our providers reported benefits for clinical video telehealth beyond audio-only calls for patient-provider visits, failure to connect using clinical video visits was common.
While reports have documented challenges with clinical video telehealth [ 17 ], few have monitored these challenges over time. During the pandemic, as our health care delivery system’s experience with video visits grew, clinicians did not report a meaningful reduction in connection failure rate. The most frequently reported challenges were general network connectivity and those related to the digital divide (eg, patient lack of internet access, needed software, or internet-connected cameras). Gaps in access to technology and the internet for telehealth may impact some patient groups more than others. For example, older age, rural residence, dual Medicare and Medicaid enrollment, and non-Hispanic Black or Hispanic race or ethnicity have been shown to be associated with a lower probability of technology ownership, access to the internet, and use of the internet for communication in cancer survivors [ 18 ]. Further, over 10% of clinicians also reported that they experienced software or hardware challenges (eg, limited availability of internet cameras at a clinical location). Expanding telehealth will require ongoing investments in technology for clinicians. New workflows to support successful connection during video visits and follow-up processes may also be needed.
Our video visit monitoring results were shared with clinical operations leadership. In response to the sustained challenges noted, we initiated a new video visit program to provide patient support prior to scheduled video visits. Our technology navigators are a specially trained, centralized team and are directed to reach out to vulnerable patients and families to facilitate video visit access. A new electronic health record dashboard identified patients with (1) a scheduled video visit and (2) 1 or more risk factors (eg, lack of a prior successful video visit and lack of patient portal access). We further prioritized patients older than 65 years and those living in rural areas. Technology navigators reached out by telephone to contact these at-risk patients to assess their technology access (eg, internet, software, webcam, or smartphone), technology literacy and perceived competence, and availability of at-home support from family and friends. The technology navigators then troubleshoot any challenges noted by the patients and offer to conduct a “practice” video visit. Evaluation of this program is ongoing. In 2022-2023, the navigators contacted 1266 patients at high risk for video visit failure. Among those contacted, 515 requested and were provided assistance. With previsit support from the navigators, the patient-provider scheduled video visit completion rate was 84% as compared with a 60% completion rate among those patients who did not receive support.
Limitations of our video visit surveillance analysis include that the data were collected across 1 health care delivery system with an integrated electronic health care record system. The perceptions and challenges may be different in a smaller health care system and in those with different health care record systems. The survey measured only clinician-reported telehealth use and success rates which may be limited by recall. As with all surveys, our results may be biased as only about one-quarter of the sample responded. It is possible that respondents experienced more challenges conducting video visits than those who did not respond. Further, not all clinicians longitudinally completed both the 2020 and 2021 surveys—due both to response rates and providers leaving and entering the health care system. Thus, changes over time may represent differences in the underlying sample. For example, new clinicians may have been more or less familiar with conducting video visits.
Conclusions
Recent reviews have noted the need for more evidence related to telehealth’s implementation, effectiveness, and health equity in telehealth access [ 16 , 19 , 20 ]. Although internet and smartphone access has increased over the last decade (with older adults being one of the fastest-growing subgroups of new adoption), our longitudinal video visit surveillance reveals that the digital divide is still a significant barrier to video visit access.
Although Healthy People 2030 (a set of national objectives to improve health and well-being) includes developmental and research objectives related to patient portals and increasing the use of telehealth to improve access to health services [ 21 ], some social determinants of health taxonomies do not include technology access. If telehealth is increasingly an important component of health care access, then technology access (eg, internet, smartphone, patient portal, and connected hardware, such as internet-connected video) should be considered a social determinant of health [ 22 ]. A comprehensive solution to overcoming the digital divide has not yet been achieved. However, some partial solutions include directly providing technology to patients, providing detailed instructions, and support services (eg, our technology navigator program), and engaging trusted caregivers (family and friends) who may be able to assist patients [ 23 - 27 ].
Acknowledgments
The project was supported through the National Cancer Institute Cancer Moonshot initiative—iDAPT: Implementation and Informatics–Developing Adaptable Processes and Technologies for Cancer Control (P50 CA244693); the Wake Forest Clinical and Translational Science Award (5UL1TR001420); and also a career development award to JAP (1K23AG073529).
Conflicts of Interest
None declared.
Brief Provider Telehealth Assessment.
- World Health Organization. Telemedicine: Opportunities and Developments in Member States: Report on the Second Global Survey on eHealth 2009. Geneva, Switzerland. World Health Organization; 2010.
- Moulaei K, Shanbehzadeh M, Bahaadinbeigy K, Kazemi-Arpanahi H. Survey of the patients' perspectives and preferences in adopting telepharmacy versus in-person visits to the pharmacy: a feasibility study during the COVID-19 pandemic. BMC Med Inform Decis Mak. 2022;22(1):99. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Nesbitt TS. The evolution of telehealth: where have we been and where are we going? In: Lustig TA, editor. The Role of Telehealth in an Evolving Health Care Environment: Workshop Summary. Washington, DC. National Academies Press; 2012;11-16.
- Kane CK, Gillis K. The use of telemedicine by physicians: still the exception rather than the rule. Health Aff (Millwood). 2018;37(12):1923-1930. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Kane CK, Gillis K. The use of telemedicine by physicians: still the exception rather than the rule. Health Aff (Millwood). Dec 2018;37(12):1923-1930. [ CrossRef ] [ Medline ]
- Weiner JP, Bandeian S, Hatef E, Lans D, Liu A, Lemke KW. In-person and telehealth ambulatory contacts and costs in a large US insured cohort before and during the COVID-19 pandemic. JAMA Netw Open. 2021;4(3):e212618. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Gilson SF, Umscheid CA, Laiteerapong N, Ossey G, Nunes KJ, Shah SD. Growth of ambulatory virtual visits and differential use by patient sociodemographics at one urban academic medical center during the COVID-19 pandemic: retrospective analysis. JMIR Med Inform. 2020;8(12):e24544. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Hatef E, Wilson RF, Hannum SM, Zhang A, Kharrazi H, Weiner JP, et al. Use of Telehealth During the COVID-19 Era. Rockville, MD. Agency for Healthcare Research and Quality; 2023.
- Sittig DF, Singh H. A new sociotechnical model for studying health information technology in complex adaptive healthcare systems. Qual Saf Health Care. 2010;19(Suppl 3):i68-i74. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap): a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O'Neal L, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Midway S, Robertson M, Flinn S, Kaller M. Comparing multiple comparisons: practical guidance for choosing the best multiple comparisons test. PeerJ. 2020;8:e10387. [ FREE Full text ] [ CrossRef ] [ Medline ]
- R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria. R Foundation for Statistical Computing; 2023.
- Shaver J. The state of telehealth before and after the COVID-19 pandemic. Prim Care. 2022;49(4):517-530. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Hyder MA, Razzak J. Telemedicine in the United States: an introduction for students and residents. J Med Internet Res. 2020;22(11):e20839. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Doraiswamy S, Abraham A, Mamtani R, Cheema S. Use of telehealth during the COVID-19 pandemic: scoping review. J Med Internet Res. 2020;22(12):e24087. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Garfan S, Alamoodi AH, Zaidan BB, Al-Zobbi M, Hamid RA, Alwan JK, et al. Telehealth utilization during the Covid-19 pandemic: a systematic review. Comput Biol Med. 2021;138:104878. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Lama Y, Davidoff AJ, Vanderpool RC, Jensen RE. Telehealth availability and use of related technologies among medicare-enrolled cancer survivors: cross-sectional findings from the onset of the COVID-19 pandemic. J Med Internet Res. 2022;24(1):e34616. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Moulaei K, Moulaei R, Bahaadinbeigy K. Barriers and facilitators of using health information technologies by women: a scoping review. BMC Med Inform Decis Mak. 2023;23(1):176. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Rodriguez JA, Shachar C, Bates DW. Digital inclusion as health care: supporting health care equity with digital-infrastructure initiatives. N Engl J Med. 2022;386(12):1101-1103. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Healthy people 2030: health IT. U.S. Department of Health and Human Services. URL: https://health.gov/healthypeople/objectives-and-data/browse-objectives/health-it [accessed 2024-03-14]
- Benda NC, Veinot TC, Sieck CJ, Ancker JS. Broadband internet access is a social determinant of health!. Am J Public Health. 2020;110(8):1123-1125. [ CrossRef ] [ Medline ]
- Francis J, Kadylak T, Makki TW, Rikard RV, Cotten SR. Catalyst to connection: when technical difficulties lead to social support for older adults. Am Behav Sci. 2018;62(9):1167-1185. [ CrossRef ]
- Cotten SR, Yost EA, Berkowsky RW, Winstead V, Anderson WA. Designing Technology Training for Older Adults in Continuing Care Retirement Communities, 1st Edition. Boca Raton, FL. CRC Press; 2016.
- Sadasivam RS, Kinney RL, Lemon SC, Shimada SL, Allison JJ, Houston TK. Internet health information seeking is a team sport: analysis of the Pew internet survey. Int J Med Inform. 2013;82(3):193-200. [ CrossRef ] [ Medline ]
- Luger TM, Hogan TP, Richardson LM, Cioffari-Bailiff L, Harvey K, Houston TK. Older veteran digital disparities: examining the potential for solutions within social networks. J Med Internet Res. 2016;18(11):e296. [ FREE Full text ] [ CrossRef ] [ Medline ]
- Houston TK, Richardson LM, Cotten SR. Patient-directed digital health technologies: is implementation outpacing evidence? Med Care. 2019;57(2):95-97. [ CrossRef ] [ Medline ]
Abbreviations
Edited by G Eysenbach, T Leung; submitted 26.10.23; peer-reviewed by K Moulaei; comments to author 19.12.23; revised version received 24.01.24; accepted 09.03.24; published 08.04.24.
©Jessica A Palakshappa, Erica R Hale, Joshua D Brown, Carol A Kittel, Emily Dressler, Gary E Rosenthal, Sarah L Cutrona, Kristie L Foley, Emily R Haines, Thomas K Houston II. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 08.04.2024.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in the Journal of Medical Internet Research, is properly cited. The complete bibliographic information, a link to the original publication on https://www.jmir.org/, as well as this copyright and license information must be included.
- Alzheimer's disease & dementia
- Arthritis & Rheumatism
- Attention deficit disorders
- Autism spectrum disorders
- Biomedical technology
- Diseases, Conditions, Syndromes
- Endocrinology & Metabolism
- Gastroenterology
- Gerontology & Geriatrics
- Health informatics
- Inflammatory disorders
- Medical economics
- Medical research
- Medications
- Neuroscience
- Obstetrics & gynaecology
- Oncology & Cancer
- Ophthalmology
- Overweight & Obesity
- Parkinson's & Movement disorders
- Psychology & Psychiatry
- Radiology & Imaging
- Sleep disorders
- Sports medicine & Kinesiology
- Vaccination
- Breast cancer
- Cardiovascular disease
- Chronic obstructive pulmonary disease
- Colon cancer
- Coronary artery disease
- Heart attack
- Heart disease
- High blood pressure
- Kidney disease
- Lung cancer
- Multiple sclerosis
- Myocardial infarction
- Ovarian cancer
- Post traumatic stress disorder
- Rheumatoid arthritis
- Schizophrenia
- Skin cancer
- Type 2 diabetes
- Full List »
share this!
April 10, 2024
This article has been reviewed according to Science X's editorial process and policies . Editors have highlighted the following attributes while ensuring the content's credibility:
fact-checked
peer-reviewed publication
trusted source
Experiencing racial discrimination impacts the mental health of teens in the U.S. justice system
by Southern Methodist University

A new study by Southern Methodist University psychologists and a researchers from the University of Washington shows that interpersonal racial discrimination and other forms of violence can impact the mental health of adolescents in the justice system.
The research advocates for a more holistic approach to mental health intervention, emphasizing the importance of considering adolescents' experiences of interpersonal racial discrimination alongside other more recognized forms of violence. By acknowledging and addressing these intersecting factors, stakeholders can better tailor support systems to meet the unique needs of adolescents of color in the justice system.
Published in the Journal of Interpersonal Violence , the study involves 118 adolescents of color, ages 14 to 17, and their mothers, comparing the effects of interpersonal racial discrimination together with experiences of harsh parenting, teen dating violence, and exposure to parental partner violence. The authors note that while interpersonal racial discrimination can be conceptualized as a type of interpersonal violence, it is seldom considered as such.
This can be a problem when trying to understand how a teen's exposure to interpersonal violence, in various forms, relates to their mental health symptoms and subsequent acts of delinquency. The authors note that adolescents of color are disproportionately represented in the U.S. justice system, a disparity that previous studies have tied to racism and interpersonal racial discrimination.
"It is common for researchers to look at common adverse childhood experiences related to violence, but often racial discrimination is left out of the equation," said lead author Ernest Jouriles, professor and director of clinical training in SMU's Department of Psychology. "We found that experiencing interpersonal racial discrimination is as harmful, if not more harmful, than other commonly studied traumatic events."
The research used 3-month longitudinal data from a larger study that looked at how mother-adolescent communication about dating relationships is linked to adolescent dating violence and victimization. Participants in that study were recruited with flyers distributed at truancy courts, by probation offices, and through victim services offices.
Half of the teenagers reported experiencing violence from their parents, and more than half said they had experienced violence in their dating relationships. Some also reported they had seen their parents being physically violent with each other. About half noted they themselves had been mistreated because of their race. Many believed the unfair treatment stemmed from people perceiving the teens as lacking intelligence.
"Historically, this research has been very siloed, with racial discrimination in one area of research and interpersonal violence in another, but our results suggest they should be examined together," said Melissa Sitton, a doctoral student in the SMU Clinical Psychology program and one of the paper's authors. "Researchers, clinicians and others providing services must assess situations more broadly to provide more effective assistance."
Sitton will present the research at the upcoming Society for Research in Child Development Anti-Racist Developmental Science Summit: Transforming Research, Practices, and Policies Summit , scheduled for May 15-17 in Panama City, Panama.
Additional research team members include SMU professors David Rosenfield and Renee McDonald and Pricilla Lui from the University of Washington.
Explore further
Feedback to editors

Study finds esketamine injection just after childbirth reduces depression in new mothers
4 hours ago

A new screening protocol can detect aggressive prostate cancers more selectively
5 hours ago

How a new drug prototype regenerates lung tissue
6 hours ago

Why some people with rheumatoid arthritis have pain without inflammation

Researchers show chemical found naturally in cannabis may reduce anxiety-inducing effects of THC
7 hours ago

'Virtual biopsy' lets clinicians analyze skin noninvasively

Research team discovers new way to generate human cartilage

Filling in genomic blanks for disease studies works better for some groups than others

Researchers find new origin of deep brain waves
8 hours ago

Study suggests liquid biopsy could detect and monitor aggressive small-cell lung cancer
Related stories.

Adult interpersonal violence or childhood abuse, neglect increase later diabetes risk
Aug 27, 2023

Racial and gender discrimination among teens exposed to dating violence
Aug 17, 2018

Adolescents of color with a disability experience more racial discrimination, study finds
Aug 24, 2023

Exposure to gun violence is associated with suicidal behavior in Black adults
Feb 6, 2024

Pregnant people with schizophrenia have threefold risk of interpersonal violence
Mar 6, 2023

For black teens, online racial discrimination tied to PTSD symptoms
Jan 3, 2024
Recommended for you

New AI tool creates virtual model of the infant microbiome and predicts neurodevelopmental deficits

AI-assisted breast-cancer screening may reduce unnecessary testing
10 hours ago

'Deaths of despair' among Black Americans surpassed those of white Americans in 2022
11 hours ago

Living near green space associated with fewer emotional problems in preschool-age kids, study finds

Neuroscience study taps into brain network patterns to understand deep focus, attention
Let us know if there is a problem with our content.
Use this form if you have come across a typo, inaccuracy or would like to send an edit request for the content on this page. For general inquiries, please use our contact form . For general feedback, use the public comments section below (please adhere to guidelines ).
Please select the most appropriate category to facilitate processing of your request
Thank you for taking time to provide your feedback to the editors.
Your feedback is important to us. However, we do not guarantee individual replies due to the high volume of messages.
E-mail the story
Your email address is used only to let the recipient know who sent the email. Neither your address nor the recipient's address will be used for any other purpose. The information you enter will appear in your e-mail message and is not retained by Medical Xpress in any form.
Newsletter sign up
Get weekly and/or daily updates delivered to your inbox. You can unsubscribe at any time and we'll never share your details to third parties.
More information Privacy policy
Donate and enjoy an ad-free experience
We keep our content available to everyone. Consider supporting Science X's mission by getting a premium account.
E-mail newsletter
New way to generate human cartilage
University of Montana researchers and their partners have found a new method to generate human cartilage of the head and neck.
Mark Grimes, a biology professor in UM's Division of Biological Sciences, said they have induced stem cells to become the cell type that normally makes up human craniofacial cartilage. Stem cells can replicate themselves and also develop into different types of cells.
"The cells that normally give rise to this type of cartilage are called neural crest cells," Grimes said. "We found a novel method for generating craniofacial organoids from neural crest cells."
Organoids are a simplified, miniature version of an organ that mimic the architecture and gene expression of the organ. "Organoids are a good model for certain human tissues that we can study in ways that are not possible using tissue from human beings," he said.
Grimes said there is a critical unmet need for new methods to regenerate human cartilage for the 230,000 children born annually in the U.S. with craniofacial defects. Growing cartilage in the laboratory also could lead to effective treatments to repair craniofacial cartilage damage due to injuries.
The researchers studied gene expression data at the RNA and protein level to reveal how cartilage cells arise from stem cells. They revealed that stem cells communicate in the early stages to become elastic cartilage, which makes up human ears.
To accomplish this, the team used extensive analysis of biological markers and machine-learning pattern-recognition techniques to understand the cell signaling pathways involved when cells differentiate into cartilage.
It is difficult to reconstruct natural features such as a person's ears, nose or larynx with current plastic surgery techniques, and transplanted tissue is often rejected without immunosuppressants.
"To use patient-derived stem cells to generate craniofacial cartilage in the laboratory, you need to understand the human-specific differentiation mechanisms," Grimes said. "Our aim is to develop a protocol for craniofacial cartilage generation for transplantation using human stem cells."
The research was published in the journal iScience . Besides Grimes, contributing UM authors include Lauren Foltz, Nagashree Avabhrath and Jean-Marc Lanchy. Other authors are Bradly Peterson of Missoula's Pathology Consultants of Western Montana and Tyler Levy, Anthony Possemato and Majd Ariss of Cell Signaling Technology of Danvers, Massachusetts.
- Joint Health
- Human Biology
- Skin Cancer
- Prostate Cancer
- Immune System
- Medical Topics
- Head injury
- Osteoarthritis
- Human skeleton
- Stem cell treatments
- Adult stem cell
Story Source:
Materials provided by The University of Montana . Note: Content may be edited for style and length.
Journal Reference :
- Lauren Foltz, Nagashree Avabhrath, Jean-Marc Lanchy, Tyler Levy, Anthony Possemato, Majd Ariss, Bradley Peterson, Mark Grimes. Craniofacial Chondrogenesis in Organoids from Human Stem Cell-Derived Neural Crest Cells . iScience , 2024; 109585 DOI: 10.1016/j.isci.2024.109585
Cite This Page :
Explore More
- 3D Mouth of an Ancient Jawless Fish
- Connecting Lab-Grown Brain Cells
- Device: Self-Healing Materials, Drug Delivery
- How We Perceive Bitter Taste
- Next-Generation Digital Displays
- Feeling Insulted? How to Rid Yourself of Anger
- Pregnancy Accelerates Biological Aging
- Tiny Plastic Particles Are Found Everywhere
- What's Quieter Than a Fish? A School of Them
- Do Odd Bones Belong to Gigantic Ichthyosaurs?
Trending Topics
Strange & offbeat.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Health Res Policy Syst
How to strengthen a health research system: WHO’s review, whose literature and who is providing leadership?
Stephen r. hanney.
1 Health Economics Research Group, Institute of Health, Environment and Societies, Brunel University London, Uxbridge, UB8 3PH United Kingdom
2 Department of Health Policy, London School of Economics and Political Science, London, United Kingdom
Subhash Pokhrel
Teresa h. jones, annette boaz.
3 Faculty of Health, Social Care and Education, a partnership between Kingston University and St George’s, University of London, London, United Kingdom
Associated Data
The full details of the papers included in the Health Evidence Network Evidence Synthesis are provided in that report, which is cited in this paper as reference [ 30 ]. The additional analysis of papers from Health Research Policy and Systems was based on the open access publications.
Health research is important for the achievement of the Sustainable Development Goals. However, there are many challenges facing health research, including securing sufficient funds, building capacity, producing research findings and using both local and global evidence, and avoiding waste. A WHO initiative addressed these challenges by developing a conceptual framework with four functions to guide the development of national health research systems. Despite some progress, more is needed before health research systems can meet their full potential of improving health systems. The WHO Regional Office for Europe commissioned an evidence synthesis of the systems-level literature. This Opinion piece considers its findings before reflecting on the vast additional literature available on the range of specific health research system functions related to the various challenges. Finally, it considers who should lead research system strengthening.
The evidence synthesis identifies two main approaches for strengthening national health research systems, namely implementing comprehensive and coherent strategies and participation in partnerships. The literature describing these approaches at the systems level also provides data on ways to strengthen each of the four functions of governance, securing financing, capacity-building, and production and use of research. Countries effectively implementing strategies include England, Ireland and Rwanda, whereas West Africa experienced effective partnerships. Recommended policy approaches for system strengthening are context specific. The vast literature on each function and the ever-growing evidence-base are illustrated by considering papers in just one key journal, Health Research Policy and Systems, and analysing the contribution of two national studies. A review of the functions of the Iranian system identifies over 200 relevant and mostly national records; an analysis of the creation of the English National Institute for Health Research describes the key leadership role played by the health department. Furthermore, WHO is playing leadership roles in helping coordinate partnerships within and across health research systems that have been attempting to tackle the COVID-19 crisis.
Conclusions
The evidence synthesis provides a firm basis for decision-making by policy-makers and research leaders looking to strengthen national health research systems within their own national context. It identifies five crucial policy approaches — conducting situation analysis, sustaining a comprehensive strategy, engaging stakeholders, evaluating impacts on health systems, and partnership participation. The vast and ever-growing additional literature could provide further perspectives, including on crucial leadership roles for health ministries.
Interest in strengthening health research systems has intensified following increasing recognition of the importance of research in achieving key goals such as universal health coverage [ 1 ] and the Sustainable Development Goals (SDGs) [ 2 ]. However, achieving progress in health research faces many challenges, including securing sufficient funds [ 3 – 9 ], building and retaining capacity [ 3 , 7 , 10 – 14 ], producing research findings, and using both local and global evidence [ 1 , 15 – 20 ].
Chalmers and Glasziou [ 21 ] dramatically highlighted the extent of the challenges facing health research by claiming, in 2009, that even where there was funding and capacity, up to 85% of all biomedical research was wasted because it asked the wrong questions, was poorly designed, or was either not published or poorly reported, with only about 50% of studies being published in full.
Many of these challenges have long been recognised and the adoption of a systems approach advocated. In 2000, the Bangkok Declaration on Health Research for Development promoted the importance of a systems approach, following consideration of how a health research system could “be integrated with a nation’s health development plan” [ 15 ]. It suggested that establishing and strengthening an effective health research system needed coherent and coordinated health research strategies [ 15 ]. National strategies should have specific combinations of various health research system components, tailored to the country’s circumstances.
The WHO’s Knowledge for Better Health initiative involved further work on these issues [ 3 , 16 ]. The Mexico Statement on Health Research, issued in 2004 by a Ministerial Summit, called for nations to take actions to strengthen their national health research systems (NHRSs). It was endorsed in 2005 by the Fifty-eighth World Health Assembly in a resolution committing its Member States to strengthening their NHRSs as a pathway to improve their overall health system [ 22 ].
As part of the initiative, Pang et al. [ 3 ] developed a conceptual framework to guide the analysis and strengthening of health research systems, including development of a health research strategy. While this can be used for planning, monitoring and evaluation of health research systems, it did not claim to provide a precise blueprint. The framework defined a health research system as “the people, institutions, and activities whose primary purpose in relation to research is to generate high-quality knowledge that can be used to promote, restore, and/or maintain the health status of populations; it should include the mechanisms adopted to encourage the utilization of research” [ 3 ].
The framework indicates the range of constituent components and how they can best be brought together into a coherent system. It identified four main functions for an effective system, namely stewardship, financing, capacity-building (or creating and sustaining resources), and producing and using research [ 3 ]. Each function is defined by operational components and consists of one or more of a total of nine such components.
Since then, progress is evidenced by analyses of developments in individual countries, including the National Institute for Health Research (NIHR) in England [ 23 – 25 ], and in repeat surveys conducted in various WHO regions, including Africa [ 4 , 26 , 27 ] and the Pan-American Health Organization (PAHO) [ 28 ]. However, as reported by those surveys and other publications, many challenges remain. For example, in February 2020 a new analysis by the WHO Global Observatory on Health R&D examined health research funding, concluding that “neglected diseases such as those on the WHO list of neglected tropical diseases remain very neglected in terms of R&D investments” [ 29 ].
Nevertheless, there are various initiatives underway, including in WHO’s Regional Office for Europe, which commissioned an evidence synthesis on the topic as part of its Action Plan to Strengthen the use of Evidence, Information and Research for Policy-making in the WHO European Region [ 18 ]. The synthesis is published in the WHO Region’s Health Evidence Network (HEN) report series and consists of a scoping review addressing the question “What is the evidence on policies, interventions and tools for establishing and/or strengthening NHRSs and their effectiveness?” [ 30 ].
The evidence synthesis focuses on the systems level and so primarily includes publications taking a systems approach at either the national or multi-national level. Not surprisingly, Health Research Policy and Systems ( HARPS ) is the single largest source of papers included in the HEN report. These were papers directly identified in the review’s search or papers included in the HEN report to illustrate a key point because they had been cited in one of the WHO reports or other systems-level collations of papers included in the synthesis.
While the system level papers did provide considerable data about each function, limited resources to conduct the scoping review meant that we had to exclude papers focusing solely on one specific function of a health research system or on just one field of health research. As acknowledged in the HEN report’s agenda for further research, there is a large number of publications (papers and grey literature) covering each function [ 30 ]. Therefore, reviewing all of these publications would be a major task but some exploration of the extent of the task, and the nature of such literature, could be informative. Furthermore, additional papers are continuously emerging, including from the various initiatives that are ongoing or just underway, for example, the European Health Research Network [ 31 ].
The three sections of this paper sequentially address the question of how to strengthen a health research system by:
- Describing key points and conclusions from WHO’s HEN report.
- Illustrating the nature of the ever-widening literature available on each function, or component, of a health research system by examining two sources in particular. First, the full range of papers published in HARPS in the 30 months up to February 2020. Second, the range of data gathered from publications or interviews that is included in detailed studies of the national health research systems in two countries – Iran [ 32 ] and England [ 33 ]; between them, these two papers also illustrate diverse aspects of the additional material that could be drawn upon.
- Considering a key question in the analysis of the current and future initiatives, namely who is going to steer the development of health research systems? Here, information and insights from the HEN about this sometimes-controversial issue, along with wider continuing analysis, are drawn on in the more flexible and speculative way that can be undertaken in an Opinion piece compared to a formal evidence synthesis.
WHO’s review, whose literature and who is providing leadership?
Who’s review.
The evidence synthesis described by the HEN report [ 30 ] starts by describing the importance of NHRSs in helping to achieve universal health coverage [ 1 ] and the SDGs [ 2 ]. It goes on to analyse the challenges facing health research and describes how issues remain unresolved despite the development and application of a systems approach including WHO’s framework for health research systems [ 3 ]. Many countries do not have comprehensive national health research policies or strategies that would facilitate the introduction of a systems approach. Therefore, challenges remain around two key and overlapping sets of issues. First, how to develop a systems approach to maximise the benefits from the research resources available – this can be a challenge even in high-income countries with considerable research funding. Second, how best to strengthen each specific function and component of a health research system [ 30 ].
The HEN identifies two main systems-level approaches to strengthening NHRSs. The first is comprehensive and coherent strategies, which can be contained in either policy documents, such as those from the English NIHR [ 34 ], the Irish Health Research Board (HRB) [ 35 ] and the Rwandan Ministry of Health [ 14 ], or in specific legislation as in the Philippines [ 36 ]. The second systems-level approach involves partnerships and multi-country initiatives, especially with international organisations. Two initiatives from the West African Health Organization (WAHO) are particularly important examples [ 5 , 37 ]. Here, the ministries of health of the 15 West African member countries worked together in a joint initiative covering all the countries and with funding and expertise from a range of partners, including the Council on Health Research for Development (COHRED), the Canadian International Research Centre, the Special Programme for Research and Training in Tropical Diseases, and the Wellcome Trust. All WHO Regions have seen multi-country activities by WHO and/or COHRED to strengthen NHRSs, including the repeat surveys that identify areas for action [ 4 , 26 , 28 ].
Then, broadly using the WHO framework as the structure [ 3 ], the HEN identifies key points from systems-level literature on each of the four functions and nine components. The components of the stewardship and governance function include defining a vision, ethical review, research priority-setting, and appropriate monitoring and evaluation [ 3 ]. Consultation with health system stakeholders should enhance the relevance of the research priorities to the healthcare system, with examples of extensive priority-setting engagement activities sometimes being seen as a key aspect of building the NHRS as in Brazil [ 38 ]. Evaluating the impact of research on policy and practice should help researchers to focus on achieving such impact and was therefore promoted in the World Health Report 2013 [ 1 ].
Securing finance can involve obtaining funding from sources within the country and from external donors or multi-national organisations [ 30 ]. Targets for research expenditure, such as the 2% of national health expenditure set by the 1990 Commission on Health Research for Development [ 39 ], can usefully be brought into health research system strategies as in Rwanda [ 14 ]. Major health research strategies from countries within the European Union can highlight the importance of European Union funding as in France [ 40 ], Ireland [ 35 ] and Malta [ 41 ]. Requests for funding can be more effective when linked to other parts of the overall strategy, including identified priorities that need supporting through donor funding [ 42 ] and assessments of the benefits obtained from previous funding such as in England [ 24 ].
Capacity-building involves building, strengthening and sustaining the human and physical capacity to conduct, absorb and utilise health research [ 3 ]. In 2016, Santoro et al. [ 43 ] identified the generally low levels of research production in 17 countries of the former Soviet Union and south-eastern Europe and made recommendations for the sustained investment in training and career development of researchers, which should go beyond scholarships for training abroad and involve comprehensive strategies to ensure clear career structures. Strategies such as that from Inserm in France set out comprehensive plans for capacity-building [ 40 ] and strategies in both England and South Africa addressed priority gaps identified in the research capacity within the healthcare professions [ 34 , 44 ]. Donors can play an important part in building capacity but, recognising the need to avoid donor domination, often do so through partnerships. These can take diverse forms ranging from multi-country initiatives, such as that by WAHO, which included an initiative focusing on the challenges of post-conflict countries but was unable to meet all the needs [ 37 ], to accounts that focus on the partnership to address a broad range of capacity issues in a single country such as Malawi [ 7 ], to partnerships between individual institutions. Examples of the latter can feature particular challenges – the James Cook University in Australia worked with the Atoifi Adventist Hospital in Malaita, the most populous province of the Solomon Islands, to start establishing health research system capacity on the island using an inclusive, participatory approach [ 45 ]. Increasingly, there are also south–south partnerships, for example, an account of the Panamanian health research system described how the country’s first doctoral programme in biotechnology was established with support from Acharya Nagarjuna University in India [ 46 ]. The Rwandan strategy described plans to tackle the ‘brain drain’ through making the country an appealing place to conduct health research in terms of job requirements and providing opportunities for career advancement [ 14 ].
The three mutually reinforcing components of the producing and using research function encourage the production of scientifically valid findings that are relevant for users and communicated to them in an effective manner [ 30 ]. Major research funding bodies increasingly seek to address the waste issues raised by Chalmers and Glasziou [ 21 ] by working together in the Ensuring Value in Research (EViR) Funders’ Collaboration and Development Forum. It issued a consensus statement committing the organisations signing it to “require robust research design, conduct and analysis” [ 47 ]. The Forum is convened by the English NIHR, the Netherlands Organization for Health Research and Development, and the Patient-Centered Outcomes Research Institute (United States) with the active support of major research funding organisations from Australia, Ireland (HRB), Italy, Sweden and Wales, plus the Special Programme for Research and Training in Tropical Diseases [ 48 ]. The first WAHO intervention also worked to boost research publications, including by creating a regional peer-reviewed, multilingual journal [ 5 ]. How research is produced can increase the chance that the evidence will be used in the health system, for example, the English NIHR strategy noted that leading medical centres with substantial funding to conduct translational research can act as “early adopters of new insights in technologies, techniques and treatments for improving health” [ 34 ].
Fostering the use of research requires specific knowledge translation and management approaches that draw on both locally produced and globally available evidence. Various health research strategies promote the role of Cochrane, including in England, where a unified knowledge management system to meet the needs of various stakeholders, including patients and their carers, involves funding both Cochrane and a review centre focusing on the needs of the National Health System [ 34 ]. In Ireland, the HRB strategy facilitated evidence-informed decisions through promoting access to the Cochrane Library and supporting training in conducting high-quality Cochrane reviews [ 35 ]. South Africa Cochrane featured as an important element in the NHRS [ 44 ]. The Rwandan strategy stated that “The Government of Rwanda is committed to using research findings to make evidence-based decisions that will improve health in Rwanda” [ 14 ]. It aimed to orientate various functions, including agenda-setting, monitoring and evaluation, and capacity-building, towards facilitating this challenging aim. The World Health Report 2013 highlighted various mechanisms that health research systems could adopt, including EVIPNet (Evidence-informed Policy Network), to promote the use of research [ 1 , 49 ].
The review also considers the effectiveness of approaches to strengthening NHRSs. Several reviews identified the effectiveness of the comprehensive approach taken by Professor Dame Sally Davies in creating the English NHRS [ 23 , 25 , 50 ]. The title of one analysis, ‘NIHR at 10: 100 examples, 10 themes, 1 transformation’, emphasises that the success of the NIHR depended on a range of elements being brought together in one transformation [ 25 , 50 ]. One of the 10 themes was the involvement of patients in decisions about research priorities and processes and, based on this, another recent analysis highlighted England and Alberta (Canada) as having health research systems that had made important progress [ 51 ]. Davies herself reflected on the success of the NIHR and stated: “What we envisaged was integrating a health research system into the health care delivery system so that the two would become interdependent and synergistic ” [ 24 ]. WHO’s Regional Office for Africa drew on their series of surveys of the performance of countries in building NHRSs and analysed the data from the 2014 and 2018 surveys using the NHRS barometer that they developed to score progress on a range of items linked to the list of NHRS functions [ 11 , 26 ]. In the 2014 survey, the Rwandan system was identified as the best performing and it, along with the majority of systems, was reported to have further improved in the 2018 survey; by then, South Africa was reported to have the best performance in Africa. The surveys also illustrate how the multi-country approach makes a useful contribution to strengthening NHRSs by helping to target action. Furthermore, the WAHO interventions made some progress but, while the evaluations identified the importance of political will and leadership provided by WAHO’s parent organisation of West African states, they also emphasised that building capacity for a whole NHRS is a significant task requiring commitment over the long-term [ 17 , 37 ].
The HEN review collated a range of examples of tools for NHRS strengthening. These were identified from the systems level discussions of NHRS strategies and partnerships and/or the major reports calling for NHRS strengthening such as the World Health Report 2013 [ 1 ]. The HEN lists these in an Annex [ 30 ].
The discussion in the HEN draws on the literature that was included to identify five key policies that those responsible for strengthening NHRSs could consider [ 30 ], namely conduct context, or situational, analyses to inform strengthening activities [ 5 , 34 , 35 , 37 , 52 – 54 ], develop a comprehensive and coherent strategy [ 14 , 34 – 36 ], engage stakeholders in the development and operation of the strategy [ 7 , 23 , 34 , 35 , 38 , 41 , 44 , 51 , 55 – 59 ], adopt monitoring and evaluation tools that focus on the objectives of the NHRS, including health improvement [ 1 , 14 , 24 , 60 , 61 ], and develop partnerships [ 5 , 11 , 28 , 37 , 62 ]. Examples of the evidence to support or illustrate each policy are given in Table 1 .
Policies to strengthen National Health Research Systems and supporting evidence
Source: Data extracted from Health Evidence Network report 69 (Hanney et al., 2020) [ 30 ]
COHRED Council on Health Research for Development, HEN Health Evidence Network, HRB Health Research Board, NHRS National Health Research System, NIHR National Institute for Health Research, PAHO Pan-American Health Organization, WAHO West African Health Organization
In summary, therefore, this section shows that the WHO evidence synthesis, published as a HEN report [ 30 ], provides a firm basis for decision-making by policy-makers and research leaders looking to strengthen the health research system in their country. It analyses, in turn, the individual functions and components within a system and identifies a series of tools that can be used for strengthening many of them. Finally, this section highlights the five crucial policy approaches that the HEN report suggests can be applied as appropriate to the context of the country (Table (Table1 1 ).
Whose literature?
As noted above, the HEN was a scoping review and focused on the literature at the systems level rather than on publications (papers and grey literature) related solely to specific functions, types or fields of research [ 30 ]. Therefore, there is scope for further work to incorporate an even wider range of publications than the 112 included in the HEN review [ 30 ]. The discussion in the HEN suggests that further research could usefully take the form of a series of reviews on the extensive literature on each of the NHRS functions or components, which could then be collated [ 30 ]. Just two of the many available sources illustrate the nature of the vast literature available on each function, or component, of a health research system and the way the literature on that, and the system level developments, is ever-widening. First, we can examine the papers published in HARPS, the specialist journal in the field of building NHRSs. Second, we can focus on two very different but detailed studies of individual NHRSs – one conducted for a PhD thesis to show the 50 year history of the development of all the functions in the Iranian health research system [ 32 ] and the other an interview-based study to understand the factors behind the creation of the NIHR with its new strategy [ 33 ].
In terms of further reviews of the literature on specific functions or components, HARPS would probably be a key source. In the summer of 2017, an analysis by the retiring editors of the papers published in the journal from its inception in 2002 identified many papers that had been published on each of the functions or components of a health research system [ 63 ]. While this editors’ analysis was included in the HEN review because it organised its discussion of the papers at the systems level, the individual papers in it were, in general, only included in the HEN review if they, too, adopted a systems approach at the national or partnership level, or were also cited in a report such as the World Health Report 2013 [ 1 ]. Examples of such papers include Viergever et al. on priority-setting [ 59 ], Bates et al. on capacity-building [ 64 ], and Lavis et al. on the SUPPORT tools for evidence-informed policy-making [ 65 ]. Therefore, many additional papers related to specific functions (or fields) could be consulted, in a formal review or otherwise, in any future series of reviews, each with a narrow focus on strengthening a specific function.
To further inform this current Opinion piece, a quick ‘hand-search’ was conducted of the papers published in HARPS in the 30 months since the previous analysis in mid-2017 [ 63 ]. This again identified a wide range of papers on specific components, especially priority-setting, evaluation of research impacts, capacity-building and the translation of research (or knowledge mobilisation). Various papers linked the final two points and discussed capacity-building and knowledge translation [ 13 , 66 ]. Such a focus is entirely consistent with the aim described by the incoming editors in Autumn 2017 of bringing “all elements of the research–policy world together – such that the research which is done is useful and that it is used” [ 67 ]. In this more recent phase of HARPS , there have also been important papers on issues related to the policies ‘recommended’ at the end of the HEN and listed above, including the contribution of stakeholder engagement in research [ 68 ].
The more recent papers could sometimes provide useful further tools on specific functions. Their narrow focus meant they had not been directly included through the HEN search and, further, they had not been included in any of the major reports also used as sources for tools such as the World Health Report 2013 [ 1 ]. In some instances, this was because they were too recent, for example, the ISRIA statement by Adam et al. [ 69 ] describing the ten-point guidelines for an effective process of research impact assessment prepared by the International School on Research Impact Assessment (ISRIA). Even more recently, the Intervention Scalability Assessment Tool, developed by Milat et al. [ 70 ], was proposed for use not only by health policy-makers and practitioners for selecting interventions to scale up but also to help design research to fill evidence gaps. This analysis of the papers from just one journal reinforces the message that there is likely to be a plentiful supply of literature for a future review on any of the main specific components.
This message is further reinforced by a more detailed analysis of the papers in HARPS in the first 2 months of 2020. Articles on the main components of a NHRS were supplemented by some important papers on topics that are highly relevant but which feature less frequently in HARPS. These include a study aimed at reducing the research waste that arises from disproportionate regulation by examining the practices for exempting low-risk research from ethics review in four high-income countries [ 71 ], the Global Observatory’s paper on research funding described earlier [ 29 ], a study on the governance of national health research funding institutions [ 72 ], and one on a more recent topic of growing significance – an analysis of attempts to boost gender equality in health research [ 73 ]. Additionally, some of the papers on specific components, such as impact evaluation or use of evidence, are extending the analysis. Examples include consideration of how research impact assessments are implemented in practice within research organisations [ 74 ] and how evidence is used in decision-making in crisis zones [ 75 ]. To illustrate the volume of studies being produced, there has been a flurry of studies, in the first 2 months of 2020 alone, on the collaboration and coproduction of health research. The titles include ‘Building an integrated knowledge translation (IKT) evidence base: colloquium proceedings and research direction’ [ 76 ], ‘Using a ‘rich picture’ to facilitate systems thinking in research coproduction’ [ 77 ], ‘Exploring the evolution of engagement between academic public health researchers and decision-makers: from initiation to dissolution’ [ 78 ], ‘Research co-design in health: a rapid overview of reviews’ [ 79 ], and ‘Conceptualising the initiation of researcher and research user partnerships: a meta-narrative review’ [ 80 ].
Finally, another article in May 2020 presented a new conceptual model for health research systems to strengthen health inequalities research [ 81 ]. Here, we have focused on just one journal, HARPS, because it was the largest single source of papers in the HEN report, which totalled 140 publications (additional publications were included to the 112 in the review to help set the background, provide examples of key tools, etc). However, even with the review’s focus on the system level, HARPS only provided 22% (31 out of 140) of the publications; 31% (43 of 140) came from other journals and 47% (66 of 140) were other types of publication. If the focus was shifted to including papers on specific functions it is highly likely that there would be a higher proportion of papers from other journals.
The authors of two single-country papers on the development of the health research system, Mansoori [ 32 ] about Iran and Atkinson et al. [ 33 ] on the creation of the NIHR in England, both highlight the importance of context but also claim their findings could have wider application. Examining these two papers is also informative because of the differences between the studies, including one being located in a low- or middle-income country, and the other not.
Mansoori’s narrative review of studies addressing the health research system of Iran included 204 relevant and mostly national records, categorised using an approach informed by the functions and components of WHO’s NHRS framework [ 32 ]. The papers and grey literature documents included were all available in English or Persian, and mostly published in journals other than HARPS, and illustrate the vast literature available at a global level on the various components of a NHRS . They informed an impressively detailed account of the various NHRS components and the attempts to strengthen them. For example, the account of the development of the national level ethical overview includes a fully documented chronology of the progress over 25 years and some insightful analysis of how the progress was facilitated by the pivotal role of Professor Bagher Larijani, who was a prominent medical practitioner, leading researcher and founder of the Medical Ethics Research Centre in Iran. He was able to “use the confidence that Iranian authorities had in him as an opportunity” [ 32 ].
While Mansoori’s review was included in the HEN review, only a tiny fraction of the available data about Iran could be included, primarily in a brief description of the system’s effectiveness [ 30 ]. However, the full paper could usefully inform the approach of researchers and/or policy-makers planning a detailed analysis of their own NHRS prior to embarking on exercises to strengthen it, and “ [t] he findings emphasized that improvement of HRS functions requires addressing context-specific problems” [ 32 ]. As an illustration, Mansoori’s review identified a need for “ a more systematic, inclusive” approach to research priority-setting [ 32 ] and, in the same stream of research, she co-led just such a priority-setting exercise to help address the knowledge gaps related to achieving both Iran’s national health policies and the SDGs [ 82 ].
Atkinson et al. examined the creation of what might be viewed as the most successful attempt to strengthen a health research system in their paper ‘‘All the stars were aligned’? The origins of England’s National Institute for Health Research’ [ 33 ]. Compared with Mansoori, the authors adopted a different but equally detailed approach in their analysis, which was conducted principally through interviews and a witness seminar but also drew on the existing literature and documents [ 33 ]. They showed how the formation of the NIHR was led from the Department of Health by a key group driven by Sally Davies. They aimed to improve patient care through both the strengthening of evidence-based medicine and through boosting the infrastructure to facilitate pharmaceutical clinical trials that would also meet wider industrial and economic goals.
As with Mansoori’s study, consideration was given to how the full analysis could be informative to any planned detailed study or reforms in any other country. The key observations were similar to the recommendations from the HEN report with a focus on stakeholder engagement and building support: “ [t] wo measures likely to contribute to political support are to place the greatest emphasis on ‘problem’ rather than ‘investigation’ research, and to devote attention to measuring and reporting research ‘payback’ ” [ 33 ]. Atkinson et al.’s paper is also a link to the other main source considered here because it was a recent paper published in HARPS.
In summary, if further analysis and research beyond that in the WHO evidence synthesis [ 30 ] is thought to be relevant in the particular country looking to strengthen its health research system, this Opinion piece indicates some of the types of additional sources of information that are available and how they might be organised. The vast literature on each function and the ever-growing evidence base are illustrated by considering papers in just one key journal, HARPs, and analysing the contribution of two national studies. A review of the functions of the Iranian system identifies over 200 relevant, mostly national, records and an analysis of the creation of the English NIHR describes the key leadership role played from the health department.
Who is providing leadership?
The above analysis demonstrates that there is no shortage of useful material on which to draw when strengthening health research systems. However, key questions remain as to who might best lead or steer attempts to strengthen such a system.
The papers by both Mansoori [ 32 ] and Atkinson et al. [ 33 ] illustrate that, where a key committed individual has the capacity and opportunity to provide leadership, this can be a vital element in making progress. However, the institutional factors are also crucial.
The HEN developed the argument that a department or ministry of health will have a particular interest and perhaps experience in promoting research agendas that meet the needs of the healthcare system and in helping to develop mechanisms to use the findings from such research, where appropriate, to inform local policy and practice [ 30 ]. The health ministry or a research council responsible to it played an important role in the various systems identified above as being effective, as was also the case in the WAHO initiative [ 30 ]. In some cases, as with Zambia, more progress was made once the ministry of health elected to play a more important role, sometimes in place of other stakeholders [ 57 ]. Examples of the important role that health ministries can play were described in the 2013 World Health Report, including on Paraguay: “ the support of the Minister of Health backed by the President of Paraguay has been a key factor in the development of a national health research system” [ 1 ]. Additionally, naturally enough, the activities of the various WHO regional offices in boosting NHRSs tend to focus on working with the national ministries of health, including work in Europe [ 31 ] and by PAHO [ 28 ]. Conversely, several analyses illustrate that progress in strengthening the NHRS might be limited where key parts of the ministry of health, for whatever reason, do not provide support [ 9 , 83 ].
Nevertheless, some disadvantages or dangers were identified when the ministry of health plays the leading role. First, in England prior to the creation of the NIHR as well as in some other countries, the research funds controlled by the health ministry were sometimes appropriated by other parts of the health system when they were under particular pressure for resources [ 84 ]. Similarly, there have been a few reports that health research funding lost out when donor funds that had previously been allocated specifically for health research programmes were replaced by donations of funds to be allocated by the nation’s own health system according to its own priorities [ 85 , 86 ]. One way of attempting to mitigate the danger is, as undertaken by the NIHR and described by Atkinson, by building support for health research through measuring and reporting the payback from research [ 24 , 33 ].
The second danger arises because, traditionally, many researchers argued that the best science came when they had the freedom to identify the key research topics, rather than having priorities set by others [ 84 ]. Therefore, they argued, the responsibility for funding and organising health research should be left to organisations that are part of the research system and independent of the health system [ 84 ]. Furthermore, despite the growth of interest in coproduction approaches noted above, there have also been recent doubts raised about the assumption that coproduction is always the most appropriate approach [ 87 ]. This issue clearly requires sensitive handling. Indeed, Atkinson et al. [ 33 ] argue that one of the great successes of the NIHR is that this issue has been so skilfully handled by the NIHR that external input, or stakeholder engagement, in setting agendas has become widely accepted and the structures created give ministers a sense of ownership without sacrificing scientific independence.
The efforts of WAHO [ 5 , 37 ] and the WHO regional offices for Africa and PAHO [ 11 , 26 , 28 , 62 ] indicate that partnerships can be helpful. In Europe, the WHO regional office worked with Member States to create the European Health Research Network, which is intended to help nations with limited NHRSs who wish to make more progress [ 31 ].
Partnerships can provide important support and encouragement, but the evidence suggests there must be strong political will somewhere within the political and/or health systems for a health research system to be fully strengthened. The Central Asian countries in WHO’s European Region seem to provide an illustration of this point. A COHRED collaborative initiative successfully resulted in situation analyses being produced in each country and then jointly discussed as the basis for action [ 88 ], but according to the analysis by Santoro et al. [ 43 ], limited progress seems to have been made in the subsequent years.
The importance of partnerships and collaboration in focusing research efforts in an extreme crisis, with a leadership role for the WHO, has been seen in the race to find treatments for COVID-19 and vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes the COVID-19 disease [ 89 ]. In many NHRSs across the globe, including in the Philippines, scientists are coming together to participate in WHO’s Solidarity Trial, which will test the safety and effectiveness of various possible therapies for treating COVID-19 [ 90 ]. Sarah Gilbert, leader of Oxford University’s Jenner Institute’s work on developing one of the leading vaccine candidates explained that cooperation was vital for tackling the crisis: “Work is continuing at a very fast pace, and I am in no doubt that we will see an unprecedented spirit of collaboration and cooperation, convened by WHO, as we move towards a shared global goal of COVID-19 prevention through vaccination” [ 91 ]. A key issue going forward is how such cooperation can be built on in strengthening NHRSs into the future. For now, it is recommended that a prospective study be conducted to analyse all that is being done in different NHRSs to speed up research during the pandemic, with a view to taking lessons about cooperation, partnerships and other matters into strengthening NHRSs in the future [ 89 ].
The WHO evidence synthesis, published as a HEN report [ 30 ], provides a firm basis for decision-making by policy-makers and research leaders looking to strengthen the health research system in their country. It identifies five crucial policy approaches that can be applied as appropriate to the context of the country – conducting situation analyses, sustaining a comprehensive strategy, engaging stakeholders, evaluating impacts on health policies and practices, and partnership participation. It also analyses, in turn, the individual functions and components within a system and identifies a series of tools that can be used for strengthening many of them.
If further analysis and research is thought to be relevant in the particular country looking to strengthen its health research system, this Opinion piece indicates some of the types of additional sources of information that are available. The Opinion piece also discusses aspects of the sometimes-controversial question of who should lead or steer attempts to strengthen NHRSs. Again, the context of the particular nation will be crucial in determining the most appropriate course to take, as emphasised by both Mansoori [ 32 ] and Atkinson et al. [ 33 ], but at least some involvement of the ministry of health is likely to be beneficial; additionally, sometimes, key individuals can play a crucial leadership role in strengthening the whole system or one component. In countries with a less developed tradition of conducting health research, partnerships with other countries and/or with international organisations can help lead the progress and learning for all partners. The valuable role that international organisations, such as WHO, can play in leading partnerships and cooperation to strengthen health research systems is being highlighted during the COVID-19 crisis.
Overall, therefore, the full WHO HEN report not only provides a detailed analysis of NHRS strengthening, it also provides a structure within which an even wider and ongoing literature can be considered. Additionally, it contains a perhaps more nuanced account, on which this paper builds, of some aspects of the literature around the issue of who should provide leadership in developing NHRSs and identifies the importance of ministry of health involvement.
Acknowledgements
We thank colleagues at WHO’s Regional Office for Europe for the inputs to the original Health Evidence Network Evidence Synthesis. The authors are responsible for the content of this Opinion piece.
Abbreviations
Authors’ contributions.
SP, LK and SH planned the original phase of the WHO evidence synthesis, including the search strategy. LK led the original literature search and contributed article selection and data extraction and analysis. AB and SH planned the second phase of the evidence synthesis. TJ led the second phase of the literature search and contributed to the article selection and data extraction. AB contributed to the final version of the Health Evidence Network report. SH led the data extraction and analysis and drafting of the report. SH conducted the additional analysis of the literature and initial drafting for this Opinion piece. All authors commented on the Opinion piece and approved the final version.
The WHO’s Regional Office for Europe funded the Health Evidence Network Evidence Synthesis. The additional literature searching and analysis for this Opinion piece, along with its drafting, was unfunded. Annette Boaz, Kingston University and St George’s University of London, is supported by the National Institute for Health Research (NIHR) Applied Research Collaboration South London (NIHR ARC South London) at King’s College Hospital NHS Foundation Trust. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Availability of data and materials
Ethics approval and consent to participate.
Not applicable.
Consent for publication
The full version of the evidence synthesis was published by WHO’s Regional Office for Europe, and all the data used for the report and this Opinion piece are publicly available.
Competing interests
The authors have no competing interests to declare. AB is a member of the World Health Organization European Advisory Committee on Health Research. SH was co-editor of Health Research Policy and Systems from 2006 to 2017.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Stephen R. Hanney, Email: [email protected] .
Lucy Kanya, Email: [email protected] .
Subhash Pokhrel, Email: [email protected] .
Teresa H. Jones, Email: [email protected] .
Annette Boaz, Email: [email protected] .
UT Academic Affairs Presents at Innovating Teaching and Learning in the Era of Generative AI Conference

Four members of UT Austin’s Academic Affairs community presented at a recent The University of Texas System conference hosted by UT San Antonio’s Office of Academic Innovation . Strategic Academic Initiatives postdoctoral fellows Natalie Murray, PhD, and Raj Sankaranarayanan, PhD, Kory Bieg, associate professor and associate dean of Academic Affairs in the School of Architecture, and Julie Schell, EdD, assistant vice provost and director of the Office of Academic Technology, all shared their expertise on integrating generative AI into higher education.
The conference, Innovating Teaching and Learning in the Era of Generative AI , brought together educators from across UT System to explore how generative AI and other emerging technologies are transforming teaching and learning. It was held in-person March 6-8.
Read the full story »
Explore Latest Articles
Apr 10, 2024
Clint Dawson and Stephen Vladeck Honored With President’s Research Impact Award

Apr 09, 2024
UT’s Excellence and Impact On Display in Latest Graduate School Rankings

Apr 08, 2024
25 Questions (and Answers!) About the Great North American Eclipse


Turn Your Curiosity Into Discovery
Latest facts.

Approach for Using 5 Tips To Help You Write Your Dissertation

Dmitry Doev Projects as CEO of VIS Group Doev Dmitry Vitalievich
40 facts about elektrostal.
Written by Lanette Mayes
Modified & Updated: 02 Mar 2024
Reviewed by Jessica Corbett

Elektrostal is a vibrant city located in the Moscow Oblast region of Russia. With a rich history, stunning architecture, and a thriving community, Elektrostal is a city that has much to offer. Whether you are a history buff, nature enthusiast, or simply curious about different cultures, Elektrostal is sure to captivate you.
This article will provide you with 40 fascinating facts about Elektrostal, giving you a better understanding of why this city is worth exploring. From its origins as an industrial hub to its modern-day charm, we will delve into the various aspects that make Elektrostal a unique and must-visit destination.
So, join us as we uncover the hidden treasures of Elektrostal and discover what makes this city a true gem in the heart of Russia.
Key Takeaways:
- Elektrostal, known as the “Motor City of Russia,” is a vibrant and growing city with a rich industrial history, offering diverse cultural experiences and a strong commitment to environmental sustainability.
- With its convenient location near Moscow, Elektrostal provides a picturesque landscape, vibrant nightlife, and a range of recreational activities, making it an ideal destination for residents and visitors alike.
Known as the “Motor City of Russia.”
Elektrostal, a city located in the Moscow Oblast region of Russia, earned the nickname “Motor City” due to its significant involvement in the automotive industry.
Home to the Elektrostal Metallurgical Plant.
Elektrostal is renowned for its metallurgical plant, which has been producing high-quality steel and alloys since its establishment in 1916.
Boasts a rich industrial heritage.
Elektrostal has a long history of industrial development, contributing to the growth and progress of the region.
Founded in 1916.
The city of Elektrostal was founded in 1916 as a result of the construction of the Elektrostal Metallurgical Plant.
Located approximately 50 kilometers east of Moscow.
Elektrostal is situated in close proximity to the Russian capital, making it easily accessible for both residents and visitors.
Known for its vibrant cultural scene.
Elektrostal is home to several cultural institutions, including museums, theaters, and art galleries that showcase the city’s rich artistic heritage.
A popular destination for nature lovers.
Surrounded by picturesque landscapes and forests, Elektrostal offers ample opportunities for outdoor activities such as hiking, camping, and birdwatching.
Hosts the annual Elektrostal City Day celebrations.
Every year, Elektrostal organizes festive events and activities to celebrate its founding, bringing together residents and visitors in a spirit of unity and joy.
Has a population of approximately 160,000 people.
Elektrostal is home to a diverse and vibrant community of around 160,000 residents, contributing to its dynamic atmosphere.
Boasts excellent education facilities.
The city is known for its well-established educational institutions, providing quality education to students of all ages.
A center for scientific research and innovation.
Elektrostal serves as an important hub for scientific research, particularly in the fields of metallurgy, materials science, and engineering.
Surrounded by picturesque lakes.
The city is blessed with numerous beautiful lakes, offering scenic views and recreational opportunities for locals and visitors alike.
Well-connected transportation system.
Elektrostal benefits from an efficient transportation network, including highways, railways, and public transportation options, ensuring convenient travel within and beyond the city.
Famous for its traditional Russian cuisine.
Food enthusiasts can indulge in authentic Russian dishes at numerous restaurants and cafes scattered throughout Elektrostal.
Home to notable architectural landmarks.
Elektrostal boasts impressive architecture, including the Church of the Transfiguration of the Lord and the Elektrostal Palace of Culture.
Offers a wide range of recreational facilities.
Residents and visitors can enjoy various recreational activities, such as sports complexes, swimming pools, and fitness centers, enhancing the overall quality of life.
Provides a high standard of healthcare.
Elektrostal is equipped with modern medical facilities, ensuring residents have access to quality healthcare services.
Home to the Elektrostal History Museum.
The Elektrostal History Museum showcases the city’s fascinating past through exhibitions and displays.
A hub for sports enthusiasts.
Elektrostal is passionate about sports, with numerous stadiums, arenas, and sports clubs offering opportunities for athletes and spectators.
Celebrates diverse cultural festivals.
Throughout the year, Elektrostal hosts a variety of cultural festivals, celebrating different ethnicities, traditions, and art forms.
Electric power played a significant role in its early development.
Elektrostal owes its name and initial growth to the establishment of electric power stations and the utilization of electricity in the industrial sector.
Boasts a thriving economy.
The city’s strong industrial base, coupled with its strategic location near Moscow, has contributed to Elektrostal’s prosperous economic status.
Houses the Elektrostal Drama Theater.
The Elektrostal Drama Theater is a cultural centerpiece, attracting theater enthusiasts from far and wide.
Popular destination for winter sports.
Elektrostal’s proximity to ski resorts and winter sport facilities makes it a favorite destination for skiing, snowboarding, and other winter activities.
Promotes environmental sustainability.
Elektrostal prioritizes environmental protection and sustainability, implementing initiatives to reduce pollution and preserve natural resources.
Home to renowned educational institutions.
Elektrostal is known for its prestigious schools and universities, offering a wide range of academic programs to students.
Committed to cultural preservation.
The city values its cultural heritage and takes active steps to preserve and promote traditional customs, crafts, and arts.
Hosts an annual International Film Festival.
The Elektrostal International Film Festival attracts filmmakers and cinema enthusiasts from around the world, showcasing a diverse range of films.
Encourages entrepreneurship and innovation.
Elektrostal supports aspiring entrepreneurs and fosters a culture of innovation, providing opportunities for startups and business development.
Offers a range of housing options.
Elektrostal provides diverse housing options, including apartments, houses, and residential complexes, catering to different lifestyles and budgets.
Home to notable sports teams.
Elektrostal is proud of its sports legacy, with several successful sports teams competing at regional and national levels.
Boasts a vibrant nightlife scene.
Residents and visitors can enjoy a lively nightlife in Elektrostal, with numerous bars, clubs, and entertainment venues.
Promotes cultural exchange and international relations.
Elektrostal actively engages in international partnerships, cultural exchanges, and diplomatic collaborations to foster global connections.
Surrounded by beautiful nature reserves.
Nearby nature reserves, such as the Barybino Forest and Luchinskoye Lake, offer opportunities for nature enthusiasts to explore and appreciate the region’s biodiversity.
Commemorates historical events.
The city pays tribute to significant historical events through memorials, monuments, and exhibitions, ensuring the preservation of collective memory.
Promotes sports and youth development.
Elektrostal invests in sports infrastructure and programs to encourage youth participation, health, and physical fitness.
Hosts annual cultural and artistic festivals.
Throughout the year, Elektrostal celebrates its cultural diversity through festivals dedicated to music, dance, art, and theater.
Provides a picturesque landscape for photography enthusiasts.
The city’s scenic beauty, architectural landmarks, and natural surroundings make it a paradise for photographers.
Connects to Moscow via a direct train line.
The convenient train connection between Elektrostal and Moscow makes commuting between the two cities effortless.
A city with a bright future.
Elektrostal continues to grow and develop, aiming to become a model city in terms of infrastructure, sustainability, and quality of life for its residents.
In conclusion, Elektrostal is a fascinating city with a rich history and a vibrant present. From its origins as a center of steel production to its modern-day status as a hub for education and industry, Elektrostal has plenty to offer both residents and visitors. With its beautiful parks, cultural attractions, and proximity to Moscow, there is no shortage of things to see and do in this dynamic city. Whether you’re interested in exploring its historical landmarks, enjoying outdoor activities, or immersing yourself in the local culture, Elektrostal has something for everyone. So, next time you find yourself in the Moscow region, don’t miss the opportunity to discover the hidden gems of Elektrostal.
Q: What is the population of Elektrostal?
A: As of the latest data, the population of Elektrostal is approximately XXXX.
Q: How far is Elektrostal from Moscow?
A: Elektrostal is located approximately XX kilometers away from Moscow.
Q: Are there any famous landmarks in Elektrostal?
A: Yes, Elektrostal is home to several notable landmarks, including XXXX and XXXX.
Q: What industries are prominent in Elektrostal?
A: Elektrostal is known for its steel production industry and is also a center for engineering and manufacturing.
Q: Are there any universities or educational institutions in Elektrostal?
A: Yes, Elektrostal is home to XXXX University and several other educational institutions.
Q: What are some popular outdoor activities in Elektrostal?
A: Elektrostal offers several outdoor activities, such as hiking, cycling, and picnicking in its beautiful parks.
Q: Is Elektrostal well-connected in terms of transportation?
A: Yes, Elektrostal has good transportation links, including trains and buses, making it easily accessible from nearby cities.
Q: Are there any annual events or festivals in Elektrostal?
A: Yes, Elektrostal hosts various events and festivals throughout the year, including XXXX and XXXX.
Was this page helpful?
Our commitment to delivering trustworthy and engaging content is at the heart of what we do. Each fact on our site is contributed by real users like you, bringing a wealth of diverse insights and information. To ensure the highest standards of accuracy and reliability, our dedicated editors meticulously review each submission. This process guarantees that the facts we share are not only fascinating but also credible. Trust in our commitment to quality and authenticity as you explore and learn with us.
Share this Fact:
Read our research on: Gun Policy | International Conflict | Election 2024
Regions & Countries
What public k-12 teachers want americans to know about teaching.
Illustrations by Hokyoung Kim

At a time when most teachers are feeling stressed and overwhelmed in their jobs, we asked 2,531 public K-12 teachers this open-ended question:
If there’s one thing you’d want the public to know about teachers, what would it be?
We also asked Americans what they think about teachers to compare with teachers’ perceptions of how the public views them.
Related: What’s It Like To Be a Teacher in America Today?

Pew Research Center conducted this analysis to better understand what public K-12 teachers would like Americans to know about their profession. We also wanted to learn how the public thinks about teachers.
For the open-end question, we surveyed 2,531 U.S. public K-12 teachers from Oct. 17 to Nov. 14, 2023. The teachers surveyed are members of RAND’s American Teacher Panel, a nationally representative panel of public K-12 school teachers recruited through MDR Education. Survey data is weighted to state and national teacher characteristics to account for differences in sampling and response to ensure they are representative of the target population.
Overall, 96% of surveyed teachers provided an answer to the open-ended question. Center researchers developed a coding scheme categorizing the responses, coded all responses, and then grouped them into the six themes explored in the data essay.
For the questions for the general public, we surveyed 5,029 U.S. adults from Nov. 9 to Nov. 16, 2023. The adults surveyed are members of the Ipsos KnowledgePanel, a nationally representative online survey panel. Panel members are randomly recruited through probability-based sampling, and households are provided with access to the Internet and hardware if needed. To ensure that the results of this survey reflect a balanced cross section of the nation, the data is weighted to match the U.S. adult population by gender, age, education, race and ethnicity and other categories.
Here are the questions used for this analysis , along with responses, the teacher survey methodology and the general public survey methodology .
Most of the responses to the open-ended question fell into one of these six themes:
Teaching is a hard job
About half of teachers (51%) said they want the public to know that teaching is a difficult job and that teachers are hardworking. Within this share, many mentioned that they have roles and responsibilities in the classroom besides teaching, which makes the job stressful. Many also talked about working long hours, beyond those they’re contracted for.
“Teachers serve multiple roles other than being responsible for teaching curriculum. We are counselors, behavioral specialists and parents for students who need us to fill those roles. We sacrifice a lot to give all of ourselves to the role as teacher.”
– Elementary school teacher
“The amount of extra hours that teachers have to put in beyond the contractual time is ridiculous. Arriving 30 minutes before and leaving an hour after is just the tip of the iceberg. … And as far as ‘having summers off,’ most of August is taken up with preparing materials for the upcoming school year or attending three, four, seven days’ worth of unpaid development training.”
– High school teacher
Teachers care about their students
The next most common theme: 22% of teachers brought up how fulfilling teaching is and how much teachers care about their students. Many gave examples of the hardships of teaching but reaffirmed that they do their job because they love the kids and helping them succeed.

“We are passionate about what we do. Every child we teach is important to us and we look out for them like they are our own.”
– Middle school teacher
“We are in it for the kids, and the most incredible moments are when children make connections with learning.”
Teachers are undervalued and disrespected
Some 17% of teachers want the public to know that they feel undervalued and disrespected, and that they need more public support. Some mentioned that they are well-educated professionals but are not treated as such. And many teachers in this category responded with a general plea for support from the public, which they don’t feel they’re getting now.
“We feel undervalued. The public and many parents of my students treat me and my peers as if we do not know as much as they do, as if we are uneducated.”
“The public attitudes toward teachers have been degrading, and it is making it impossible for well-qualified teachers to be found. People are simply not wanting to go into the profession because of public sentiments.”
Teachers are underpaid
A similar share of teachers (15%) want the public to know that teachers are underpaid. Many teachers said their salary doesn’t account for the effort and care they put into their students’ education and believe that their pay should reflect this.
“We are sorely underpaid for the amount of hours we work and the education level we have attained.”
Teachers need support and resources from government and administrators
About one-in-ten teachers (9%) said they need more support from the government, their administrators and other key stakeholders. Many mentioned working in understaffed schools, not having enough funding and paying for supplies out of pocket. Some teachers also expressed that they have little control over the curriculum that they teach.
“The world-class education we used to be proud of does not exist because of all the red tape we are constantly navigating. If you want to see real change in the classroom, advocate for smaller class sizes for your child, push your district to cap class sizes at a reasonable level and have real, authentic conversations with your child’s teacher about what is going on in the classroom if you’re curious.”
Teachers need more support from parents
Roughly the same share of teachers (8%) want the public to know that teachers need more support from parents, emphasizing that the parent-teacher relationship is strained. Many view parents as partners in their child’s education and believe that a strong relationship improves kids’ overall social and emotional development.

“Teachers help students to reach their potential. However, that job is near impossible if parents/guardians do not take an active part in their student’s education.”
How the U.S. public views teachers
While the top response from teachers in the open-ended question is that they want the public to know that teaching is a hard job, most Americans already see it that way. Two-thirds of U.S. adults say being a public K-12 teacher is harder than most other jobs, with 33% saying it’s a lot harder.
And about three-quarters of Americans (74%) say teachers should be paid more than they are now, including 39% who say teachers should be paid a lot more.
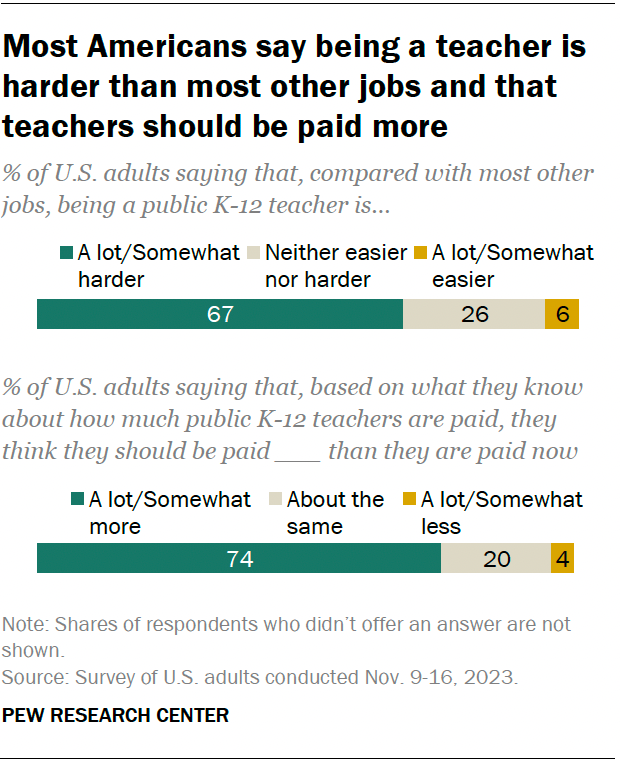
Americans are about evenly divided on whether the public generally looks up to (32%) or down on (30%) public K-12 teachers. Some 37% say Americans neither look up to or down on public K-12 teachers.

In addition to the open-ended question about what they want the public to know about them, we asked teachers how much they think most Americans trust public K-12 teachers to do their job well. We also asked the public how much they trust teachers. Answers differ considerably.
Nearly half of public K-12 teachers (47%) say most Americans don’t trust teachers much or at all. A third say most Americans trust teachers some, and 18% say the public trusts teachers a great deal or a fair amount.
In contrast, a majority of Americans (57%) say they do trust public K-12 teachers to do their job well a great deal or a fair amount. About a quarter (26%) say they trust teachers some, and 17% say they don’t trust teachers much or at all.
Related: About half of Americans say public K-12 education is going in the wrong direction
How the public’s views differ by party
There are sizable party differences in Americans’ views of teachers. In particular, Democrats and Democratic-leaning independents are more likely than Republicans and Republican leaners to say:
- They trust teachers to do their job well a great deal or a fair amount (70% vs. 44%)
- Teaching is a lot or somewhat harder when compared with most other jobs (77% vs. 59%)
- Teachers should be paid a lot or somewhat more than they are now (86% vs. 63%)
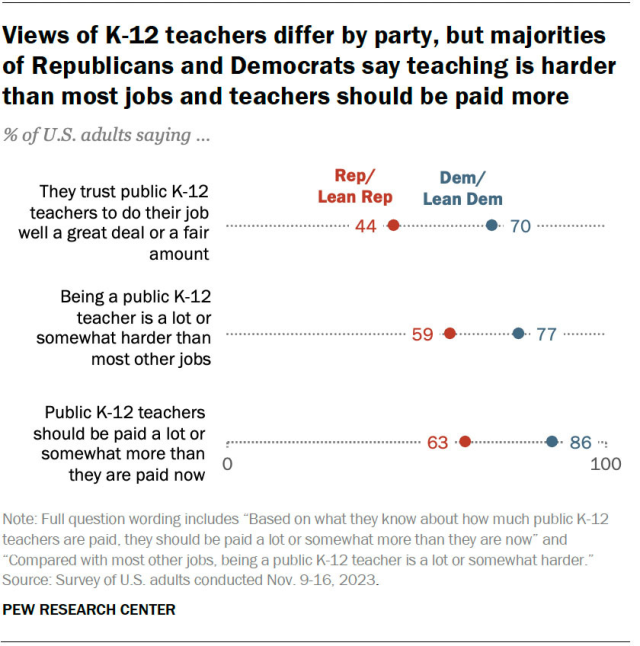
In their own words
Below, we have a selection of quotes that describe what teachers want the public to know about them and their profession.
Social Trends Monthly Newsletter
Sign up to to receive a monthly digest of the Center's latest research on the attitudes and behaviors of Americans in key realms of daily life
About Pew Research Center Pew Research Center is a nonpartisan fact tank that informs the public about the issues, attitudes and trends shaping the world. It conducts public opinion polling, demographic research, media content analysis and other empirical social science research. Pew Research Center does not take policy positions. It is a subsidiary of The Pew Charitable Trusts .
IMAGES
VIDEO
COMMENTS
Content last reviewed March 2023. Agency for Healthcare Research and Quality, Rockville, MD. Health systems research provides evidence that, when applied can make healthcare affordable, safe, effective, equitable, accessible, and patient-centered. AHRQ invests in research to generate new evidence to help health care systems and health care ...
This systems approach, in combination with stakeholder engagement, also informs the definition of priority research questions to address health systems challenges. Health systems research by necessity is highly multidisciplinary, with a strong emphasis on social sciences, economics, and anthropological investigations, for example on community ...
Here, we'll explore a variety of healthcare-related research ideas and topic thought-starters across a range of healthcare fields, including allopathic and alternative medicine, dentistry, physical therapy, optometry, pharmacology and public health. NB - This is just the start….
Introduction. The field of Health Policy and Systems Research (HPSR) is currently experiencing an unprecedented level of interest. The First Global Symposium on Health Systems Research, held in Montreux, Switzerland, in November 2010, is the most recent of a succession of conferences and task force deliberations that have spun off a series of debates about the nature of the field and the ...
Overview. Health policy and systems research (HPSR) is an emerging field that seeks to understand and improve how societies organize themselves in achieving collective health goals, and how different actors interact in the policy and implementation processes to contribute to policy outcomes. By nature, it is inter-disciplinary, a blend of ...
Health policy and systems research (HPSR) has changed considerably over the last 20 years, but its main purpose remains to inform and influence health policies and systems. Whereas goals that underpin health systems have endured - such as a focus on health equity - contexts and priorities change, research methods progress, and health organisations continue to learn and adapt, in part by ...
Table 3 Priority research questions in three health policy and systems areas, ... Symposium on Health Systems Research held in Montreux, Switzerland, in 2010: we need to mobilise the power of ideas in order to influence the ideas of power, that is to say, the ideas of those
Health policy and systems research (HPSR) is led by questions that are said to be "bubbling up from the field" (1). Indeed, these questions are about real-world policies, programmes, services and health systems arrangements (2), and they usually take the whole health system into account. At the same time, the process of refining the questions needs to be systematic and explicit. The ...
Health systems research addresses health system and policy questions that are not disease-specific but concern systems problems that have repercussions on the performance of the health system as a whole. It addresses a wide range of questions, from health financing, governance, and policy to problems with structuring, planning, management ...
This is the first of a series of three papers addressing the current challenges and opportunities for the development of Health Policy and Systems Research (HPSR). HPSR is a multidisciplinary and interdisciplinary field identified by the topics and scope of questions asked rather than by methodology. The focus of discussion is HPSR in low- and ...
The WHO evidence synthesis, published as a HEN report [], provides a firm basis for decision-making by policy-makers and research leaders looking to strengthen the health research system in their country.It identifies five crucial policy approaches that can be applied as appropriate to the context of the country - conducting situation analyses, sustaining a comprehensive strategy, engaging ...
An effective, high-performing public health system requires current, relevant, and reliable research to inform public health practice strategies. The need for funding and support to strengthen the evidence-base to guide and evaluate system improvements remains imperative, creating inspiration for an updated research agenda for the field of ...
Research Steps/Process Flowchart Some Closed Researches With Health System Research Either before or after the conception of Health System Research, Health Services Research-1972, Health Policy ...
3 answers. Jun 2, 2015. We conducted a study to estimate the economic burden of ADHD in United States using the Medical Expenditure Panel Survey (national survey by Agency of Healthcare Research ...
Overview. This comprehensive guide to health research reaches out to a wide spectrum of people: students who wish to learn the basic principles of health research and how to conduct it, field researchers, and those involved in teaching and training of health research methodologies. It seeks to develop practical skills, starting with defining ...
The Role of Health Services Research in Advances in Cancer Prevention and Control, sponsored by Department of Public Health Sciences, University of Virginia School of Medicine. ... Special Issue on Age-Friendly Health Systems Health Services Research and The John A. Hartford Foundation have partnered to publish a special issue on Age-Friendly ...
Patients not having access to their electronic health record portals was also a commonly reported challenge (109/511, 21.3% in 2020 and 137/615, 22.3% in 2021, P=.73). Conclusions: During the pandemic, our health care delivery system rapidly adopted synchronous patient-clinician communication using video visits.
The research advocates for a more holistic approach to mental health intervention, emphasizing the importance of considering adolescents' experiences of interpersonal racial discrimination ...
Evolution of a Question-Driven Field. Compared to other health research traditions, HPSR has a short but eclectic history. Many of the researchers who have led its development have brought social science perspectives, including health economics, sociology, political science, and anthropology, complementing the contributions of individuals and institutions engaged in delivering health services.
TBICoE unifies a system of TBI health care, reliably advancing the science for the warfighter and ready to meet future brain health challenges. ... Military Health Topics All Topics ... (TBICoE) aligns with the other centers of excellence within the Defense Health Agency's Research and Development Directorate, under which the TBICoE operates ...
New way to generate human cartilage Date: April 10, 2024 Source: The University of Montana Summary: University of Montana researchers and their partners have found a new method to generate human ...
As part of the initiative, Pang et al. developed a conceptual framework to guide the analysis and strengthening of health research systems, including development of a health research strategy. While this can be used for planning, monitoring and evaluation of health research systems, it did not claim to provide a precise blueprint.
UNCLASSIFIED//FOR OFFICIAL USE ONLY UNCLASSIFIED//FOR OFFICIAL USE ONLY Incident Observations (U) Tactics & Techniques: -(U) Attackers: Two female suicide bombers (one per train). -(U) Device: Explosive belts packed with plastic explosives: one per bomber; may have contained hexogen (RDX) as well as chipped iron rods and screws; believed to have been set off on the trains as the trains ...
The index for the Burevestnik space complex is 14K168. The idea that "293" is a satellite launch vehicle is corroborated by the fact that the index for one of its stages (14S47) is similar to that of some upper stages of space launch vehicles. Moreover, plans to use the MiG-31 as a satellite launch platform are not new.
Four members of UT Austin's Academic Affairs community presented at a recent The University of Texas System conference hosted by UT San Antonio's Office of Academic Innovation.Strategic Academic Initiatives postdoctoral fellows Natalie Murray, PhD, and Raj Sankaranarayanan, PhD, Kory Bieg, associate professor and associate dean of Academic Affairs in the School of Architecture, and Julie ...
40 Facts About Elektrostal. Elektrostal is a vibrant city located in the Moscow Oblast region of Russia. With a rich history, stunning architecture, and a thriving community, Elektrostal is a city that has much to offer. Whether you are a history buff, nature enthusiast, or simply curious about different cultures, Elektrostal is sure to ...
Overall, 96% of surveyed teachers provided an answer to the open-ended question. Center researchers developed a coding scheme categorizing the responses, coded all responses, and then grouped them into the six themes explored in the data essay. For the questions for the general public, we surveyed 5,029 U.S. adults from Nov. 9 to Nov. 16, 2023.
Saint-Petersburg Research Institute of Radiation Hygiene after Professor P.V. Ramzaev, Federal Service for Surveillance on Consumer Rights Protection and Human W ell-Being, Saint-Petersburg, Russia